
Abstract
Background:
Histologic subtyping of lung cancer has significant implications for treatment planning. Accurate diagnosis based on cytology/small biopsy specimens is challenging and frequently determined by morphology, as material is often not sufficient for immunohistochemical studies (IHC). We investigated the concordance between the rates of diagnosis from cytology/small biopsies compared with surgical specimens in patients with squamous cell lung cancer (SCC) and the utility of IHC for diagnostic precision in lung cancer subtyping.
Methods:
We conducted a 5-year retrospective analysis identifying cases of SCC diagnosed on cytology/small biopsies ± IHC and compared them with subsequent surgical specimens when available. The number of patients with SCC on surgical biopsy and the concordance between cytology ± IHC was determined.
Results:
Over the 5-year period (2011-2015), 231 cases were identified. Surgery was performed on 66 cases (28.5%), of which 87.9% concurred with cytological diagnosis (95% exact binomial confidence interval [CI] = 77.5%-94.6%). There were 36 cases diagnosed in 2014 and 2015 with IHC data. Of those cytology cases with IHC (n = 12), SCC was confirmed by surgery in 91.7% (95% CI = 61.5%-99.8%). Of those without IHC (n = 24), 95.8% were confirmed SCC by surgery (95% CI = 78.9%-99.9%). These rates were not different (Fisher exact test). All cases with IHC were morphologically squamous.
Conclusions:
Our data demonstrate that diagnostic precision of identifying SCC by cytology/small biopsy is comparable with or without additional IHC studies. We recommend judicious use of IHC on cytology specimens, reserving it for cases where cytomorphology is equivocal. Tissue should be preserved for molecular analysis, which may have therapeutic implications.
Introduction
The treatment for non-small cell lung cancer (NSCLC) has evolved over the past decade due to a more comprehensive understanding of pathophysiology, identification of targetable driver mutations, and advances in the field of immune-oncology. These have led to a shift in the treatment of advanced lung cancer from a broad-spectrum chemotherapy approach to a therapy tailored to each individual.
The emergence of next-generation sequencing (NGS) has changed the landscape of lung cancer therapeutics. The NGS is of paramount importance in nonsquamous cell NSCLC, but in recent years, DNA sequencing has revealed an array of potentially actionable gene altering mutations in patients with squamous cell carcinoma (SCC) as well.1,2 Through NGS techniques, mutations in TP63, PIK3CA, SOX2, CCND1, FGFR, KEAP1, and STK11 have been identified in patients with SCC. 3 Alterations in the FGFR have been identified in up to 20% of SCC, 4 making it the most frequently altered tyrosine kinases receptor family in the SCC subtype of NSCLC. 2 Clinical trials with agents targeting this pathway are currently underway and early results are promising. Another major area of development in lung cancer treatment in the last decade is the emergence of checkpoint inhibitors (CPIs) which have changed the treatment landscape for lung cancer patients whose tumors lack driver mutations. 5 Tissue-based biomarkers such as programmed death ligand 1 (PD-L1) 6 and tumor mutation burden (TMB) have been shown to predict response to CPI in both squamous and nonsquamous NSCLC. 7
Hence, to optimally treat lung cancer today, ideally tumor specimens obtained for diagnosis should not only undergo morphological evaluation but also immunohistochemical (IHC) testing as well as NGS to permit a personalized approach. Frequently, there is limited tumor material, especially if the biopsy is performed through endobronchial or transthoracic needle aspiration. It is imperative to exercise tissue stewardship on small samples to conserve sufficient material for molecular and immunologic studies. 8
A systematic analysis showed that diagnostic accuracy of cytology specimens vary widely between studies, but, in general, the accuracy of SCC was much higher than that of adenocarcinoma. 9
In approximately 2-thirds of patients with NSCLC for who diagnosis is made on small biopsies of fine needle aspirate, it is possible to diagnose SCC and adenocarcinoma based on morphology alone and/or a limited IHC panel. 10
When the diagnosis is not established morphologically, IHC can provide clinically meaningful and cost-effective results quickly. 11 Optimal IHC plays a role in differentiating between histologies, and can sometimes be used as a tool to detect certain biomarkers that aid in therapeutic decision-making, such as IHC for anaplastic lymphoma kinase (ALK) fusions and PD-L1 expression. 12 Often times in patients with NSCLC, reflex testing for IHC staining for TTF-1, p40, Napsin, neuroendocrine markers, and ki-67 is used to avoid delays in diagnosis. 10 However, this practice is not ideal and has the risk of exhausting the tissue sample without leaving sufficient material for NGS and predictive markers for immunotherapy such as PD-L1 and TMB. 13 At our institution, we use a step-wise algorithm for diagnosis of SCC as depicted in Figure 1.
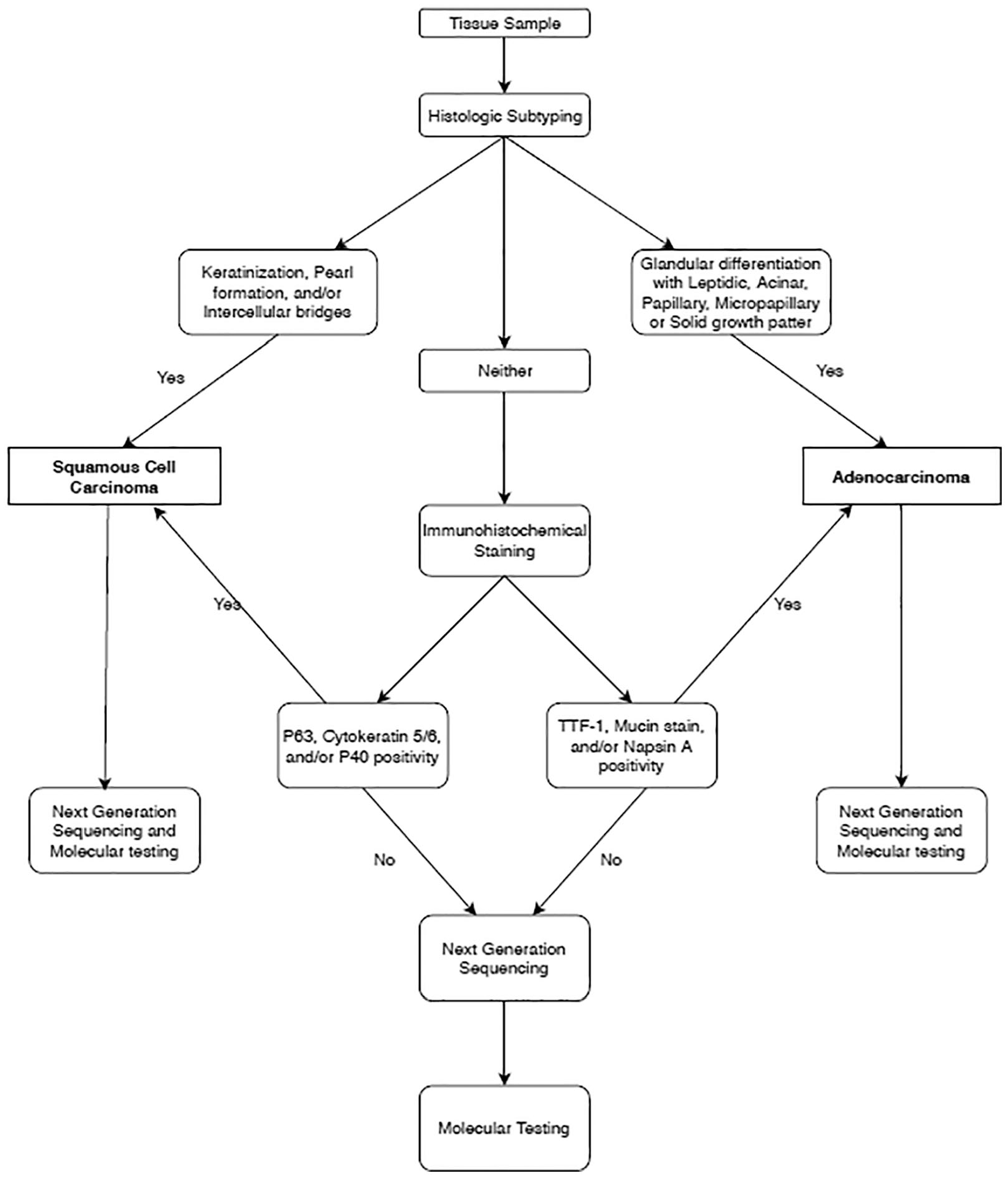
A step-wise approach to diagnosing lung cancer subtype.
In this retrospective study conducted at Northwell health Cancer Institute, we evaluated the diagnostic concordance between small biopsies and surgical specimens in patients with cytological diagnosis of squamous cell lung cancer.
Methods
We conducted a 5-year retrospective analysis identifying cases of SCC diagnosed on cytology/small biopsies and compared them with subsequent matched surgical specimens when available. The concordance rates of diagnosis from cytology/small biopsies when compared with the gold standard surgical biopsies were assessed along with confidence intervals. We further assessed the ability of cytomorphology alone and cytomophology with immunohistochemistry in making the diagnosis of SCC over a period of 2 years, 2014 and 2015. We selected this time period for the additional analysis because the beginning of 2014 marked the roll-out of electronic medical records at our institution allowing us to easily capture accurate, and complete data.
Results
Over the 5-year period (2011-2015), we identified 231 cases of SCC diagnosed on small core biopsy specimens or cytology (Table 1). Subsequent surgical resection or surgical biopsy was performed on 66 cases (28.5%). Overall, there was an 87.9% concordance with cytological diagnosis (95% exact binomial confidence interval [CI] = 77.5%-94.6%). Eight out of 66 cases were deemed nonsquamous on the evaluation of subsequent surgical specimen. For 1 patient, diagnosis was amended to small cell carcinoma, 5 to adenocarcinoma, 1 to large cell, and 1 to high-grade neuroendocrine not otherwise specified (NOS). There were 36 cases diagnosed in 2014 and 2015. Of the cytology cases where IHC was used (n = 12), SCC was confirmed by surgery in 91.7% (95% CI = 61.5%-99.8%). Of those cases where diagnosis was established based on cytomorphology alone without IHC (n = 24), 95.8% were confirmed to be SCC on surgical specimen, (95% CI = 78.9%-99.9%). These rates were not statistically different based on Fisher exact test. Cell blocks were saved for future NGS analysis for all patients in this study.
Findings of patients with SCC diagnosed over a 5-year retrospective period.
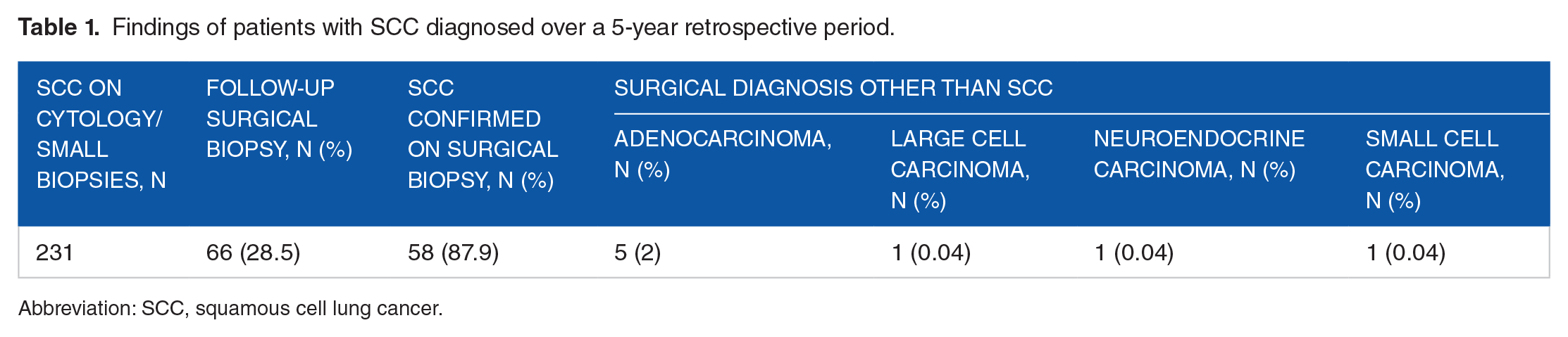
Abbreviation: SCC, squamous cell lung cancer.
These figures compare favorably with those reported in similar studies. 14 As expected, diagnosis made on cytology specimens without IHC was confirmed in surgical specimens with a higher rate than the diagnosis made on cytology specimens with IHC studies. The explanation is that the cases where IHC were used are much more challenging cases due to factors such as poorly differentiated morphology, scanty specimens, and presence of necrosis. In addition, sampling phenomenon in form of sampling bias and tumor heterogeneity is avoided in surgical specimens, and more adequate tissue is available for IHC with definitive interpretation. In patients who underwent subsequent surgical resection or surgical biopsies, a diagnosis of SCC was made based on histomorphology alone in 30 cases and IHC was used for 36 cases. All cases with IHC were morphologically described as squamous.
Discussion
In our study, we focused on SCC diagnosed on tissue obtained from fine needle aspiration compared with surgical biopsies. We used a step-wise approach (Figure 1) to obtain the diagnosis with the aim of preserving tissue material for future studies.
In our study, there was a high level of concordance between diagnosis based on small biopsies or cytology specimens and that based on surgical specimens. Our sample size was small making power calculations not feasible. Similar findings have been reported by others, a study entitled investigated the accuracy of fine needle aspiration in NSCLC compared with histologic analysis. In 85% of the cases, a diagnosis was established by cytological analysis alone and there was an 88% concordance between cytological and histological typing. 14
Key morphologic features like keratinization, pearl formation, and/or intracellular bridges confirms the diagnosis of SCC without further need for IHC analysis. 15 In this case, the remaining material should be sent for molecular testing. However, if there is no clear morphology to suggest the diagnosis of SCC, further analysis by IHC is recommended. Transcription factor 1 and p63 are the 2 principal markers to classify either adenocarcinoma or SCC subtype.9,15 If SCC is confirmed by the presence of p63/40 and/or cytokeratin type 5/6 and absence of TTF-1, Napsin A, and Mucin stain, the remaining sample should be sent for NGS (Picture 1). If the diagnosis is still unclear after NGS, further molecular analysis should be obtained.9,15
After analyzing the data from our study and reviewing the current published literature, we believe that following the algorithm to diagnose SCC in lung cancer, depicted in Figure 1, ensures the best use of tissue stewardship. Making the most of each specimen permits further molecular testing, which could yield targetable mutations that may open more therapeutic options for each patient.

Squamous cell carcinoma (A, B, C): (A) cytomorphology, (B) p40, and (C) p63. Adenocarcinoma (D, E, F): (D) Cytomorphology, (E) TTF-1, and (F) Napsin.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration Of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
CO was mainly in charge of writing the manuscript. NS and IP collected and analyzed the data and helped review the manuscript. MA provided the pictures and helped interpret the findings in the results.