
Abstract
Intramuscular lipomas, typically found in subcutaneous tissue, rarely affect deeper muscular planes, especially those of the head and neck region. The following are 3 cases of intramuscular lipomas involving the sternocleidomastoid muscle. The first 2 patients presented with painless, palpable masses confirmed by diagnostic imaging as well-circumscribed intramuscular lipomas. One was treated surgically, while the other was managed conservatively with monitoring and close follow-up. The third patient reported dysphagia associated with occasional dyspnea and mild pain. The mass was identified as infiltrative lipoma and was resected surgically. Complete tumor removal with no recurrence at 6 months was observed for the first and last cases. The second case was serially followed at 3 and 6 months with no interval changes. We report the largest case series on intramuscular lipomas of the sternocleidomastoid muscle to enhance our understanding of this rare entity.
Introduction
Benign lipomas are the most common type of soft-tissue neoplasms, characterized by mature adipose cells enclosed within thin fibrous capsules. While lipomas can develop anywhere on the body, they tend to occur superficially in the subcutaneous tissue. In rare cases, they may involve deeper muscular planes or the fascia. Lipomas are commonly present on the trunk and upper extremities and can have a round, oval, or multilobulated appearance. 1
Intramuscular lipomas account for less than 1% of all lipomas and occur more frequently in men than women. These tumors become exceedingly rare when occurring in the head and neck regions such as the sternocleidomastoid muscle (SCM), the larynx, and the tongue. The etiology of intramuscular lipomas is largely unknown, although they are thought to result from aberrant differentiation of mesenchymal cells. 2 Patients may clinically present with either an asymptomatic mass that causes only cosmetic concern or a painless, slowly growing mass that can cause discomfort and functional limitations depending on its location. When occurring in the head and neck region, common symptoms include a palpable mass, neck pain, and stiffness while in more severe cases, it can result in dysphagia and dyspnea. 3 The primary treatment for large intramuscular lipomas is surgical excision, while smaller lesions may be observed.
Case 1
A 52-year-old male patient presented to the otolaryngology clinic complaining of a left neck mass, stable in size for the past 5 years that recently started growing. He denied pain, skin changes, and swallowing or airway symptoms. On physical examination, an oval mass was palpated along the left SCM muscle. The mass was soft, non-tender to palpation, and measured 60 × 21 mm2 in size. The overlying skin showed normal color without erythema or inflammatory findings. Preoperative computed tomography (CT) scan showed a well-circumscribed non-enhancing fat-attenuating mass in the left side of the neck, suggestive of an intramuscular lipoma. There were no features of local tissue infiltration (Figure 1a). To confirm tissue diagnosis, a fine needle aspiration biopsy (FNA) was obtained which revealed mature fat cells consistent with lipoma. The physician opted to surgically remove the tumor because of its size and esthetic burden on the patient.
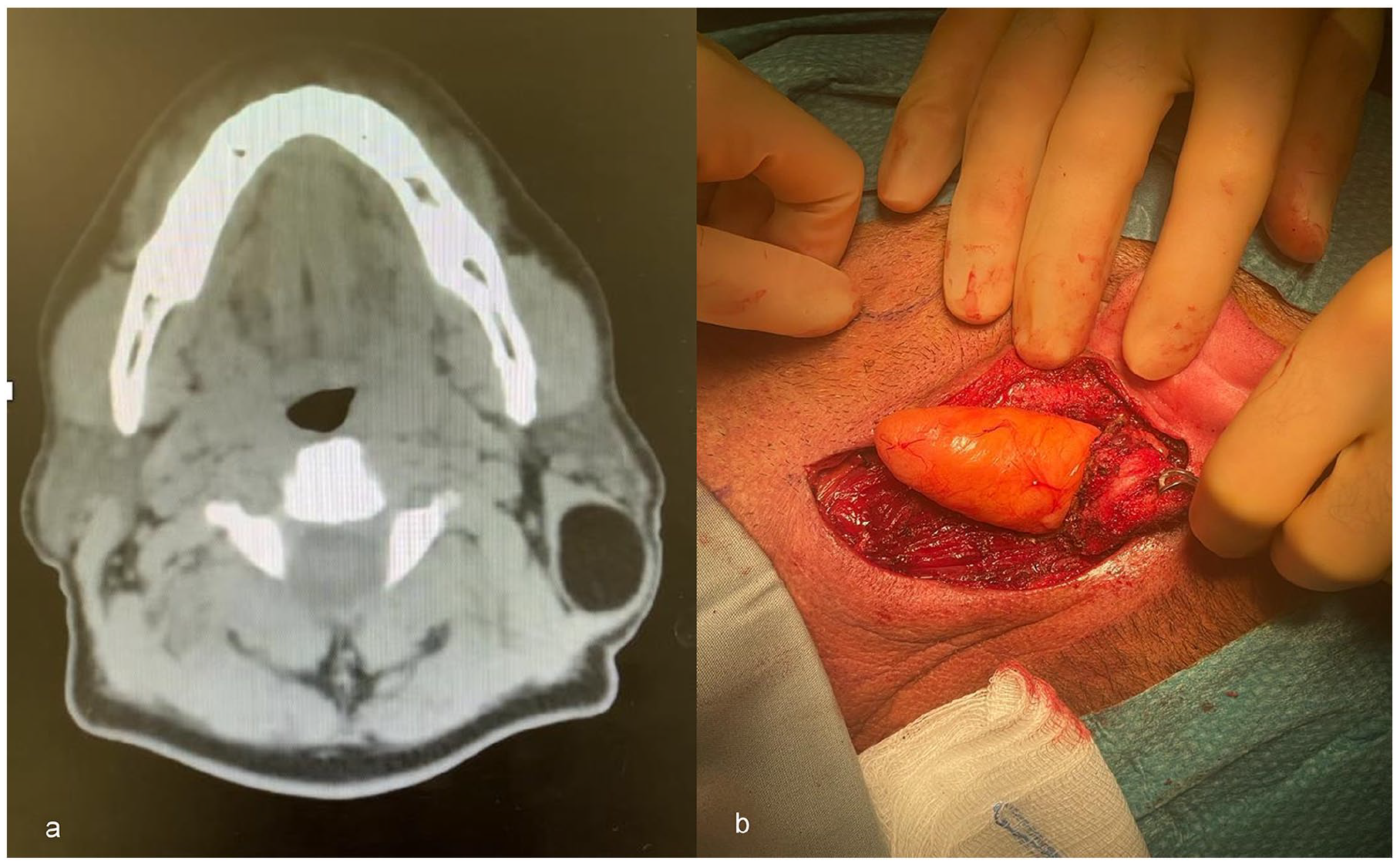
(a) Preoperative axial CT scan showing a well-circumscribed well-defined non-enhancing fat-attenuating mass in the left side of the neck; (b) Intraoperative image of the lipoma invading the SCM muscle and adhering to the muscle fascia.
Under general anesthesia, an incision was extended from the mastoid tip along the neck creases. Dissection through the skin, subcutaneous tissues, until the anterior border of the SCM muscle, revealed a lipoma focally invading the muscle and adhering to its fascia (Figure 1b). Careful dissection was achieved around the mass until adequately freeing all edges to achieve complete resection. On gross examination, the oval-shaped mass measured 6.5 × 2 × 2 cm3, with soft, bright-yellow homogenous fatty tissue, and a rubbery consistency. Histologic findings showed mature fat cells within muscle tissues. Cellular dysplasia, mitosis, necrosis, or excessive proliferation of blood vessels were not observed (Figure 2). At the last follow-up visit 6 months after the procedure, no recurrence of the mass was observed.

(a) Histologic appearance of an overall well circumscribed intramuscular lipoma with mature univacuolated adipocytes of fairly uniform size (H&E, X20); (b) Focal area of infiltration within the surrounding skeletal muscle (H&E, X40); (c) Desmin immunostaining to highlight the skeletal muscle.
Case 2
A 74-year-old male patient presented to the otolaryngology clinic for a left posterior triangle neck mass found incidentally 1 month before presentation. The patient reported mild pain, dysphagia to both solids and liquids, and occasional dyspnea without signs of respiratory distress such as stridor or cyanosis. On physical exam, a 10 cm mass was identified in the posterior triangle of the neck. It was soft, non-tender to palpation, with no overlying skin discoloration, and a preserved range of motion of the neck. Because of the presenting compressive symptoms, a preoperative CT scan was ordered, which showed an 11 × 7 × 7 cm3 mass within the SCM muscle. Magnetic resonance imaging (MRI) was further requested to rule out a sarcomatous component within the lesion because of its large size and unusual presentation. MRI revealed that the lesion is an intramuscular lipoma extending between neck level VB and the supraclavicular region, anteriorly limited by the SCM muscle (Figure 3a). Ultrasound-guided FNA confirmed that the tumor is consistent with benign adipose tissue as seen in lipoma. The patient was planned for surgical resection of the mass.
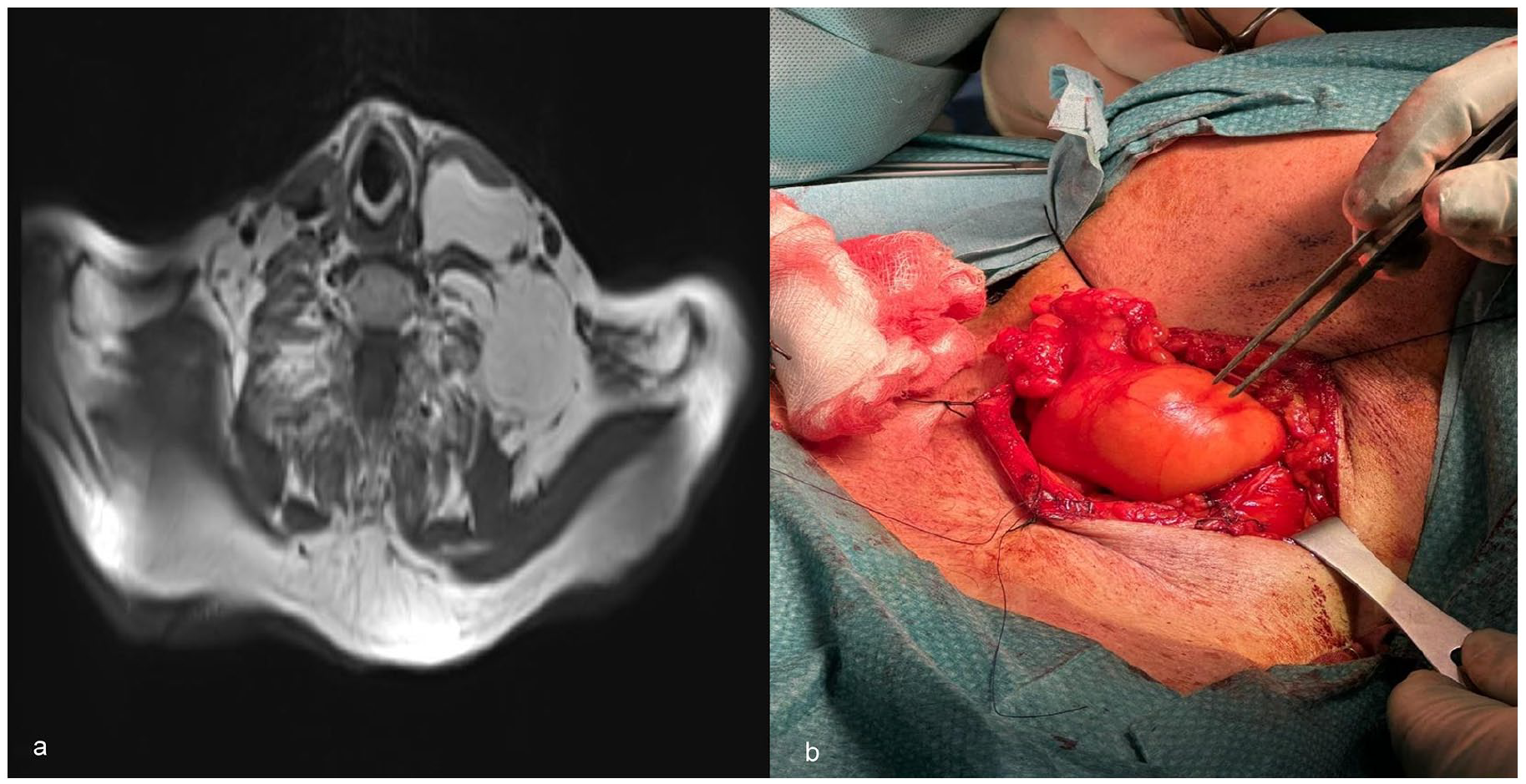
(a) T1-weighted MRI revealing an intramuscular lipoma extending between neck level VB and the supraclavicular region, anteriorly limited by the sternocleidomastoid muscle; (b) Intraoperative image of the lipoma invading the SCM muscle and adhering to the muscle fascia.
Under general anesthesia, a horizontal incision over the neck mass was designed along the skin crease extending from its posterior edge to the anterior edge of the SCM muscle. Dissections through the skin, subcutaneous tissues, external jugular vein, and SCM muscle were achieved to expose the lipoma, which was infiltrating the muscle. Careful dissection was carried out to free its borders circumferentially while keeping its capsule intact (Figure 3b). The mass was friable and was delivered in fragmented parts. A specimen was sent for pathological examination which revealed mature adipose tissue consistent with lipoma. No cytological atypia was identified in the multiple sections of the adipose neoplasm, ruling out liposarcoma. At 6-month follow-up visit, no recurrence of the mass was observed.
Case 3
A 38-year-old male patient presented to the otolaryngology clinic with a 3-month history of a left neck mass, stable in size. The patient denied neck pain, difficulty articulating, dysphagia, odynophagia, limitation in neck motion, and other systemic symptoms. On physical examination, there was a 2 × 2 cm2 bulge at the anterior upper third of the left SCM muscle. It was non-tender to palpation with no overlying skin changes. There was no trismus and no limitation in the range of motion of the neck.
Initial ultrasound imaging the presence of an intramuscular lesion, which required an MRI for better soft tissue assessment. MRI showed a well-circumscribed small lipoma (4 × 2 cm2), within the muscle planes, and lacking solid or nodular components. Only one faintly enhancing septum was detected with no high-grade features. The lesion was labeled as a low-grade lipomatous tumor confirmed by FNA.
Given the size, lack of symptoms, and benign nature of the mass, the decision was made to conservatively manage the tumor with monitoring and close follow-up. Serial follow-up visits at 3 and 6 months showed stable size of the mass with no interval changes.
Discussion
Intramuscular lipomas can be classified into 2 subtypes: infiltrative and well-circumscribed. Histologically, infiltrative lipomas exhibit a mass with an irregular distribution of uniform, mature, and uni-vacuolated adipocytes. In contrast, the well-circumscribed subtype consists of a discrete mass of uniform, mature adipocytes that are demarcated from the surrounding muscle tissue. 4 Both subtypes share common features such as the absence of nuclear atypia, scattered capillaries, muscle bundles within the fat lobules, and an incomplete fibrous capsule covering the tumor. 2 Intramuscular lipomas can be differentiated from liposarcomas by the absence of atypical cells or vacuolated lipoblasts admixed with fibroblast-like spindle cells, particularly within the septa, and by the presence of fewer and thinner fibrous septae with less prominent blood vessels. 5
The etiology and pathogenesis of intramuscular lipomas remain unknown although many theories have been suggested. Factors such as trauma, metabolic disorders, metaplasia, and chronic irritation may be implicated in the formation of lipomas. 6 Type-selective muscle fiber atrophy coupled with an increase in the lysosomal catabolic enzyme cathepsin D may be associated with the development of intramuscular lipoma, highlighting the potential link between local muscle atrophy and lipoma formation. 7 Another interesting theory is the fibrohistiocytic differentiation of cells in fatty tumors: CD34+ perimysial fibroblasts and interstitial dendritic cells appear to undergo an adipocytic transformation, contributing to the pathogenesis of intramuscular lipomas. 8 Moreover, an immunohistochemical study demonstrated that structures within the head and neck region are abundantly covered with CD34+ fibrous tissues, especially the parotid gland and the sternocleidomastoid muscle. 9 This can potentially explain how an intramuscular lipoma could have arisen within the SCM muscle.
FNA can serve as valuable tool in confirming the lipomatous nature of the lesion as well as differentiating benign from malignant tumors with a high diagnostic accuracy and more than 90% specificity. 10 The primary treatment for large intramuscular lipomas is surgical excision, with complete removal being the preferred approach to reduce the risk of recurrence. In other cases, where the mass is smaller, observation may be considered. These benign tumors have an excellent prognosis with a low risk of recurrence and malignant transformation following complete resection. 5
After exploring PubMed library, only 6 relevant reports on intramuscular lipomas of the SCM muscle were identified, the majority of which being infiltrative,6,11 -13 except for 2 which were well-circumscribed.14,15 (Table 1). These articles focused on the recurrence rate of these benign tumors and their differentiation from malignant liposarcoma. MRI features may help distinguish between the 2 pathologies; the presence of thick septa, a maximum tumor diameter of more than 13 cm, and contrast enhancement constitute solid predictors of well-differentiated liposarcoma. 16 Moreover, both disease entities exhibit acceptably low rates of local recurrence with high 10-year local recurrence-free survival rates of 95% and 81% for intramuscular lipoma and atypical lipomatous tumor, respectively. 17
Characteristics of the SCM intramuscular lipoma case reports mentioned in the literature and in the present series.

To the best of our knowledge, this is the largest series to date reporting on such a rare entity with 2 cases of well-circumscribed and 1 case of infiltrative intramuscular lipomas of the SCM muscle.
Conclusion
Intramuscular lipomas of the SCM muscle are rare benign tumors that occur in the neck region. Patients may present with an asymptomatic mass causing only cosmetic concern or a painless, slowly growing mass leading to discomfort and limited neck movement. In severe cases, the tumor can cause neck pain, stiffness, dysphagia, and dyspnea. Surgical excision is the primary treatment for larger intramuscular lipomas, aiming for complete removal to minimize the risk of recurrence. Smaller masses may be observed. The prognosis of intramuscular lipomas of the SCM muscle is excellent, with a low likelihood of recurrence or malignant transformation after successful resection.
Footnotes
Acknowledgements
None.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author contributions
All authors contributed to the study conception and design. Material preparation, data collection was performed by Jad Hosri, Yara Yammine, and Nadine El Hadi. The first draft of the manuscript was written by Jad Hosri and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Ethics Approval Statement
The American University of Beirut Institutional Review Board has determined that this is not a “Human Subject Research” and hence no ethical approval is required. Therefore, this article does not contain any studies with human participants performed by any of the authors.
Informed Consent
For this type of study, informed consent is not required.
Consent for Publication
Consent for publication was obtained for every individual person’s data included in the study.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.