
Abstract
In December 2019, an outbreak of a respiratory disease called the coronavirus disease 2019 (COVID-19) caused by a new coronavirus known as severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) began in Wuhan, China. The SARS-CoV-2, an encapsulated positive-stranded RNA virus, spread worldwide with disastrous consequences for people’s health, economies, and quality of life. The disease has had far-reaching impacts on society, including economic disruption, school closures, and increased stress and anxiety. It has also highlighted disparities in healthcare access and outcomes, with marginalized communities disproportionately affected by the SARS-CoV-2. The symptoms of COVID-19 range from mild to severe. There is presently no effective cure. Nevertheless, significant progress has been made in developing COVID-19 vaccine for different therapeutic targets. For instance, scientists developed multifold vaccine candidates shortly after the COVID-19 outbreak after Pfizer and AstraZeneca discovered the initial COVID-19 vaccines. These vaccines reduce disease spread, severity, and mortality. The addition of rapid diagnostics to microscopy for COVID-19 diagnosis has proven crucial. Our review provides a thorough overview of the historical development of COVID-19 and molecular and biochemical characterization of the SARS-CoV-2. We highlight the potential contributions from insect and plant sources as anti-SARS-CoV-2 and present directions for future research.
Introduction
The severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) was first discovered in Wuhan, Hubei province, China, in December 2019.1-3 Afterward, the pneumonia-like illness spread worldwide.4-7 It was named “coronavirus disease 2019” (COVID-19) by the World Health Organization (WHO) on February 11, 2020, while the virus was named “severe acute respiratory syndrome coronavirus-2” by the International Committee on Virus Taxonomy (SARS-CoV-2). 8 So far, SARS-CoV-2 has caused a significant threat to over 7.8 billion people by negatively affecting their livelihoods and economies.
SARS-CoV-2 shares similar symptoms with the SARS coronavirus, including a dry cough, chest discomfort, fever, myalgia, dyspnea, and exhaustion.3,9,10 Less frequent clinical symptoms include nausea, headache, vomiting, abdominal pain, diarrhea, loss of taste or smell, and muscle or joint pains.4-7,11-13). In severe cases, the affected person may experience shortness of breath, hypoxia, lung damage, and dysfunction in several body organs. 14 If not treated, the disease can sometimes result in death. 15
Health professionals and family members reported cases of human-to-human transmission from close contact with an affected person.16,17 Driblets from an infected person’s coughing and sneezing are breathed in as the transmission mode. Nevertheless, the SARS-CoV-2 has been detected in stool and blood samples, as well as in aerosol and fomite.4-7,18-20 As of January 29, 2023, there were 753 million verified cases and 6.8 million deaths.21,22
It is intriguing to note that since the SARS-CoV-2 outbreak, numerous attempts have been made to snappily diagnose the contagious virus and treat it by creating medications and vaccines. A suspected or infected person’s throat or nasopharynx is swabbed, spittle, blood, intestine, and alveolar lavage fluid samples can be collected.23,24 These samples are used to perform antigen-based or nucleic acid-based laboratory discovery using either a rapid test tool or real-time RT-PCR, as appropriate. The Centers for Disease Control and Prevention (CDC) suggested a conception to stop the spread of the COVID-19 contagion that included wearing a face mask, constantly washing hands with detergents and water, using at least 60% alcohol-based sanitizers, segregating infected/suspected individualities, and observing social distance (accessed January 26, 2023).
Many advancements in treatment have been made, including the development of vaccines, monoclonal antibodies, antiviral specifics, and immunosuppressant. 25 The COVID-19 vaccination dramatically reduced mortality and morbidity in the population who received it. 26 Unfortunately, administering the COVID-19 vaccine proved fraught with difficulties. The vaccine was less readily available to meet worldwide demand and needed specialized depot facilities to conserve its potency. Also, following the completion of the initial vaccination injection, those who received the vaccine were demanded to wane their immunity every 6 months27-29 or the need for 2 dosages of some vaccines to achieve proper vulnerable protection. 30 The recent emergence of the SARS-CoV-2 omicron variant and the resurgence of vaccine populations have necessitated alternate curatives, particularly oral drug remedies.
The effective remedies now available for the care of SARS-CoV-2 are symptomatic drugs, including Remdesivir, Favipiravir, Lopinavir, Chloroquine, Ivermectin, Nirmatrelvir-Ritonavir, and Molnupiravir.23,24,31-35 The US Food and Drug Administration has approved Nirmatrelvir-Ritonavir, Remdesivir, Tocilizumab, and Baricitinib for the treatment of COVID-19 Food and Drug Administration. 36 As the disease evolves, adequate measures are being considered. However, SARS-CoV-2 seeks to mutate fleetly, making the present treatment drugs hastily lose their potency in combating the complaint. This review presents a comprehensive characterization of COVID-19 and SARS-CoV-2 by highlighting biochemical and molecular features, symptoms and modes of detection, and potential contributions from insects and plant sources in combating the disease.
Methodology
This review was based on a comprehensive selection of research work carried out on the impact of COVID-19, biochemical and molecular characterization of SARS-CoV-2, and development of anti-SARS-CoV-2 from various natural sources. Curation of data was based on an extensive literature review conducted using resources such as PubMed, PubChem, DrugBank, protein data bank (PDB) NCBI, Gene Ontology, UniProt, Prota4u, and String Database.
History and Geographical Distribution of Coronaviruses
Coronaviruses derived their name from the Latin word corona, which means the crown. 37 Morphologically, coronaviruses are particles that look like crowns with spikes projecting from their surfaces. Coronavirus was first isolated in birds in 1937 and described as infectious bronchitis virus (IBV), with the murine hepatitis virus (MHV) reported a decade later. 38 Other animal coronaviruses described afterward included the transmissible gastroenteritis virus (TGEV), bovine coronavirus (BCoV) and feline infectious peritonitis virus (FIPV), among others.39-41 In the 1960s, a coronavirus sample (labeled 229E) was taken from a student during a study of respiratory illness among University of Chicago medical students. 42 Around that period, in 1965, there were reports of B814 and HCoV-OC43 viruses isolated from patients with the common cold, which shared similar morphological features with the IBV earlier described.43,44 The “OC” viruses, such as the HCoV-OC16, HCoV-OC37, HCoV-OC38, HCoV-OC44, and HCoV-OC48, among others, are a group of viruses grown in organ cultures. This coronavirus group is suggested to originate from mice. 45 The morphological crown-like similarities observed among all the viruses described got them classified as coronaviruses, and infections with these viruses mainly occurred in winter and spring than in summer and fall. 44 Most of these coronaviruses were challenging to propagate with tissue cultures. In 2002 to 2003, there was an outbreak of another human coronavirus called severe acute respiratory syndrome (SARS), which was easily propagated with cell and tissue cultures and was thus easily diagnosed and identified. 43 Though unclear, bats and palm civets have been suggested to be the natural reservoir.44,46-48
Around the early 2000s, molecular techniques were used to amplify conserved regions in coronaviruses’ genomes, eliminating the need for cultures to propagate coronaviruses to enhance identification. In 2001, reverse transcriptase polymerase chain reaction (RT-PCR) was used to identify human coronavirus HKU1 (HCoV-HKU1) from samples taken from a 71-year-old man returning to Hong Kong from China. 43 The HCoV-HKU1 is reported to have originated from bats and murine. 49 Around the same period in 2004, a group of closely related coronaviruses, namely the New Haven human coronavirus strain (HCoV-NH) and the Netherlands human coronavirus strains HCoV-NL and HCoV-NL63, were also identified. 43 The Middle East respiratory syndrome (MERS) outbreak which was believed to have originated from bats with dromedary camels serving as intermediate hosts was first reported in 2012 in a 60-year-old man in Saudi Arabia. 46 The MERS-CoV infections were initially referred to as human coronavirus Erasmus Medical Centre (HCoV-EMC) before being adequately renamed by the international committee on the Taxonomy of Viruses (ICTV). 38
The latest or newest of the coronaviruses is the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), which was first detected in China. The SARS-CoV-2 pandemic was reported in 2019 and is believed to have originated from bats and pangolins.46,50 While the outbreaks of the earlier human coronaviruses claimed hundreds of lives globally, fatalities recorded from SARS-CoV-2 infections were in the millions worldwide. Prior to the SARS-CoV-2 (COVID-19) pandemic, the only human coronaviruses that had caused extensive infections and major outbreaks with high mortality rates were the SARS-CoV and MERS-CoV.51-53 SARS-CoV infections were first reported in November 2002 in China, spreading to more than 30 countries in less than a year (July 2023), claiming 774 lives out of 8096 infected individuals.39,54 The first MERS-CoV infection was discovered in Saudi Arabia in June 2012 from a 60-year-old patient’s lung sample. 39 Unlike SARS-CoV infections which lasted less than a year, MERS-CoV seems to persist even after the first outbreak, thus inducing occasional outbreaks in the Middle East. 38 Infections with MERS-CoV had spread to about 27 countries by 2020, with 862 fatalities out of 2506 reported cases worldwide.42,48,55 Though first reported in December 2019 in China, SARS-CoV-2 was earlier analyzed by researchers in East Malaysia who named this newly discovered virus CCOV-HuPn-2018 while working on nasal swabs from 301 pneumonia patients. 56 These researchers believed this new coronavirus had been transferred from dogs to people.
The World Health Organisation (WHO) temporarily named it the 2019 novel coronavirus (2019-nCoV). 47 It was later named COVID-19 in February 2020 48 after the WHO declared this outbreak a public health emergency of international concern due to the fast pace at which it spread globally (Figure 1). 45 There have been controversies concerning coronavirus disease 2019 (COVID-19) pandemic investigations. While some believe that the SARS-CoV-2 pandemic occurred because of spillover from bats and other animals, others believe it originated from the Wuhan Virology Laboratory. However, the latter part of these arguments is mostly driven by international politics. 57 In less than 3 months (late December 2019 to early March 2020), global cases of SARS-CoV-2 had reached 90 053. 45 Around April 2020, confirmed cases had soared to 6 057 853, with about 371 166 mortality in 167 countries worldwide. 48 By March 2020, when the virus spread had been declared a pandemic since its outbreak in November 2019, 87 SARS-CoV-2 genomes had been fully sequenced. 58 Current information curated between November 2021 and March 2023 by Global Initiative on Sharing All Influenza Data (GISAID) indicates that 4001 SARS-CoV-2 viral genomes have been collected from over 210 countries. In time, quasispecies such as Alpha, Beta, Gamma and Delta variants of SARS-CoV-2, with their attendant strains, have been duly classified. SARS-CoV-2 is the only coronavirus that killed over 300 000 people during the pandemic. Like MERS-CoV, it persists even after the outbreak. Table 1 further explains coronaviruses’ history and characteristic features.

Global map of known distribution records for COVID-19.
History and characterization of coronaviruses.

Economic Impact of COVID-19
The COVID-19 pandemic posed severe challenges to the health sector at the peak of its outbreak, which caused severe financial implications for healthcare facilities worldwide. The United Nations estimated that to provide adequate healthcare in response to the COVID-19 pandemic, low and middle-income countries would need about US$52 billion. They cost the global economy around 2 trillion dollars in 2021. 58 In America, the Hospital Associations estimated a financial impact of $202.6 billion loss in revenue or an average of $50.7 billion per month to the hospitals and healthcare systems, 60 whilst in Canada, the value of human life lost to COVID-19 was estimated in internal dollars with the Total Dollar Value of Human life Losses (TDVHL) estimated at 2 037 021 173 and an average of 231 217 per human life lost. Two provinces, Quebec and Ontario alone in Canada, accounted for 94.99% of the TDVHL. 61
As of April 2, 2020, the number of affected people was estimated to be over a million people from 181 countries, and the death toll due to the disease was reported to be 52 900. 62 The pandemic seriously impacted populations in different regions such that 15 million deaths were estimated globally for the lowest scenario. In the U.S. alone, the estimate is 236 000 deaths, which is high compared to regular influenza, with around 55 000 deaths yearly. In the year 2020, the disease and its aftermath effects in Germany were expressed as the number of years of life lost to the disease or death such that 305,641 years of life were believed to have been lost to the disease, with 34.8% of men and 21% women being the percentage of disability-adjusted life years (DALY) that persons under the age of 70 lost. 63
Concerning agriculture and the food supply chain, sufficient evidence confirms that COVID-19 affected food demand, which affected food security due to reduced purchasing power and mobility restrictions. During this period, the restriction of farmers from working on their farmlands, buying seeds from the markets, or even selling their farm products due to lockdowns resulted in increased hunger and malnutrition amongst the most vulnerable populations. 64 Also, the use of migrant labor for harvesting disrupted the supply chains. Again, since restaurants and hotels closed down, sales of crops and vegetables were affected. Another major challenge was the misinformation of the populace on social media that chickens carried COVID-19, thereby significantly affecting the poultry industry. 65
Many nations have suffered severe economic losses due to covid-19. Oil prices for the first time hit subzero territory, with China suffering a loss of 13.5% in industrial production, 92% in car sales, 21% in retail sales, and 95% in restaurant business. 66 Also, the decline in working hours as of April 1, 2020, resulted in full-time job loss estimated to be equivalent to 200 million. 66 In India, the pandemic hugely disrupted economic activities, resulting in a 34.6% and 28.7% reduction in exports and imports, respectively, as most countries closed their borders. This resulted in the World Bank and other credit rating agencies downgrading the growth for 2021, the lowest experienced in 3 decades. 65 There was also an overall Gross Domestic Product (GDP) loss in the global economy (Table 2), so the cost of lost economic output potentially ran into trillions of dollars. 67
GDP losses in selected countries.
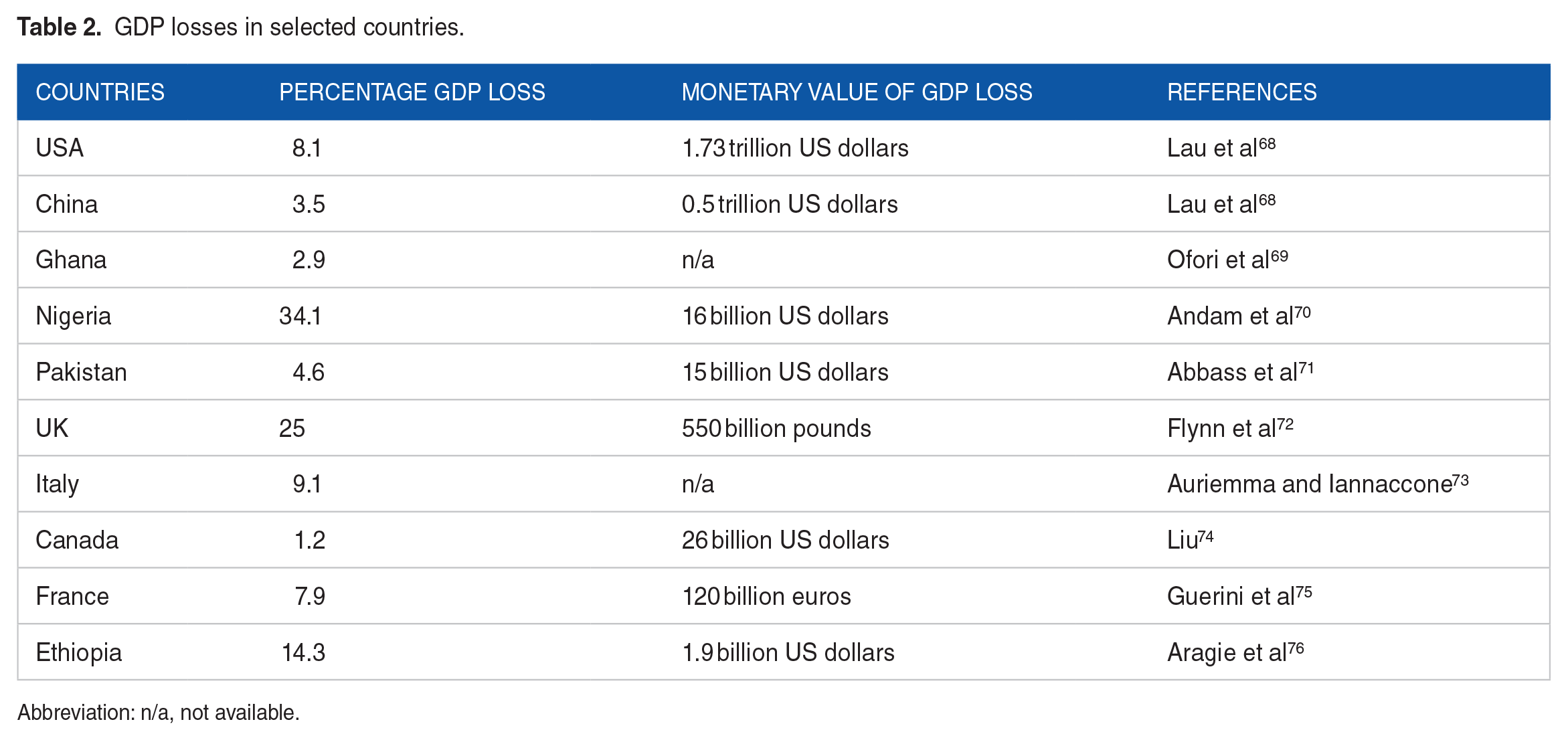
Abbreviation: n/a, not available.
Its impact on the tourism industry resulted in a brief, significant loss to the worldwide economy, assessed to be about 2.7 trillion U.S. dollars by experts. This resulted from the ban on travel imposed by some countries, with airlines and tourism industries making losses in millions of dollars. 77 During the COVID-19 pandemic, there was a general decline in global airport revenue around the second quarter of 2020 to about $39.2 billion and around $97 billion for the entire year due to many countries’ imposition of travel restrictions. Data obtained from the World Travel & Tourism Council showed that before the pandemic in 2019, the travel and tourism sectors contributed about 14.3% and 13% to the Spanish and Italian GDP 13%, respectively. However, these figures declined considerably during the pandemic. The decline resulted from low patronage from hotels, travel agents, airlines, restaurants, and other sectors, which benefit directly from tourist expenditures. For the United States, the travel and tourism sector contribute 8.6% to the country’s GDP. However, the U.S. Travel Association and Oxford Economics reported that an estimated 8 million people in the tourism industry lost their jobs during the pandemic. Expenditures on travel and tourism were estimated to have reduced by $500 billion in 2020, whereas the international tourism sector was estimated to have shrunk by 45% to 70%. The hotel and restaurant businesses were no exception, as about 51 million businesses faced economic difficulty and increased unemployment. 78
Although there have been many losses due to COVID-19, there have also been some winning instances, especially in the environment. The environment benefited from the lockdown, which resulted in unexpectedly deficient pollution levels globally, especially in Asia countries like China and India and developing countries. The lockdown effect from COVID-19 on the environment was positive as economic, institutional and industrial activities came to a standstill. Reduced carbon emission, clear skies and cleaner breathing air were observed, with a 71% reduction in nitrogen dioxide levels reported by the Central Pollution Control Board of India’s Environment Ministry. 65 The business also boomed for supermarkets and grocery stores as online sales for essential items and food were in high demand. 66
The economic importance of the COVID-19 disease is immense in that every country worldwide has its share of the associated problems. Most countries are battling the disease’s aftermath, from losing many precious lives, money, livelihood and jobs. The only positive impact of COVID-19 was the clean environment observed due to the lockdown imposed by most countries for weeks and, in some cases, months, although this could not outweigh the negatives.
Symptoms and Detection of COVID-19
Generally, the COVID-19 disease is manifested by signs and symptoms ranging from mild (asymptomatic) to severe forms (symptomatic) and death. This implies that some individuals may not present any signs and symptoms of the disease but can still spread it, and others may show worsened signs and symptoms. Typical symptoms of COVID-19 may include fever, dry cough, sore throat, fatigue, loss of smell and taste, diarrhea, chest pain, conjunctivitis, hyposmia, hypogeusia, rhinorrhea, tachypnea, dyspnea, exhaustion, confusion.79-81 For most of these symptoms, fever and cough are most predominant in patients with COVID-19.79,81,82 In contrast, a study in Ghana found fever not to be the most predisposing symptom in individuals with COVID-19 but instead cough and headache. 83 It thus suggests that although temperature may be a valuable contributing factor, there may be better tools to screen individuals with the disease. Again, most of these symptoms may be associated with other viral, bacterial and protozoan infections; hence, further tests are needed to confirm the disease. It is expected that within a week of infection, adaptive immunity should rise, but this may not be possible in some individuals with certain risk factors such as age and comorbidities.13,84,85 This may inform the significant complications of the disease seen in some patients. These complications include pneumonia, acute respiratory disease (ARD), septic shock, multiorgan dysfunction, hemodynamic instability and cardiovascular complications.86-88 These complications have been shown to account for about 20% of all severe COVID-19 cases. 86
Due to some severe complications associated with the disease, lack of vaccines and ultimately death, there was a need to develop robust techniques to quickly and early detect the disease. 89 The early detection was to provide measures for the timely recovery of the patients and the spread of the disease. The development of techniques is based on certain structural features of the causative agent and its genetic compositions. Alongside the clinical manifestations of the disease, molecular-based assays, serology (antigen-antibody interactions), imaging, and biosensors have been used to detect the virus. 89
Molecular-based assays are the most widely used technique in COVID-19 detection due to their high sensitivity in the early detection of viremia during the early stages of the disease. 90 One of the molecular-based assays used extensively as the gold standard in detecting COVID-19 is the reverse transcriptase quantitative polymerase chain reaction (RT-qPCR). The RT-qPCR is a very sensitive technique for quantifying mRNA. It allows for detecting rare transcripts and minor variants in gene expression. The principle of this technique relies on targeting specific genes and regions of the SARS-COV-2 genome. Notably amongst genes and regions include the RNA-dependent RNA polymerase (RdRp) gene, nucleocapsid (N) gene, envelope (E) gene, spike (S), and the open region frames 1b (ORF 1b) and 8 (ORF 8).16,90,91 Some challenges with this technique are that it is laborious, time-consuming and requires skilled personnel in sample handling and processing. Another drawback is the high inconsistency or the high number of false negative results observed in some individuals with the disease.92,93 The differences are sometimes attributed to variations in viral RNA sequences that may affect primers designed from the ORFs and N genes. Again, the viral load has been shown to be different at specific sites in patients; hence sampling procedures may be a significant contributing factor in the higher rate of false negatives.4-7
Another PCR method similar to the RT-qPCR is digital droplet PCR (ddPCR). This method is precise and sensitive for samples with low viral loads, hence minimizing situations of false negatives. 94 In this test, the reaction is first partitioned into several individual reaction vessels before amplification. It cycles the samples to an endpoint, and then the positive samples are detected by counting the number of positive droplets. 89 This reduces the contaminant level while maintaining the integrity of cDNA in the sample. 95 The method’s robustness was confirmed by a study conducted by Vasudevan et al 96 in which the viral load SARS-Cov-2 was quantified in crude lysate without RNA extraction.
The loop-mediated isothermal amplification (LAMP) method has also been used to detect SARS-Cov-2 in samples. Generally, LAMP is a novel molecular tool that amplifies a few copies of DNA in a shorter time (less than an hour) under isothermal conditions with higher specificity and sensitivity. Since SARS-CoV-2 is an RNA virus, the RNA is reverse transcribed, hence the name RT-LAMP. This method amplifies a specific target region under isothermal conditions. 90 The reaction mixture involves 4 to 6 different primers, which would recognize 4 to 6 regions on the target gene and a Bst DNA polymerase, which causes an elongation of the nucleotide sequence chain. Primers have been designed targeting the Nsp3 region, 97 ORFiab gene, 98 and N, M, and S genes. 99 This amplification method does not require an expensive machine (thermocycler). However, it can be conducted using a water bath or heating blocks, and the amplification product is visualized using a fluorescent dye. 90 The method has been used as a point-of-care diagnosis of COVID-19 to overcome some of the shortcomings of the RT-qPCR method. One of this method’s drawbacks could be a lack of sensitivity due to cross-reactivity and possible mutations at the primer binding site of the virus. 90
An antibody in a sick person may indicate the development of an immune response to a pathogen. This knowledge has been used to detect the presence of specific pathogenic agents in bodily fluids. This forms the basis of most serological tests, such as rapid diagnostic tests, enzyme-linked immunosorbent assays (ELISA), chemiluminescent immunoassays and neutralization assays. These tests have been used as an alternative to augment nucleic acid tests. 100 The tests usually detect anti-SARS-CoV-2 immunoglobulins such as IgG and IgM against some surface antigens in the serum or plasma of individuals infected with COVID-19. Serological tests have emerged as valuable tools to identify individuals previously infected with SARS-CoV-2. 100 Compared to nucleic acid tests, serological tests are easy to perform and require less technical expertise and instrumentation. 101 However, they are limited in their performance as rapid tests since antibodies appear later during the disease. 101
The use of enzyme linked immunosorbent assay (ELISA) and multiplex immunoassays have been used to detect the presence of SARS-CoV-2 in serum and saliva samples.102-105 These assays have been used to measure individual or multiple analytes in biological samples simultaneously. In their study, using a commercial serum-based ELISA kit, MacMullan et al 102 achieved 100% specificity and 84.2% sensitivity in saliva samples. They postulated that it is possible to test IgG against SARS-CoV-2 in saliva, thus providing an accessible and non-invasive option for detecting prior infection. In another ELISA study, Luo et al 105 demonstrated that the N-protein is more sensitive and specific in detecting SARS-CoV-2 specific IgG antibodies in human serum than the S-protein.
Chemiluminescence involves the emission of electromagnetic radiation caused by a chemical reaction to produce light. This principle has been employed in a chemiluminescence assay to detect small amounts of biological samples. The assay is a reproducible, fast, cost-effective, precise method of measuring IgG and IgM antibody levels. It combines chemiluminescence and some immunochemical reactions to detect antibodies in the sera of COVID-19 patients.106,107 In their study, Yin et al108,107 designed 4 detection assays, ACE2-RBD, S1-IgG, RBD-IgG, and N-IgG, based on the chemiluminescence technique to identify probable antibodies in sera. Results from the study showed that the specificity and sensitivity of the 4 methods were very high. Thus, these methods would be instrumental in the large-scale detection of the disease and in evaluating the effect of SARS-CoV-2 vaccination. A study also demonstrated that detecting IgM by chemiluminescent immunoassays is not encouraging. It was therefore recommended that the measurement of total antibodies rather than IgG and IgM alone would be better for monitoring the progress of the infection and diagnosis.13,108
It is worth noting that diagnostic tests using nucleic acids or antigen detection assays are available as rapid diagnostic tests (RDTs). This is to ensure early detection of the disease and also screen large populations who are suspected of having the disease. They are approved for use in symptomatic and asymptomatic individuals. 109 The rapid antigen detection assays are in contrast to the antibody detection assays in that they can detect the virus in respiratory samples. 110 Freire et al 111 stated that many commercially available RDTs can detect SARS-CoV-2-specific antigens. Using an antigen-based immunofluorescence RDT on respiratory samples from infected individuals, Porte et al 112 showed that the assay had very high sensitivity and specificity. Based on the results, they concluded that the method could be used in the early detection of SARS-CoV-2 in situations where access to molecular methods is limited.
Overall, sequencing techniques have emerged as a powerful tool for tracking the spread of COVID-19 and identifying new variants. These techniques provide essential information about the genetic diversity of the virus, as well as the transmission dynamics and potential clinical implications of new variants. As such, sequencing is likely to continue to play an essential role in the global response to the COVID-19 pandemic. One study by Faria et al 112 used sequencing techniques to investigate the emergence and spread of the B.1.1.7 variant of SARS-CoV-2 in the United Kingdom. The study found that the B.1.1.7 variant had multiple mutations in the spike protein, which may have contributed to increased transmissibility. Another study by Voloch et al 113 used sequencing techniques to investigate the genetic diversity of SARS-CoV-2 in Brazil. The study found that Brazil’s virus had multiple introductions, and different regions had distinct viral lineages. The study also found that there were mutations in the spike protein that were unique to Brazil, highlighting the importance of sequencing for understanding the local transmission dynamics of the virus. Also, in Ghana, a study detected the presence of the B.1.1 lineage followed by the alpha variant, B.1.1.138 lineage and delta variant. 114 The rapid evolution of the virus suggests a potential for the emergence of novel variants.
Imaging techniques have played a crucial role in detecting and managing COVID-19. These techniques include chest X-ray, computed tomography (CT), and ultrasound. Chest X-rays and CT are frequently used for diagnosing and monitoring COVID-19 patients. A study by Ai et al 115 found that chest CT scans could detect COVID-19 in 97% of patients, which was higher than the sensitivity of RT-PCR (71%). The researchers concluded that chest CT could be a complementary diagnostic tool for COVID-19. It is essential to note that imaging findings on chest X-rays and CT are not specific to COVID-19 and can be similar to other respiratory diseases. Ultrasound is a portable and cost-effective imaging technique with the advantage of minimizing radiation exposure. 116 It has yet to be widely used in the detection of COVID-19. However, studies have shown that sure signs such as thickened pleural lines, subpleural consolidations, and B-lines can be indicative of pulmonary involvement in COVID-19 patients.116,117
Mode of Transmission and Infection of SARS-CoV-2
There are several modes of transmission of the disease, which could be either direct or indirect. The direct means could be due to droplets or human-to-human transmission, while the indirect means may involve contact with infected objects or airborne contamination. A common source of the spread of the airborne disease may be personal protection equipment (PPE). The most acceptable transmission mode of virus is that it spreads from person to person through coughing, sneezing, singing, and releasing respiratory droplets or aerosols. 118 Also, worldwide reports suggest that in virtually every nation, the disease transmission is brought about by inhaling aerosols into the upper respiratory system and lungs.119,120 Typically, the droplets can travel a distance of about 2 m and float in the air for some hours. It can stay in the air for up to about 3 hours while still being intact and pathogenic in droplets <5 microns in size. 18 However, airborne isolation, proper room ventilation, and disinfection could prevent the virus from spreading by aerosols. 121 Concerning indirect transmission, when an individual’s hands come into direct contact with mucous membranes such as the eyes, nose, or mouth after touching a surface infected with the virus, the symptoms of COVID-19 may manifest. It is thus advisable to thoroughly wash hands with soap under running water or hand sanitizer as shown in Figure 1. 122 According to a WHO-China joint report, the fecal-oral transmission route did not seem to be a significant factor in the spread of the disease. However, viral RNA has been found in blood and stool samples, culturing living SARS-CoV-2 from some individuals with COVID-19. 123 A joint WHO-China report showed that out of tens of thousands of confirmed cases in China, the rate of secondary COVID-19 infection varies from 1% to 5%. 118 However, COVID-19 patient produces viral plumes of thousands of droplets per cubic centimeter through frequent sneezing and dry coughing. It is critical to evaluate the particle properties and propensity of SARS-CoV-2 aerosols or droplets to circumvent various physiological barriers and enter the host body because it is thought that SARS-CoV-2 infection is transmitted mainly via aerosols and droplets. 124 Initially, it was believed that bigger droplets from the patient conveyed the pathogens, which settled on surfaces and were then transferred to the host by the dust that rose from the dried droplets. 125 Recent research has shown that COVID-19 patients who sneeze and cough produce droplets with sizes ranging from 0.6 to 100 μm, and the quantity of droplets rises proportionately to the coughing rate. Most of these droplets are smaller than 10 μm, and more than 97% are typically lower than 50 μm. Asymptomatic patients can also produce and release significant numbers of droplets smaller than 1 μm through regular breathing and speech.
Furthermore, transmission from symptomatic individuals can more easily be identified, and they can take precautions to stop the virus from spreading; however, it is much harder to stop transmission from non-symptomatic individuals. The scope and timing of non-symptomatic transmission significantly impact the efficacy and implementation of public health measures. According to indirect evidence, asymptomatic people are less contagious than symptomatic people, and less than half of SARS-COV-2 infections in China and European nations in the first half of 2020 were caused by asymptomatic people. 126
In a study on 4 hospital employees who contracted the COVID-19 infection, the results showed that although each patient had at least 2 negative tests, the RT-PCR test was persistently positive from 5 to 13 days after discharge. In addition, viral shedding in the stool probably lasts up to 5 weeks, with a mean of 11.2 days after the negative respiratory tract test.127,128 So, because SARS-CoV-2 can spread from recovered patients, the discharge protocol had to be altered. These included complete remission of the patient’s acute exudative pulmonary disease; 2 consecutive RT-PCR negative results in at least a 24-hour window of tumors on the chest computed tomography scan, return of temperature to normal after >72 hours, and improvement in the patient’s respiratory symptoms.129,130 Moreover, looking into COVID-19’s potential vertical transmission is crucial because pregnant women are particularly vulnerable to getting the virus. Some studies revealed immunoglobulin M (IgM) antibodies to SARS-CoV-2 were present in newborn infant blood, so possible transmission of SARS-CoV-2 from mother to fetus could not be excluded. A study by Antonelli et al 131 found that a baby delivered from an affected mother tested negative for 7 duplicate samples of neonatal blood, stool, and oropharynx.
Another study analyzed the average rate of rise of new COVID-19 patients compared to the average temperature daily in countries such as Iran, Italy, Germany, Spain, and the United States. 132 Different regions in each nation were analyzed individually to reduce the impact of confounding factors like the implementation of government actions or cultural variations between these countries. According to findings from the study, there was a strong correlation between the mean daily air temperature difference between the 2 regions and the average cumulative daily rate of new patients in those 2 regions. 133 Also, it was found that the average temperature and humidity of affected cities were between 5°C to 11°C and 47 to 79%, respectively. For SARS-CoV-2 to survive in vitro, the ideal temperature and humidity ranges were 4°C and 20% to 80%, respectively. However, the contaminated cities never had an average temperature below 0°C. Furthermore, the virus spread in the latitude range of 30° to 50° north of South Korea, Japan, Iran, and North Italy. Comparing the maps of COVID-19 spread to the world climate, there is no correlation between temperature and the distribution of the virus, despite what the findings showed. 134
According to a recent study, SARS-CoV-2 aerosols are contagious and can infect humans for at least 3 hours with a half-life of roughly 1 hour. 134 Many mathematical models, primarily the Wells and Riley models, were utilized to evaluate the risk of infection when close to a COVID-19 patient. 134 The bat Rhinolophus affinis was identified as the 2019-nCoV’s natural host since its genome shares 96.2% of its total length with that of BatCoV-RaTG13. Research suggests that a third host, such as a palm civet, is necessary for transmitting SARS-CoV-2 from an animal to a human. 135 Due to the 2019-nCoV and SARS-CoV-2 similarities, many experts think that an intermediate host animal is likely required to transmit 2019-nCoV to people. Finding the intermediate 2019-nCoV host is essential if this is the case to stop interspecies transmission. Pangolins have been proposed as a potential intermediate host for 2019-nCoV in this regard; however, this hypothesis has yet to be proven. 136 Figure 2 throws more light on the mode of infection of SARS-CoV-2.

Mode of infection of SARS-CoV-2.
Biochemical and Molecular Characterization of SARS-CoV-2
There are close links between the SARS-CoV-2 pandemic and epidemics involving SARS-CoV (Severe Acute Respiratory Syndrome Coronavirus) and MERS-CoV (Middle East Respiratory Syndrome Coronavirus) which occurred in China (2002) and Saudi Arabia (2012) respectively. 137 The family of coronaviruses, Coronaviridae, are single-stranded, enveloped positive-sense RNA (ribonucleic acid) viruses of the order Nidovirales. 138 Of the 4 genera within Coronaviridae; Alphacoronavirus, Betacoronavirus, Gammacoronavirus, and Deltacoronavirus, only 2 directly affect human health.
Alphacoronaviruses contain the strains 229E and NL63 associated with the common cold, while Betacoronaviruses are associated with more severe respiratory tract disease 138 The Betacoronavirus genus is further divided into 4 groups; Group A associated with human respiratory tract infections contains coronavirus OC43; Group B associated with severe pneumonia contains SARS-CoV; Group C contains the human beta-coronavirus 2c EMC/2012 (HCoV-EMC) and HKU9, the Rousettus bat coronavirus belongs to Group D. 138
SARS-CoV-2 is the most rapidly evolving within the betacoronavirus genus due to its RNA-dependent RNA polymerase, which exerts very little proofreading activity during replication. 139 The infidelity of the RNA polymerase consequently produces a heterogenous viral pool containing genetic variants classified as quasispecies. 139 Quasispecies refers to viral population structures that contain numerous genome variants due to relatively high mutation rates as viral replication proceeds. 140 SARS-CoV-2, thus named because of its similarity to SARS-CoV, is composed of an envelope protein (E), spike glycoprotein (S), membrane protein (M), and a linear positive-sense, single-stranded, ~30 kb (kilo bases) RNA nucleocapsid protein (N). 141
While SARS-CoV-2 strains share similarities with counterpart Betacoronavirus such as MERS-CoV (50%) and SARS-CoV (79%), it is more genomically similar (88%) to bat-SARS-like-CoV. 142 Phylogenic classification of the strains presents 2 clades in the tree with MERS-CoV in one clade and SARS-CoV-2, SARS-CoV, bat-SARS-like-CoV, and bat-SARS-CoV in the other clade. 142 Additionally, whole genome sequence analysis indicates that SARS-CoV and bat-SARS-CoV are descended from bat-SARS-like-CoV while SARS-CoV-2 is parallel to bat-SARS-like-CoV. This explains the genomic similarity (88%) between the 2 and why the SARS-CoV-2 genome is organized similarly to bat-SARS-like-CoV ZXC21 and ZC45 genomes. 142
Characteristic of all coronaviruses, the approximately 14 open reading frames (ORF) contained in the genetic material codes for 31 non-structural, structural, and regulatory proteins altogether. 143 A set of16 non-structural enzymatic proteins (NSP1-16) make up a helicase, an endonuclease and the RNA-dependent RNA polymerase; one of the 4 structural proteins, spike (S) protein mediates host cell binding, while the remaining 11 (ORF3a, ORF3b, ORF3c, ORF3d, ORF6, ORF7a, ORF7b, ORF8, ORF9b, ORF9c, ORF10) are accessory proteins. 143 Although there are similarities between the proteins encoded by SARS-CoV-2, bat-SARS-like-CoV ZXC21, and bat-SARS-like-CoV ZC45, minor differences exist. For instance, SARS-CoV-2 encodes a longer spike protein than the 2 bat variants and those coded by SARS-CoV and MERS-CoV. 142 Genomes sequence analysis conducted by Zhang et al 142 mapped the 12 amino acid coding regions; 1ab, S, 3, E, M, 7, 9, 10b, N, 13, and 14, which contribute to the similarities between SARS-CoV-2 and bat-SARS-like-CoV. The differences between SARS-CoV-2, SARS-CoV, and MERS-CoV were also traced to their amino acid coding regions (Table 3).
Differences between amino acid coding regions in SARS-CoV-2, SARS-CoV, and MERS-CoV.

Another difference between the 3 globally acclaimed viruses is that MERS-CoV relies on recognizing dipeptidyl peptidase 4 (DPP4) receptors to infect human cells. At the same time, SARS-CoV-2 and SARS-CoV bind angiotensin-converting enzyme 2 (ACE2) receptors for host cell invasion. 141 Total mutations and subtle variations also exist in the S gene of SARS-CoV-2 lineages Alpha, Beta, Gamma, and Delta (https://gisaid.org/lineage-comparison/). 144
As the pandemic peaked and it became evident how quickly SARS-CoV-2 evolved to evade medical intervention, research focused on detecting new variants and lineages. The extent of mutation within SARS-CoV-2 variants isolated in the USA, Italy, Germany and China was investigated using a neighbor-joining method linked to the MEGA X (Molecular Evolutionary Genetics Analysis X) software. 142 By aligning complete genome sequences of representative coronaviruses, the team carried out phylogenetic analyses based on the nucleotide sequences generated from the neighbor-joining. Results from the pairwise sequence identities indicated a highly shared identity (99.5%-100%) among SARS-CoV-2 isolates from the 4 countries. 142
When the SARS-CoV-2 UK variant B.1.1.7 became a variant of concern (VOC), a research team in Jordan analyzed genetic variations in locally prevailing SARS-CoV-2 and the UK VOC. 139 Of the 579 sequences of SARS-CoV-2 analyzed, 19 different SARS-CoV-2 genetic lineages were identified, with 3 being significantly vital. Major amino acid substitutions occurred in the spike glycoprotein of the 3 variants (B.1.1.312, B.1.36.10, and B.1.1.7) identified in Jordan, 139 highlighting the rapid rate of often dangerous mutation within the virus. The team reported a deleterious amino acid substitution (Q957L) in the S gene region of variant B.1.1.312, resulting from a non-synonymous substitution. The molecular signature of the second Jordanian variant (B.1.36.10) indicated a synonymous mutation that yielded the wild-type protein (D614G), making the variant neutral 139 about virulence. Similarly, a team in Italy investigating the variations between the Wuhan-Hu-1variant and a clinical sample reported 2 non-synonymous changes in ORF1a and ORF3a in the region responsible for spike protein-coding. 58 The substitution identified in the Italian isolate (G26144T) was similarly present in 5 sequences from cases occurring in Australia, the USA, Taiwan, and France.
Despite worldwide vaccination, SARS-CoV-2 VOC Omicron, first identified in November 2021 and first detected in Botswana/Hong Kong/South Africa, rapidly became predominant, spreading to as many as 40 countries. 145 The Delta, first identified in the USA and occurring in 99% of SARS-CoV-2 genomes sequenced there, was rapidly overshadowed by the ~20 kb Omicron. 145 Work in 2021 reported that Omicron contained 14 shared mutations with existing variants and 22 novel mutations (including 3 deletions) in the S gene alone, while 10 additional mutations occurred in ORF1a. 145 Of the 10 ORF1a mutations, 4 were deletions (G3676del, L3674del, S2083del, and S3675del) while 4 of the remaining 6 mutations (A2710T, I3758V, K856R, L2084I, P3395H, and T3255I) occurred in NSP6. 145 The same study also reported other important mutations that occurred within the E (T9I), M (D3G, Q19E, and A63T) and N (P13L, E31del, R32del, S33del, R203K, and G204R) structural genes and NSP9b regions ((P10S, E27del, N28del, and A29del). Concerning host binding and invasion, Omicron was shown to contain 8 new mutations, notably Q493R, which overlaps with 7 previously identified anti-RBD (receptor binding domain) monoclonal antibody (mAb) biding sites 145 Current data from GISAID used in this review to visualize the various mutations in the S genes of Delta and omicron variants indicate more than 22 mutations (https://gisaid.org/lineage-comparison/). The GISAID database additionally informs about a 3 amino acid (EPE) insertion at position 214 in the spike protein.
Current Drugs and Vaccine Status
Several antiviral medications, many of which are used to treat the symptoms of the human immunodeficiency virus (HIV), hepatitis, and the flu, are currently administered off-label or are undergoing clinical testing to treat COVID-19. Remdesivir is an antiviral drug developed from the collaboration between Gilead Sciences, CDC, and the US Army Medical Research Institute of Infectious Diseases to develop treatments for RNA viruses. 146 Despite its previous failure in treating Ebola in 2014, it was employed and administered during the initial phases of the SARS-CoV-2 pandemic. 147 It gained popularity due to early trial findings that suggested it helped speed up recovery for seriously ill hospitalized patients. This phosphoramidate prodrug is metabolized into an active form called GS-441524, which functions as a nucleoside analog that inhibits the RNA-dependent RNA polymerase enzyme (RDRp) needed for replication, thereby reducing the viral load in the body. 148
Usually, it is given intravenously over a 5- to 10-day period. However, there have been several concerns regarding its side effects, including nausea and vomiting, with reports suggesting that it can lead to acute renal injury and respiratory failure.31,149
Tocilizumab, a recombinant humanized anti-IL-6 receptor monoclonal antibody that targets the interleukin-6 receptor, which is involved in inflammatory response by competing with both the soluble and membrane-bound forms of the human IL-6 receptor (IL-6R), was initially approved for use in patients with rheumatologic disorders. 150 This drug has been investigated as a potential target for treating various conditions, including the cytokine release syndrome associated with certain types of cancer and SARS-CoV-2. 151 Tocilizumab is utilized in hospitalized pediatric patients who need supplemental oxygen, invasive or noninvasive mechanical ventilation, or extracorporeal membrane oxygenation (ECMO) and receive systemic corticosteroids. Several clinical trials have been done to investigate the effectiveness of this drug, but the results have been conflicting.152-154 A meta-analysis of clinical trials published in the Lancet suggested a lower risk of death and requirement for mechanical ventilation in hospitalized COVID-19 patients. 155 However, some studies have not indicated a meaningful benefit with the optimal time and dosage of tocilizumab for COVID-19 individuals still being debated.
The SARS-CoV-2 major protease (Mpro) is the target of the novel antiviral drug nirmatrelvir. In contrast, ritonavir, a protease inhibitor of HIV and cytochrome P450 (CYP) 3A, has been investigated for its potential to increase nirmatrelvir concentrations to the target therapeutic range. 156 A combination of both drugs has been employed in treating individuals with a higher risk of death or hospitalization but do not require supplemental oxygen. 157 Nirmatrelvir-ritonavir is packaged as oral tablets of 150 and 100 mg, respectively and is prescribed at an authorized dose of 300 mg/100 mg (2 tablets of nirmatrelvir and 1 tablet of ritonavir) to be taken orally every 12 hours. It can be administered with or without food for 5 days. 158 However, some individuals have concerns about the COVID-19 rebound. 159 Figure 3 depicts the chemical structures of common drugs that may be used to control SARS-CoV-2.

Chemical structures of remdesivir, nirmatrelvir, and ritonavir.
There are about 242 vaccine candidates as of May 2023, with 50 approved worldwide and 92 at different phases of clinical trials.21,22,160 Their mechanism of action differs based on the unique response to either DNA, RNA or protein.1604 There are 2 categories of COVID vaccines, namely component viral vaccine and whole virus vaccine. An example of a component viral vaccine is the protein subunit vaccine, which involves purifying specific components of the spike protein found on the surface of SARS-CoV-2. 161 Novavax and Covovax are typical examples of protein subunit vaccines. 162
Another type is the Virus-like Particle (VLP) vaccine. These vaccines work by attenuating the SARS-CoV-2 virus. VLP vaccines contain viral proteins that mimic the structure of the virus but do not contain any genetic material. By presenting these viral proteins to the immune system, VLP vaccines stimulate an immune response without causing an infection. 163
Nucleic acid vaccine, especially mRNA vaccines, has gained significant attention and has successfully developed SARS-CoV-2 vaccine. The most successful vaccines produced by Pfizer-BioNtech (Comirnaty) and Moderna (mRNA-1273) are mRNA vaccines. 164 Both products contain mRNAs encoding the spike protein of SARS CoV-2, which is needed in the attachment of the virus to the host cells expressing its receptor angiotensin-converting enzyme 2. 165 These mRNA vaccines use liposomes to deliver SARS-CoV antigens. The suitable liposome enhances the uptake and internalization, leading to higher therapeutic delivery. The liposomes also minimize mRNA degradation before internalization. 166 Pfizer-Biotech and Moderna vaccines are administered as a 2-dose regimen, with a recommended interval of 21 days between doses and 28 days, respectively, for either vaccine. 167 They have demonstrated high efficacy in clinical trials and real-world effectiveness in preventing severe disease and hospitalization from COVID-19. 168
Many viruses have been successfully employed as vectors, including adenovirus, vesicular stomatitis virus, vaccinia virus, adenovirus-related virus, retrovirus, lentivirus, cytomegalovirus, and Sendai virus. Viral vector-based vaccines introduce SARS-CoV-2 genes into hosts, thereby increasing immunogenicity without adjuvants and leading to a strong cytotoxic T-cell response to kill virus-infected cells. 169 Some vaccines enter cells and produce SARS-CoV-2 protein, but essential genes are inactive, preventing replication. 170 In-depth research has demonstrated the high efficacy of vector-based vaccinations in reducing COVID-19 illness. They provide benefits such as single-dose administration, convenience with storage, and transport. Current studies and surveillance continue to assess these vaccines’ safety and effectiveness against new SARS-CoV-2 variants and the length of their protective effect.
Plant Sources of anti-SARS-CoV-2
Fruits and vegetables are regarded to be of critical importance for the management of COVID-19. Individuals with underlying medical conditions are at the highest risk of becoming severely ill. 171 Fruits and vegetables such as red beets, squash, apples, pears, berries, mangoes, oranges, grapes, soybeans, mushrooms, cantaloupe, bananas, beans, spinach, onions, broccoli and parsley contain essential nutrients and minerals that may benefit COVID-19 patients with underlying medical disorders such as cardiovascular diseases, diabetes, chronic kidney disease, obesity and compromised immune systems. 171 Also, higher consumption of fruits, vegetables and dietary fiber may lower the odds of contracting COVID-19. 172 Nutrients and minerals that may feature prominently include calcium, carotenoids, copper, fiber, folate, magnesium, manganese, potassium, iron, and vitamins A, B1, B6, C, and D. 171
There are also relatively inconclusive investigations about the potential of herbs and spices to help fight COVID-19. Ginger has been traditionally used as a natural remedy for respiratory infections, and studies have suggested that it may have antiviral activity against respiratory viruses, including SARS-CoV-2. 173 Cinnamon has been shown to have antiviral properties against respiratory viruses, including SARS-CoV-2. 174 Traditional Chinese herbal medicines such as Ephedra sinica, Glycyrrhiza uralensis, and Lonicera japonica have been studied for their potential to treat COVID-19. 175 Herbs and spices that were commonly employed to help in the prevention of COVID-19 disease in the Ghanaian society included Moringa oleifera, Allium cepa, Camellia sinensis, Xylopia aethiopica, Taraxacum officinale, Zingiber officinale, Hibiscus sabdariffa, Tetrapleura tetraptera, Syzygium aromaticum, Menta piperita, Parkia biglobosa, Capsicum annuum, and Ocimum gratissimum. 176
In particular, several phytochemicals of plant origin have been investigated for their use against COVID-19 in the context of mechanisms of action against SARS-COV-2 (Figure 3). Quercetin, a flavonoid found in many fruits, vegetables, and herbs, has been found to inhibit the entry and replication of SARS-CoV-2 in vitro and has been proposed as a potential COVID-19 metabolism modulator. 32 Combined with vitamins C and D, quercetin may exhibit synergistic effects against viral loads and exert immunomodulatory effects. 32 Quercetin may inhibit SARS-CoV-2 replication by possibly suppressing the activity of the leading viral protease, as well as reducing the production of pro-inflammatory cytokines that are associated with severe COVID-19 symptoms 177
Curcumin, a polyphenol found in the spice turmeric, depicts promising antiviral properties. Curcumin may inhibit SARS-CoV-2 replication and inflammatory responses in alveolar cells, thereby acting as a potential agent against pulmonary impairment. 178 This suggests that it may have therapeutic potential for the treatment of COVID-19. Curcumin may also exhibit a cardioprotective effect, which may help prevent myocardial injury in COVID-19 patients.9,178
It may function as a potent antithrombotic to help prevent coagulation and thrombosis in COVID-19 patients. 178 Furthermore, curcumin may act to reduce inflammation in SARS-CoV-2 infection. The gene expression and secretion of several pro-inflammatory cytokines were shown to be modulated upon treatment with nanocurcumin.179,180
Epigallocatechin gallate (EGCG), a catechin found in green tea, has been investigated for its potential use against COVID-19. As already indicated for curcumin, EGCG is also known to possess antiviral properties. EGCG may inhibit the entry and replication of SARS-CoV-2 in vitro. 181 The compound inhibited SARS-CoV-2 infection in vitro, suggesting it may have therapeutic potential for treating COVID-19. 181 In addition to SARS-COV-2, it blocked the entry of MERS- and SARS-CoV-2 pseudotyped lentiviral vectors. 181 Mechanistically, the catechin was found to inhibit the SARS-CoV-2 spike-receptor interaction in vitro, 181 suggesting that it may act by inhibiting the binding of the spike to angiotensin-converting enzyme 2 (ACE2). 51
Andrographolide, a natural compound found in the plant Andrographis paniculata, may exhibit considerable inhibition of SARS-CoV-2 virus infection and inflammation in lung epithelial cells by modulating angiotensin-converting enzyme 2 (ACE2) expression.182,183 In silico investigations reported that andrographolide may block inflammatory regulators that promote virus-induced inflammation, leading to cytokine storms in the host body. 183 Moreover, as a significant component of Andrographis paniculata, andrographolide may exhibit the potential to protect against 3-chymotrypsin-like protease, spike, RNA-dependent RNA polymerase, and papain-like protease of SARS-CoV-2 virus, thereby helping to curb replication, transcription, and host cell recognition. 184
Resveratrol, a natural polyphenol found in grapes, berries, and peanuts, has also demonstrated anti-inflammatory, antioxidant, and antiviral properties against SARS-CoV-2, making it a potential therapeutic agent in the treatment of COVID-19. Resveratrol may mitigate the significant pathways involved in the pathogenesis of SARS-CoV-2, such as the regulation of the renin-angiotensin system, expression of ACE2, stimulation of the immune system and downregulation of pro-inflammatory cytokines release. 185 Xu et al 186 demonstrated that resveratrol was a specific and selective inhibitor of the 3-chymotrypsin-like protease and papain-like protease of SARS-CoV-2 in vitro. Derivatives of resveratrol tested by molecular modeling techniques for COVID-19-mediated drug development produced more promising results than antimalarials such as chloroquine. 187 Several studies have also demonstrated the potential of resveratrol to inhibit the replication of SARS-COV-2 with minimal toxicity.87,188 Figure 4 depicts the chemical structures of the potential anti-SARS-CoV-2 phytochemicals that may serve to complement commercially available drugs. Table 4 further summarizes a list of selected plants with potential anti-SARS-CoV-2 activity.

Chemical structures of quercetin, curcumin, epigallocatechin gallate, andrographolide, and resveratrol.
List of selected plants with potential anti-SARS CoV-2 activity.

Insect Sources of anti-SARS-CoV-2
The SARS-CoV-2 spike glycoprotein is at the center of vaccine research attempts to prevent the coronavirus disease 2019 (COVID-19) pandemic caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). Vaccines, particularly those for SARS-CoV-2, train the immune system to recognize and eliminate a disease-causing pathogen by delivering either a live virus or a dead virus into the body. Injecting messenger RNA, also known as mRNA, which is a genetic code that compels cells in the body to make the spike protein of the virus, or injecting a weakened cold virus to transport the code for the spike protein into the body, where it is turned into spike protein, are 2 of the many methods that can be used to enhance immunity against diseases. Injecting the viral spike protein itself is an alternative method that can be utilized. Neutralizing antibodies primarily target this protein. 203
Nearly 80% of all existing animals are arthropods, which include insects, arachnids, myriapods, and crustaceans.204,205 While other natural sources like plants, fungi, and bacteria were heavily explored for new drugs, insect-derived protease inhibitors have been largely overlooked.206,207 Nevertheless, vaccines containing virus-like particles have been manufactured utilizing various expression systems, including those derived from bacteria, yeast, insects, mammals, and plants. There may be untapped prospects to find new therapeutic options effective toward SARS-CoV-2 main protease (Mpro) among insect-derived protease inhibitors. The advancement of the baculovirus expression vector technology has allowed insect cells to appear as a viable tool. Using the Baculovirus Expression System Technology (BEST), a protein can be created in insect cells; once purified, it can be used as part of a vaccination as a booster in combination with another constituent, an adjuvant. Vaccines against future influenza pandemics, in particular, have had the usage of insect cell expression systems proposed as a more secure method of production. 208
A French pharmaceutical company Sanofi, developed a vaccine against influenza using insect cells. The technology was used to develop a platform for manufacturing influenza H7N9-TW VLPs utilizing insect cells. 209 This platform includes the expression of the hemagglutinin (HA), neuraminidase (NA), and M1 proteins. Novavax has just recently developed a protein subunit vaccine, and the efficacy of the vaccination has been reported as being 89.3%.210,211 This vaccine was developed by genetically modifying a baculovirus to incorporate an altered COVID-19 spike protein gene, which encodes vaccine antigens, allowing the modified virus to infect cultivated Sf9 insect cell lines.210,211 This research resulted in developing of a vaccine for Spodoptera frugiperda. 203 Using an insect cell-based baculovirus expression vector system (IC-BEVS), it was possible to develop a scalable bioprocess for mass-producing S protein stabilized in its pre-fusion conformation for use in a virosome-based COVID-19 vaccine candidate. 212 For a virosome-based COVID-19 vaccine candidate, the highly glycosylated and complex S protein must be produced, and this study demonstrates that IC-BEVS can do so without compromising its structure or antigenicity. According to Li et al, 213 a recombinant COVID-19 vaccine could benefit from using insect cells to produce a SARS-CoV-2 S-protein stabilized in a prefusion trimer. A cell-based approach for reliable detection of patient serum was developed using recombinant baculovirus-infected insect cells. Notably, a newly devised detection technique, in which S-displaying insect cells that act as antigens, detected anti-S antibodies from many patients whose levels had previously been undetectable by Western blotting. According to Wei et al, 214 conformation-dependent anti-S antibodies are the predominant antibody produced by patients with COVID-19.
Honey and its components are being studied extensively as a possible natural medication due to their potential to decrease acute inflammation by increasing the immune response. Its antiviral, antibacterial, and immune-boosting qualities may help patients with COVID-19. 215 Honey and its primary constituents can prevent virus entry into the host cell, halt viral multiplication, and inhibit inflammatory response. 216 The SARS-CoV protein binds to angiotensin-converting enzyme (ACE), and flavonoids have been proven to block ACE in many in vitro and in vivo studies, suggesting that honey and related products may show significant benefits for treating COVID-19. 217 Honey’s antiviral properties stem from its composition, which includes methylglyoxal, copper, ascorbic acid, flavonoids, nitric oxide, hydrogen peroxide, and its derivatives. 218 It contains immune-boosting, autophagic, anti-inflammatory, anti-oxidative, antimicrobial, anti-diabetic, anti-hypertensive, and cardioprotective properties that help it to fight COVID-19. 219 Honey’s antiviral effects against SARS-CoV-2 and its indirect effects on the immune system suggest that it may help mitigate the symptoms of COVID-19 infection. 220 Honeybee products have been shown to have potent antiviral effects against infections that cause severe respiratory syndromes, such as human coronaviruses. These products include honey, pollen, propolis, royal jelly, beeswax, and bee venom. 221 Antibody formation induction, immune cell maturation, and activation of innate and adaptive immunological responses are all functions of bee products.
Because of the abundance and variety of insect-derived protease inhibitors, the ClusPro server has been used to dock SARS-CoV-2 Mpro onto many inhibitors and then designed peptides based on regions with high inhibitory potentials against Mpro. 204 Based on an AutoDock analysis, the peptide 1KJ0-7 synthesized from SGCI (Schistocerca gregaria chymotrypsin inhibitor) has the maximum binding energy and the lowest inhibition constant. Further analysis using Haddock revealed that a different peptide, 2ERW-9, from infestin, a serine protease inhibitor of Triatoma infestans, had the best docking score, binding energy, and dissociation constant for Mpro. The findings from such studies highlight the utility of insect-derived peptides and computational approaches to drug discovery by presenting 2 peptides with promising protease inhibitor activity against Mpro. Neutrophil extracellular traps (NETs) have also been studied as a potential treatment for SARS-CoV-2. NETs are commonly seen in snakes, insects, arachnids, and myriapods.222,223 Though there is potential for drug discovery using insects and insect-related products, more studies through clinical trials are needed to confirm these functions.
Conclusions and Future Prospects
The COVID-19 pandemic brought the world to a standstill, affecting the lives of millions of people worldwide. While traditional control measures such as social distancing, quarantine, and vaccination have played a significant role in combating the virus, other potential contributions from microbes, insects, and plants could be utilized to manage the disease. These alternative solutions could be valuable in reducing the spread of COVID-19 and helping people recover from the disease.
Currently, there are several commercially available drugs for the treatment of COVID-19. One of the most widely used drugs is remdesivir, an antiviral medication that has shown effectiveness in reducing the duration of hospitalization for COVID-19 patients. 224 Another drug commonly used is dexamethasone, a corticosteroid that reduces mortality in severely ill patients requiring oxygen support. 225 Monoclonal antibody therapies, such as bamlanivimab and casirivimab/imdevimab, are also available and authorized for emergency use in specific high-risk individuals. 226 These drugs target specific virus components and helping the immune system fight off the infection. 227
The development of vaccines has been a significant breakthrough in combatting the COVID-19 pandemic. The mRNA vaccines developed by Pfizer and Moderna have been highly effective in preventing severe illness and hospitalization from COVID-19. 228 Other vaccines, such as those developed by AstraZeneca and Johnson & Johnson, have also been effective. 229 The rapid development of these vaccines was made possible by technological advancements and collaborations between researchers, governments, and private industry.
Microbes, such as bacteria, fungi, and viruses, have been used in various ways to combat infectious diseases. For example, bacteriophages have been used to treat bacterial infections, and some viruses have been engineered to target cancer cells. 230 In the case of COVID-19, researchers have identified specific bacteria that could be used to prevent infection or help patients recover from the disease. For example, a recent study found that a nasal spray containing a type of bacteria called Lactobacillus could reduce the severity of COVID-19 symptoms and prevent the spread of the virus. 231
Insects also have the potential to contribute to the fight against COVID-19. For example, researchers have identified that mosquitoes infected with the bacteria Wolbachia are less likely to transmit viruses such as dengue, chikungunya, and Zika. 232 These mosquitoes could be released in areas where COVID-19 is prevalent to reduce the spread of the virus. Furthermore, certain insects, such as ants and termites, produce antimicrobial compounds 233 that could be used to develop new treatments for COVID-19. Also, insect-derived protease inhibitors are promising potential therapies for SARS-CoV-2. 234 Targeting specific viral proteases can inhibit viral replication and reduce the severity of COVID-19 symptoms.
Plants are another potential source of new treatments for COVID-19. Many plants produce antimicrobial compounds, such as the plant extract artemisinin, used to treat malaria. 235 Researchers have identified several plants that contain compounds that could be used to treat COVID-19. For example, a study found that extracts from the herb. Andrographis paniculata could reduce the replication of the COVID-19 virus in cells. 182
While these potential contributions from microbes, insects, and plants are exciting, much work must be done to fully understand their potential applications in the fight against COVID-19. Further research is needed to determine the safety and effectiveness of these alternative solutions, and regulatory approval would be necessary before they could be used to treat patients. Additionally, it is vital to consider the potential environmental impacts of releasing insects or plants into the environment.
In addition to the traditional public health strategies of testing, tracing, and isolating infected individuals, new control and management strategies have emerged to combat the virus. One of the most notable new strategies is the development of digital contact tracing apps. These apps use Bluetooth technology to detect other users close to the user and can alert them if they have been exposed to the virus. 236 By quickly identifying potential exposures, contact tracing apps can help reduce the spread of the virus and contain outbreaks. However, these apps have concerns about privacy and data security, and their effectiveness depends on widespread adoption. 237
Another strategy implemented to reduce the spread of the virus is wastewater surveillance. Researchers have found that wastewater can contain traces of the virus, even in asymptomatic individuals, making it a valuable tool for the early detection and monitoring of outbreaks. 238 Public health officials can analyze wastewater samples to identify areas where the virus spreads and take appropriate measures to contain it.
Mask mandates have also been implemented in many places to reduce the spread of the virus. Masks are an effective tool for preventing the transmission of respiratory viruses, including SARS-CoV-2, and can reduce the risk of infection for both the wearer and those around them. 239 However, mask mandates have been controversial in some areas, and compliance can be challenging. 240
Technological advancements have played a crucial role in managing the COVID-19 pandemic. For example, artificial intelligence and machine learning have been used to analyze large amounts of data to identify potential treatments for COVID-19. 239 Researchers have used these technologies to identify existing drugs that may be effective against the virus and to develop new treatments and vaccines. 239
Telemedicine has also become increasingly popular during the pandemic. With many hesitant to visit healthcare facilities in person, telemedicine allows patients to receive medical care remotely. 240 This reduces the risk of exposure to the virus and ensures that patients can still receive the care they need. Telemedicine has been used for various healthcare services, from routine check-ups to mental health consultations. 240
Footnotes
Acknowledgements
We thank Frederick Leo Sossah for his insightful comments and contributions to earlier versions of this manuscript.
Funding:
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contribution
AKD: Study-conceived and designed, Writing-original draft, Review & Editing; NKAQ, AFO, BOB, AK, AFA, SMA, SKL, WE, JHNO, OFA: Writing-original draft, Review & Editing; MJO: Review & Editing.