
Abstract
The differential diagnosis of cystic echinococcosis should be considered in the suspected case of a pelvic mass presenting with vague symptoms. Primary pelvic hydatid cyst is rare, and the achievement of early diagnosis is important, as the involvement of bone in the pelvis is difficult to treat, and the probability of recurrences is greater. This case report presents a rare case of a primary pelvic hydatid cyst in a male in his 30s. The patient presented vague symptoms of difficulty in micturition and chronic pelvic pain. First-line radiological imaging techniques diagnosed it as a neoplastic mass and tuberculosis, while MRI revealed it as a cystic disease, probably a hydatid cyst. Surgical excision and histopathological examination confirmed the diagnosis of a primary pelvic hydatid cyst. Acquaintance with the varied presentation of cystic echinococcosis helps to obtain an accurate diagnosis and thus decreases the severe complication associated with the disease. This case report highlights the importance of considering parasitic infections in the differential diagnosis of cystic pelvic masses, even in regions with low endemicity.
Introduction
Echinococcosis is an infectious disease caused by parasitic tapeworms of the Echinococcus genus. It is prevalent in parts of Europe, Asia, Africa, South America, and Australia. Rural and pastoral communities, especially those involved in livestock farming, are at a higher risk due to their close proximity to infected animals. Human infection occurs through the ingestion of Echinococcus eggs present in contaminated food, water, soil, or by direct contact with infected animals. The parasite has a complex lifecycle, involving definitive hosts like dogs and intermediate hosts like humans. Infection occurs through ingestion of parasite eggs, leading to cyst formation, primarily in the liver and lungs.1 -3 Unusual sites of infection are fallopian tubes, broad ligament, kidney, musculoskeletal system, and pelvic region, often leading to delayed diagnosis, misdiagnosis, and severe complications. 4 The location of the pelvic region is rare, with an incidence of 0.5% to 2%, and the clinical presentation can mimic other diseases, such as tuberculosis and neoplastic conditions. Diagnosis can be challenging due to nonspecific symptoms and the lack of specific serological tests.2,3 Treatment of these patients poses a greater risk and is associated with morbidity and mortality. 5 We report a case of osseous hydatidosis in the pelvic region with differential diagnosis of tuberculosis and neoplastic mass. While echinococcosis is not currently a pandemic threat, its prevalence and distribution can still evolve within endemic regions due to factors like changes in animal populations and human activities.
Case Presentation
A male in his 30s presented to the outpatient department with chronic pelvic pain for the past 6 months. He is not a resident of rural or pastoral area. His occupation doesn’t involve any working with animals. He owns 1 dog that roam freely at his residence. He admits that his dog is not regularly dewormed. His dietary practices, includes the consumption of meat, raw vegetables, and fruits. He denied any travel history to endemic regions and history of trauma, weight loss, or other constitutional symptoms. The family history shows that his father had pulmonary tuberculosis 5 years ago. A detailed medical history was obtained, including information on the nature, duration, and location of the pain. The pain was intermittent, dull in nature and located in the lower abdomen and pelvic region. The patient also complains of difficulty in micturition and intermittent low-grade fever for 6 months. Informed consent was obtained from the patient. Physical examination revealed mild tenderness in the suprapubic region without palpable masses or lymphadenopathy.
Initial laboratory investigations were conducted during the first visit, including complete blood count, liver and kidney function tests, and serological tests for tuberculosis. Chest X-ray and abdominal ultrasound was performed. Chest X-ray was normal and ultrasound revealed a cystic mass in the pelvis. Initial diagnostic imaging revealed the absence of lesion in areas prone to echinococcal infection like lungs and liver. The patient returns for a follow-up visit to discuss the test results after 2 days (second visit). Laboratory investigations, including blood and serological tests, show no significant abnormalities. Peripheral blood eosinophil count and IgE levels was not elevated. ELISA for echinococcus antibodies was negative. The patient’s symptoms persist and the cystic lesion remains unexplained. X-ray and computed tomography (CT) scan of the abdomen and pelvis are ordered to obtain further information about the lesion.
The patient returns for a review of the results of the X-ray and CT scan after 4 days (third visit). The pelvis shows the presence of an osteolytic lesion in the entire right acetabulum, the right femoral head, and the right sacral foramina. Multidetector computed tomography (MDCT) scan of both hip joints shows a high density of soft tissue in the presacral space, displacing the pelvic viscera. It was also associated with bone erosions in the right acetabulum, right femoral head, right sacral foramina, and mild effusion of the right hip joint.
The findings of the MDCT scan suggested a neoplastic pelvic mass such as a schwannoma or chordoma. The need for further investigation and a possible surgical intervention was considered. Biopsy and magnetic resonance imaging (MRI) was also advised. MRI shows the presence of a cystic lesion in the pelvis and deep gluteal space that favors the most likely osseous hydatid disease and the less likely possibility of tubercular osteomyelitis with periosseous abscess (Figure 1).
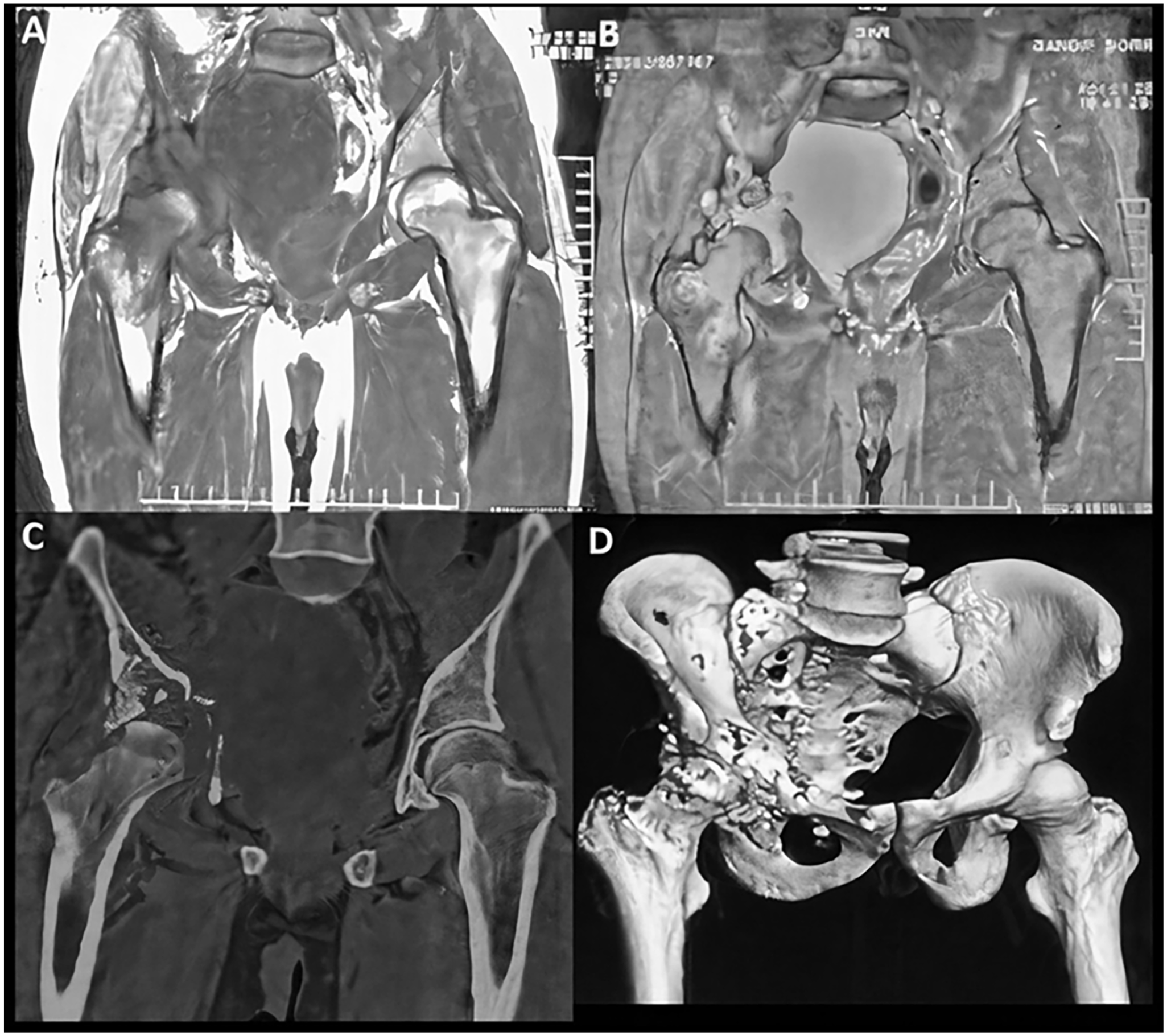
Magnetic resonance imaging (MRI) T1 and T2FS coronal images showing cystic mass in right side of pelvis involving right acetabular rim and extending to right hip joint with involvement of head, neck, and greater trochanter of the right femur (A and B). Computed Tomography (CT) coronal image (C) and VRT (Volume Rendered technique) image (D) showing osseous erosions involving right acetabular rim, right superior pubic ramus, proximal part of right femur, and right sacral ala.
The differential diagnosis for a cystic pelvic mass in this patient can be tuberculosis: Tuberculous involvement of the pelvis can present with chronic pelvic pain, abscess formation, and lymphadenopathy. However, the absence of constitutional symptoms, normal laboratory investigations, and lack of characteristic imaging findings made tuberculosis less likely in this case. Pelvic neoplasms, such as schwannoma, chordoma, can present with similar symptoms. However, the presence of a cystic lesion on MRI reduces the probability of a neoplastic mass. No other organ was involved, as revealed by the MRI, and hence the diagnosis of Hydatid disease was made.
Treatment and outcome: After 5 days the patient underwent an exploratory laparotomy for further evaluation and management. The intraoperative findings revealed a large cystic mass arising from the pelvic region. Surgical excision of the cyst was performed and the postoperative period was uneventful. Histopathological examination of the excised specimen was carried out.
Pathological Findings
Gross examination revealed the presence of pearly gelatinous cystic cavities with thick pasty material (Figure 2). Microscopic examination shows a thick laminated cyst wall layer, inner germinal layer, and occasional daughter cysts. Also detached protoscolices noted (Figure 3). “Hydatid sand” was observed. Secondary changes in the form of necrosis noted (Figure 4). The diagnosis of primary pelvic hydatid disease was confirmed by histopathology. As per literature presence of protoscolex in histopathology sections is itself diagnostic of Hydatid cyst and hence special stain and Immunohistochemistry was not required in the present study.

Gross section of hydatid cyst: large hydatid cyst with daughter cyst.

Section showing the protoscolex of the hydatid larva (long arrow) with the acellular germinal layer (short arrow). H&E, 10X.
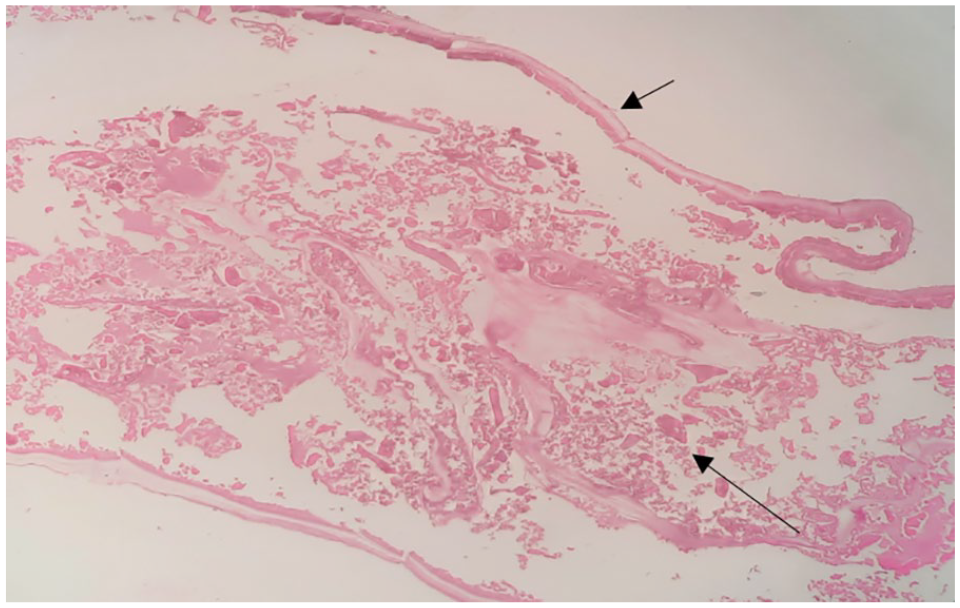
Section showing lamellated membrane (short arrow) along with areas of necrosis (long arrow). H&E, 10X.
No evidence of clinical recurrence of the disease was found on the imaging found at monthly follow-up for 6 months.
Discussion
The causal agent for hydatid disease belongs to the species Echinococcus. The definitive hosts are dogs, while sheep, cattle, and goats are intermediate hosts.1,3 Humans are accidentally infected by ingestion of eggs from the feces of definitive hosts. 1 Eggs infect different organs of the body through blood and lymphatics. Here, the eggs grow to form a hydatid cyst. Symptoms occur when the cysts enlarge to the point to cause them. It may take several years for symptoms to develop after initial exposure.2,4 The disease is prevalent in the Mediterranean region, Australia, Africa, and some parts of Northern and Central India. 6
Ertem 7 and Palanivelu et al 8 reported that 30 to 40 years is a common age of presentation as seen in our study. Tekin et al 9 reported an increase in female prevalence, however, Palanivelu et al 8 reported male predominance 5 times more than female, similar to the present study. The younger population is commonly affected by the disease. One of the reasons for the same is increased participation in activities such as agriculture and animal breeding.10,11
The most common sites involved in the hydatid cyst are the liver and lungs. Other sites are kidney, spleen, muscles, ovaries, omentum. Bone and pelvis are exceptional sites of echinococcosis. 12 Pelvic hydatid disease is rare and can be primary or secondary. Secondary pelvic hydatid disease usually occurs due to rupture of the hydatid cyst of the liver or lung. Primary pelvic hydatid disease is extremely rare with an incidence of only 0.2% to 2%.12,13 The pathophysiology is not clearly rooted in pelvic inclusion due to echinococcosis. There are several theories that the pelvis is involved in a hematogenous and lymphatic way. 12 Bone erosion associated with pelvic disease can be due to ischemia due to obstruction or compression of blood vessels, pressure atrophy of the bone, or osteoclast proliferation around compressed bone. 5
In our study patient presented with chronic pelvic pain with difficulty in micturition. Patients with primary pelvic hydatid disease have no specific symptoms. They often present with pressure symptoms such as obstructive uropathy, constipation, and menstrual irregularities. They may present with secondary infection, such as an abscess or an allergic reaction due to rupture of the cyst and release of fluid in the adjacent area.11,12
Diagnosis is challenging in such cases as routine laboratory investigations are usually within the normal limit. Serological tests must be interpreted considering other factors such as clinical characteristics, epidemiology, and radiological imaging techniques.2,5 In our case, initial laboratory investigations, including blood tests, serological tests for tuberculosis did not provide a clear diagnosis. The negative ELISA for echinococcus antibodies initially shifted the focus away from parasitic causes.
Different imaging modalities are available for diagnosis. Ultrasonography is the first-line imaging technique. More detailed information can be achieved by contrast-enhanced computed tomography (CECT) and MRI, such as size, number, location of cyst, adhesion to surrounding structures, local extension into soft tissue, determination of residual disease, and recurrences. 5 Imaging techniques are more sensitive than serological tests. In present study ultrasound and chest X-ray, did not provide a clear diagnosis. Subsequent MDCT scans revealed unexpected osteolytic lesions accompanied by a high-density soft tissue mass in the presacral space. This prompted consideration of neoplastic pelvic masses like schwannoma or chordoma. To refine the diagnosis, additional imaging with MRI was pursued. The findings, including bone erosions and a cystic lesion in the pelvis and deep gluteal space, raised suspicion of osseous hydatid disease.
Surgical removal and debridement are the most acceptable treatment for pelvic hydatid disease. Albendazole therapy is recommended both preoperatively and postoperatively to reduce the risk of recurrences. The final diagnosis is made by histopathological examination of the removed cyst. Echinococcal cysts consist of 3 layers: the outer pericyst, the middle laminated layer, and the inner germinal layer. The laminated layer appears as concentric layers of acellular material. The germinal layer contains brood capsules, protoscoleces (developing larvae), and daughter cysts. Inflammation is commonly seen in the surrounding tissues, including eosinophilic infiltrates. Depending on the host’s immune response, a chronic granulomatous reaction may be present around the cyst. Depending on the location of the cyst, secondary changes such as tissue compression, atrophy, and necrosis may be evident. In some cases, the cyst wall or surrounding tissues may undergo calcification, particularly in chronic infections. The cytological examination of the fluid shows protoscolices, hooklets in an inflammatory background. 14 Immunohistochemistry (IHC) can be a valuable tool for diagnosing hydatid cysts (echinococcosis). Some commonly used markers for hydatid cysts are
Anti-Echinococcus Antibodies: Polyclonal or monoclonal antibodies raised against various Echinococcus antigens can be used to specifically detect the presence of the parasite within the tissue. These antibodies can target different components of the parasite, such as cyst wall proteins, glycoproteins, or surface antigens.
Em2 Antigen: Em2 is a specific antigen found in the germinal layer of Echinococcus cysts. Anti-Em2 antibodies are often used in IHC to detect the presence of the parasite.
Antibodies Against Echinococcus granulosus Antigen B (EgAgB): EgAgB is a major protein antigen of Echinococcus granulosus. Antibodies against this antigen can be used to identify the parasite within cystic lesions.
Echinococcus Species-Specific Antibodies: Depending on the suspected Echinococcus species (eg, Echinococcus granulosus or Echinococcus multilocularis), species-specific antibodies can be employed to differentiate between different types of hydatid cysts.
Primary pelvic hydatid cysts are rare and their diagnosis can be challenging due to nonspecific symptoms and lack of specific serological tests. 15 Imaging plays a crucial role in the evaluation of pelvic masses, but the findings can overlap with other conditions, including tuberculosis and neoplastic diseases. 16 In this case, surgical excision and histopathological examination were essential to confirm the diagnosis of a hydatid cyst.
This case highlights the importance of considering parasitic infections, such as primary pelvic hydatid cysts, in the differential diagnosis of cystic pelvic masses, even in regions with low endemicity. Acquaintance with the atypical presentation of hydatid disease is helpful in facilitating an accurate diagnosis and reducing further complications. Appropriate imaging and histopathological investigations should be considered for accurate diagnosis and timely management. Early diagnosis and treatment are crucial to prevent complications and improve patient outcomes.
Footnotes
Acknowledgements
We would like to express our deepest appreciation to the Dean, DMMC, Nagpur for her invaluable guidance, encouragement, and expertise throughout the entire research process. Furthermore, we wish to thank the Datta Meghe Institute of Higher Education and Research (DU) for providing the necessary resources and facilities that facilitated our research endeavors. The access to the library, laboratory, and data analysis software greatly enhanced the quality of our study.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
SB: Conducted the literature search, screened the articles for inclusion and performed the data extraction and analysis. Writing and editing of the manuscript. AH: Provided expertise in the radiological applications of the topic and contributed to the interpretation of the results. NB: Provided critical feedback and revisions throughout the drafting and revision process. TS: Provided expertise in the radiological applications of the topic and contributed to the interpretation of the results. YT: Contributed in editing of the manuscript. AR: Provided expertise in the clinical applications of the topic and contributed to the interpretation of the results.
Ethics Approval Statement
The project was approved by Institutional Ethics Committee. The investigation was conducted in accordance with the Declaration of Helsinki of 1975.
Consent
Informed consent was obtained from the patient.