
Abstract
Background:
Lipomas are the most common benign soft tissue tumors in the general population. These lesions can appear on any part of the body and usually develop in the subcutaneous superficial tissue. Lipomas that show ossifying changes are very rare, representing less than 1% of the reported lipomas. They usually manifest as hard nodular lesions in the head and neck, the extremities, the sternoclavicular region, and the subcutaneous tissue in general; they are rare in the costal arches.
Case presentation:
We report the case of a patient with a history of multiple diseases and 2 tumor-like lesions with internal lytic areas detected in the fourth right costal arch and in the eighth left costal arc; we describe his clinical manifestations, radiological and laboratory findings as well as the pathological results and outcome.
Conclusions:
Ossifying lipomas are rare benign tumors with asymptomatic clinical presentation. It is important to perform an adequate radiological differentiation from other more aggressive lesions such as liposarcomas.
Keywords
Background
Lipomas are the most common benign soft tissue tumors in the general population. They are characterized by the presence of mature adipocytes enclosed in thin fibrous capsules. These lesions can appear on any part of the body and usually develop in the subcutaneous superficial tissue, uncommonly involving the fascia or deep muscle planes. 1 Most tumors occur in adults aged 30 years or older, with the same incidence in both sexes. Lipomas that show ossifying changes are rare. 2 Other mesenchymal elements such as fibrous or smooth muscle, bone, or chondral tissue may be found occasionally in addition to adipocytes. 3 The latter are recognized as ossifying lipomas and chondroids, respectively. Less than 1% of lipomas were reported as ossifying in a study of 635 cases. 4
Ossifying lipomas are also known as osteolipomas, being able to use the 2 terms interchangeably. They have been documented in the head and neck area, lower extremities, the sternoclavicular region, and in subcutaneous soft tissues. 5 The clinical presentation of ossifying lipomas is usually asymptomatic and consequently, most cases are not diagnosed for years. 6 In addition, ossifying lipomas share clinical and radiological characteristics with other benign and malignant tumors. 7 For this reason, its presentation, besides being rare, results in a diagnostic challenge, which requires adequate histological characterization to differentiate it from other neoplasms with less favorable prognosis. The presentation of ossifying lipomas in the costal arches is exotic. We present the case of a patient with a history of multiple diseases and 2 tumor-like lesions with internal lytic areas detected in the fourth right and eighth left costal arches that due to their radiological characteristics, it was very difficult to define the involvement of the lung parenchyma and pleural space, with a subsequent excisional biopsy for study.
Case Presentation
A 61-year-old White man, non-smoker, with a diagnosis of long-standing arterial hypertension of difficult control, severe heart failure with a left ventricular ejection fraction of 30% receiving pharmacological treatment with carvedilol, ivabradine and losartan, and history of stage IIIB chronic renal failure without dialysis therapy. A year before the current admission, he consulted for urinary symptoms that rapidly evolved to systemic compromise with fever, diaphoresis, low back pain, hypotension, dyspnea, and increased acute phase reactants. He required hospitalization in the intensive care unit for multidisciplinary treatment with a diagnosis of sepsis of urinary origin. Alterations in calcium behavior were detected, which were associated to the underlying renal disease and to a severe hyperparathyroidism secondary to a functional adenoma in the lower left parathyroid treated with surgery, achieving control of symptoms and levels of calcium and phosphorus. Chest x-ray showed 2 lesions of tumor aspect with internal lytic areas in the fourth right and eighth left costal arches. The first lesion measured 25 × 21 mm with involvement of fourth right costal arch and the second measured 77 × 54 mm in eighth left costal arch showing growth toward the left pleural cavity (Figure 1). Both lesions were suggestive of a tumor of chondral origin, enchondroma, and as it was not possible to rule out malignancy with the images, he was admitted in our institution for excisional biopsy. The physical examination revealed a thin patient with chronic disease and a deformity in the neck with anterior flexion pronounced by severe dorsal kyphoscoliosis and secondary asymmetry of the right ribcage, which was retracted with decreased intercostal spaces. He referred increased dyspnea with the activities of daily life, with NYHA (New York Heart Association) functional class III. Blood pressure 120/70 mm Hg, heart rate 100 beats per minute, breathing frequency 16 breaths per minute, no cyanosis, with jugular engorgement at 90°, no neck masses, tachycardic rhythmic heart with no murmurs or gallop, decreased breath sounds at both lung bases, abdomen without ascites or masses, and extremities with edema grade II. No identifiable lesions in the chest wall other than deformity by kyphoscoliosis were found.
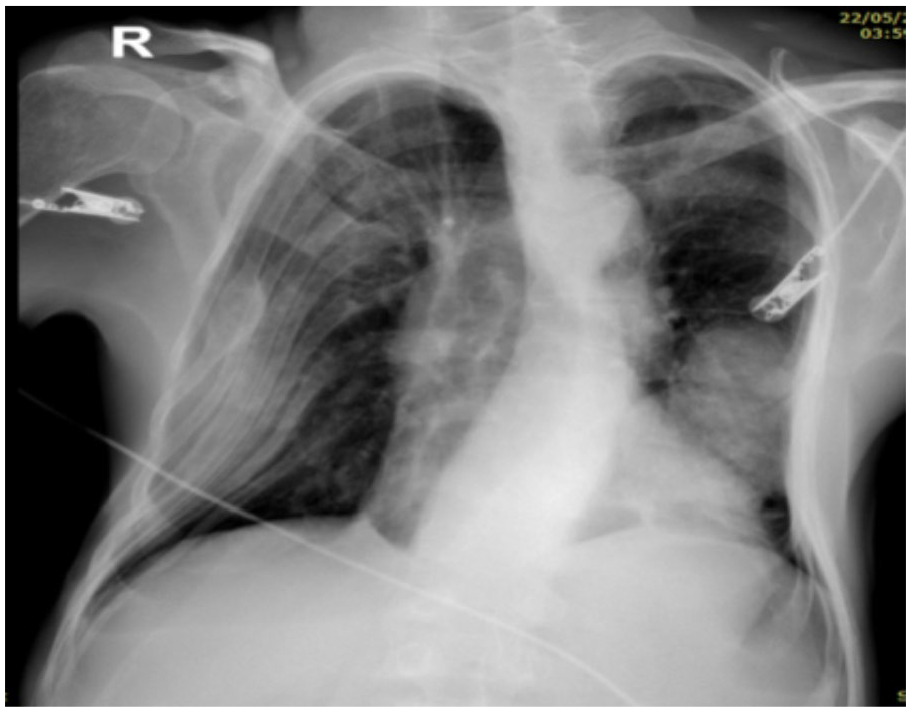
AP chest x-ray in decubitus position. On the base of the left hemithorax, a radiopaque image of lobed contours is projected, measuring approximately 88 × 56 mm. The expansion of the right hemithorax is diminished with a decrease in the intercostal spaces giving increased opacity of the lateral portion, possibly secondary to deformity of the ribcage.
Blood work was unremarkable, except for mild anemia of normal volumes (see Table 1), spirometry showed a moderate restrictive ventilatory pattern and no significant post-bronchodilator changes and diffusing capacity of carbon monoxide, in normal limits (diffusing capacity of the lungs for carbon monoxide [DLCO]: 109%). The chronic kidney disease was stable. Thoracic computed tomography (CT) scan showed a heterogeneous rounded lytic lesion with sclerotic edges and growth toward the pulmonary cavity, of expansive type, causing displacement of pulmonary parenchyma, and measuring approximately 77 × 54 mm and depending on the eighth left costal arch (Figure 2). Given the size and characteristics of the mass, it was very difficult to determine if the lung was surrounding the lesion or if the mass was in fact infiltrating the parenchyma. In addition, in the fourth right costal arch, an image of similar characteristics, but smaller in size, is found, measuring 25 × 21 mm. In addition, a severe dorsal kyphoscoliosis was identified. No further studies were implemented; the decision was made to perform a surgical resection of the mass with the possibility of having to do a lobectomy.
Summary of laboratory results.


Thoracic computed tomography scans, where the appearance of 2 bone lesions can be seen sequentially from A to F. The largest depends on the eighth left costal arch, is rounded, with a lithic component inside, with sclerotic edges, heterogeneous, that grows toward the pulmonary cavity and that in the initial cuts gives the impression of being an intraparenchymal mass, is of expansive type, measures approximately 77 × 54 mm. The second lesion is in the fourth right costal arch, it is an image of similar characteristics but smaller in size, measuring 25 × 21 mm, it has sclerotic edges and a lithic center. Other severe dorsal kyphoscoliosis and free pleural spaces are observed.
The patient was hospitalized in the intensive care unit for pre-surgical conditioning where a left ventricular ejection fraction of 30% was evidenced and a cycle of intravenous levosimendan was initiated. He received red blood cell transfusion and underwent resection of the left costal mass by thoracoscopy. During the surgical procedure, only 1 hard lesion was found that involved the eighth rib and soft tissues of the seventh to ninth left ribs, without infiltration into the lung tissue or pleural cavity. Therefore, only partial resection of these 3 ribs was necessary, without pulmonary lobectomy, the right side was not intervened. In the immediate postsurgical period, the patient presented a difficult evolution, with hemodynamic instability, required vasoactive support with norepinephrine, prolonged mechanical ventilation, and a need for a tracheostomy to assist a long-standing recovery process. Subsequently, it was possible to remove the vasoactive drugs, the invasive ventilatory support, and the tracheostomy with complete physical and respiratory rehabilitation.
Pathology Findings
The pathology reported morphological findings compatible with ossifying lipoma. The histological sections showed a benign neoplastic lesion constituted by mature adipose tissue delimited by a thin capsule of fibroconective tissue and proliferation of thin bone trabeculae throughout the tumor, without Medullary stroma and without other mesenchymal tissues within the mass (Figure 3A to D).
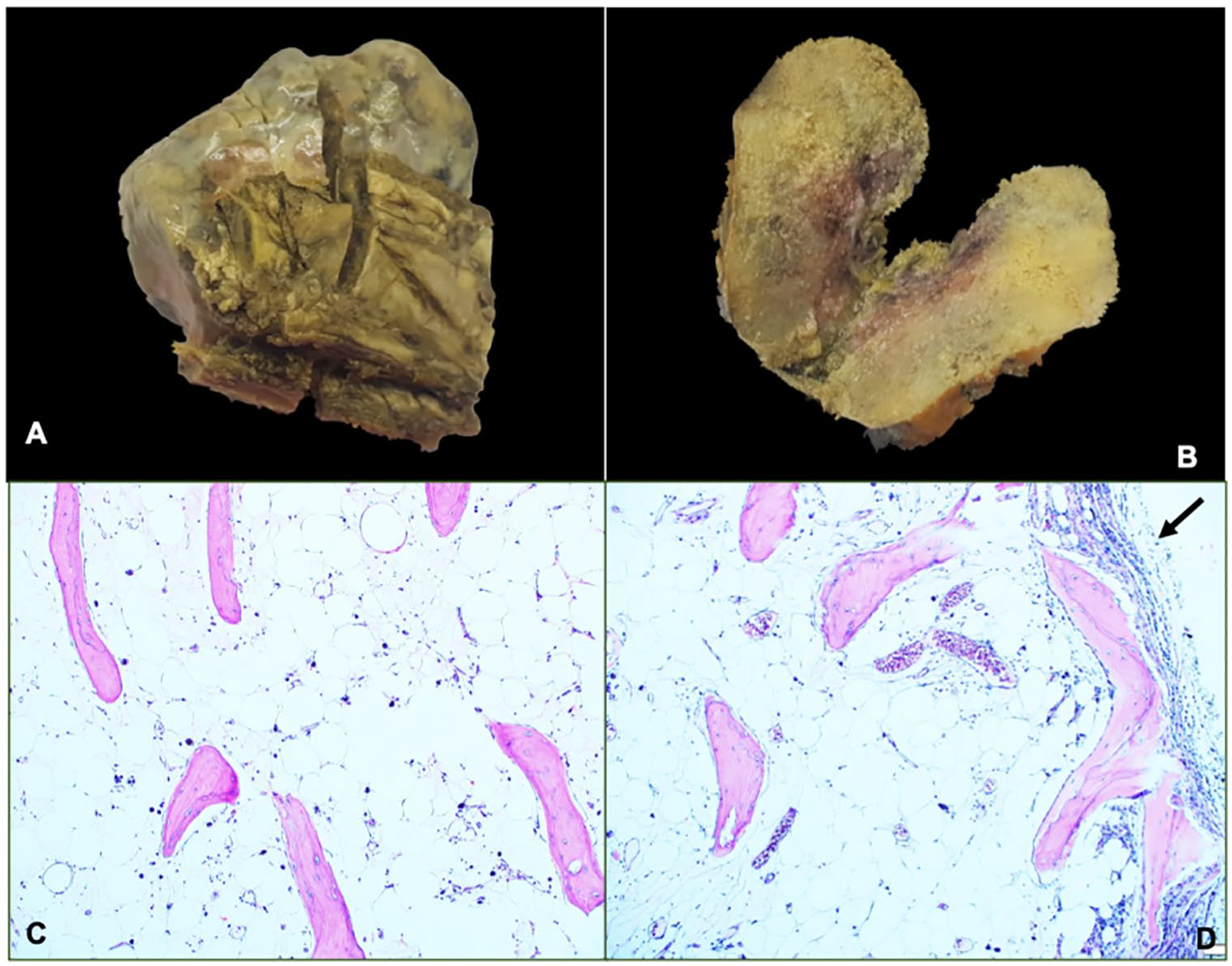
(A) Lobed mass that involves the seventh and eighth costal arch, the ninth costal arch that is free can also be seen. (B) On the macroscopic section, the aspect of spongy bone is appreciated. (C) Mature adipose tissue with bone trabeculae inside. (D) Involvement of the entire costal arch can be seen in the upper part (arrow).
After discussion with the patient and his family, and according to the histological characteristics of the tumor lesion, it was considered that chemotherapeutic treatment or other specific oncological interventions were not required, given the benign nature of the mass and its post excisional curative potential. The patient has continued in frequent control with several medical specialties including thoracic surgery specialty without evidence of recurrence of the lesions described.
Discussion and Conclusion
Lipomas are the most common benign soft tissue tumor. Among these, when they present ossification, they are known as ossifying lipomas, which are a much rare entity. It has been described in the literature that a non-depreciable percentage of patients with lipomas and ossifying lipomas present chromosome aberrations, specifically in the bands 12q13-15, being the most common translocation t(3;12) (q27-28; q14-15). These aberrations target the HMGA2 gene, thus presenting an alteration in lipogenesis and mesenchymal differentiation. However, evidence is yet to stablish if such chromosome rearrangements differ among primary and secondary ossifying lipomas. 8 Furthermore, ossifying lipomas have a short spectrum of differential diagnoses. Histological evaluation is the most useful tool to reach the definitive diagnosis of ossifying lipoma. Surgical excision is usually the treatment of this entity, 7 and its prognosis is the same as that of conventional lipomas. 6 In the case of our patient, multiple confusing factors existed that suggested as a first possibility another type of neoplastic lesion. Clinically, the patient revealed a marked weight loss, compromise of his functional class, and a recent history of another tumor lesion, the parathyroid adenoma, considering a possible malignant cause. However, it is important to clarify that the underlying diseases, especially the cardiac and renal failure played a very important role in explaining the general deterioration of the patient without involving the tumor lesion.
In addition, the presence of previous hyperparathyroidism raised suspicions of the possible relationship of this entity with the lesion that deformed and ossified the ribs. However, hyperparathyroidism and severe alteration of secondary calcium metabolism usually results in Brown tumors, which cause alterations in the trabecular bone pattern, demineralization, and replacement of bone tissue by connective tissue. Imaging shows single or multilocular radiolucency, bone deformities, which involve mainly the teeth and the jaw. Also, histologically it presents as a giant cell lesion. 9 In our case, the lesions were lytic in appearance, but did not present any of the other characteristics, thus we discarded the possibility of this mass being a Brown tumor. However, we do not reject the possibility of an association between hypercalcemia and ossification of prior lipomas, although in our knowledge, there is no report in the literature of such association.
There are 2 theories about the pathogenesis of ossifying lipomas, the first suggest that lipomas result from multidirectional differentiation of pluripotential mesenchymal cells. The mass contains the bone elements since its appearance. 10 This theory would explain why ossifying lipomas resemble benign mesenchymal tumors. The second theory proposes that they originate from the metaplasia of fibrous elements in bone tissue, secondary to an existing “classic” lipoma. This metaplasia can be a reactive change in response to several external factors such as mechanical stress, repeated trauma, or ischemia. 11 This last theory seems to fit the clinical context of our patient; unfortunately, it was not possible to have access to previous images to evaluate the evolution of the lesions over time. Both systemic hypoperfusion and metabolic imbalance (hyperparathyroidism) and serious infections (urinary sepsis followed by pulmonary sepsis) may have conditioned an abnormal healing process, which favors fibrous metaplasia in other unusual anatomical areas.
From a radiological perspective, it is possible to confuse an ossifying lipoma, which has by definition metaplastic bone, with a malignant lesion. On thoracic CT scans or magnetic resonance imaging (MRI), ossifying lipomas show intense and heterogeneous enhancement, which should raise suspicion of a soft tissue sarcoma and therefore the mass must be biopsied. 12 In our case, the radiological characteristics of the lesion of the fourth right costal arch with a rounded lytic image were highly suggestive of another type of benign lesion: an enchondroma. In addition, the image of the lesion in the eighth left costal arch, which gave the impression of involving, infiltrating, and collapsing the left lower lobe, forced us to consider a malignant transformation of an enchondroma. Therefore, the initial surgical intention was to perform a left lower pulmonary lobectomy, procedure not finally performed, when finding the lung and pleural cavity were not compromised.
Histological examination is considered the best approach to reach the definitive diagnosis of an ossifying lipoma. 13 These tumors typically present with diffuse mature adipose tissue and trabeculated bone. 14 During dissection, its macroscopic appearance is that of bone tissue. Microscopically, the mass resembles the bone marrow, with intraluminal microvasculature, erythrocytes, and leukocytes, as in mature bone. 15 In the case of our patient, the ossifying lipoma had the characteristic mature adipose tissue enclosed in a thin capsule of fibroconnective tissue and presented bone trabeculae inside. However, it lacked medullar stroma or other mesenchymal tissues inside the lesion.
Due to the poor knowledge of this benign lesion, it is advisable a long-term follow-up in these patients although the recurrence is very low; in an extensive literature review conducted by Rombado and Madewell 7 in 2018, relapses of this type of tumors have not been reported so far.
In conclusion, ossifying lipomas are rare benign tumors with asymptomatic clinical presentation. It is important to perform an adequate radiological differentiation from other more aggressive lesions such as liposarcomas. In case of doubts in the diagnosis with imaging, the size of the lesion is large or generates anatomical alterations or when there is a confusing clinical scenario, as in the present case, histological diagnosis is essential. In this situation, an excisional biopsy not only guarantees a definitive diagnosis but also results in a potentially curative treatment.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
All authors have significantly contributed to the article: AT: Conception and design, literature review, manuscript writing and correction, final approval of manuscript. NMS: Conception and design, literature review, final approval of manuscript. MV: Conception and design, literature review, final approval of manuscript. EM: Conception and design, literature review, final approval of manuscript. LFT: Conception and design, literature review, manuscript writing and correction, final approval of manuscript.
Availability of Data and Materials
All data and material are available for sharing if needed.
Consent for Publication
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
Ethical Approval and Consent to Participate
This report was prepared in accordance with the ethical standards of the institutional ethics committee and with the 1964 Helsinki Declaration. We have approval letter of Ethics Committee in biomedical research IRB/EC No. 305-2019 of the Fundación Valle del Lili to publish this manuscript.