
Abstract
Bioactive sphingolipid is clearly relevant to lung physiology. The relationship of the bioactive sphingolipid pathway to pulmonary disease has been studied in cellular, tissue, and animal model, including lung cancer models. The samples of 53 patients diagnosed with nonsmall cell lung carcinoma (NSCLC) between June 2009 and May 2014 at our hospital were analyzed. Immunohistochemical (IHC) analysis was performed. The degree of immunostaining was reviewed and scored. Using this method of assessment, we evaluated the IHC score of sphingosine kinase 1 (SPHK1), vimentin, E-cadherin, and Ki-67. Both invasive adenocarcinoma cell and squamous cell carcinoma cell were well stained by SPHK1, and fibroblasts were also well stained by SPHK1. Although the IHC score of SPHK1 was not significantly differed between invasive adenocarcinoma and squamous cell carcinoma, the IHC scores of fibroblast, vimentin, and Ki-67 were higher in squamous cell carcinoma than invasive adenocarcinoma. Correlation among IHC scores in each of invasive adenocarcinoma and squamous cell carcinoma was performed. SPHK1 had positive correlation with both fibroblast and Ki-67, and fibroblast and Ki-67 had also positive correlation in invasive adenocarcinoma. On the contrary, SPHK1 had no significant correlation with fibroblast, and had negative correlation with Ki-67 in squamous cell carcinoma. Although there was not significant prognostic difference in SPHK1 score (P = .09), IHC score high group tended to be worse on relapse-free survival. SPHK1 might be prognostic factor in lung-invasive adenocarcinoma and novel target for drug against lung-invasive adenocarcinoma.
Introduction
Lung cancer represents a leading cause of cancer-related mortality and morbidity worldwide. Two major types of lung cancer, small cell lung carcinoma (SCLC) and nonsmall cell lung carcinoma (NSCLC). 1 The most common subtypes of NSCLC include adenocarcinoma and squamous cell carcinoma. Current available treatment strategies for NSCLC, including surgery, radiotherapy and chemotherapy, remain generally unsuccessful. While SCLC usually reveals better responsiveness to chemotherapy and radiation, NSCLC is relatively insensitive to both therapeutic modalities. Hence, identification of novel targets for more effective anti-NSCLC strategies with minimal toxicity is urgent.
Sphingolipids are family of membrane lipids that have structural roles in the regulation of the fluidity and subdomain structure of the lipid bilayers. Furthermore, bioactive sphingolipids, such as sphingosine-1-phosphate (S1P) and ceramide, are signaling molecules involved in the activation of pathways that are directly relevant to carcinogenesis. S1P activates multiple intracellular signaling cascades by binding specific G-protein-coupled receptors and promotes inflammation, cell proliferation, tumor growth, and metastasis, whereas ceramides have anticancer properties by promoting apoptosis, growth arrest, and senescence.
Sphingosine kinase (SPHK) phosphorylates sphingosine to S1P, and is therefore an important regulator of the levels of ceramide, sphingosine, and S1P. In theory, upregulating SPHK should upregulate S1P, and therefore enhance cell survival and proliferative capacity. Two functional SPHK isoenzymes, SPHK1 and SPHK2, have been identified in human.2-4 The enzymes differ in their tissue distribution, with SPHK1 messenger ribonucleic acid (mRNA) expression at its highest in the lung, spleen, and peripheral blood leukocytes, 5 whereas SPHK2 mRNA is expressed highest in the liver, brain, and heart. 3 SPHKs could be activated by numerous external stimuli, including tyrosine kinase growth factors, tumor necrosis factor-α, and G-protein-coupled receptor ligands.5-12 There has been a considerable body of evidence suggesting that SPHK1 can act as an implicated in the induction of cell survival and proliferation, inhibiting of apoptosis, and promotion of tumor progression in mice, whereas SPHK2 has been implicated in arresting cell growth and promoting apoptosis.13-16 Inhibiting or down-regulating SPHK1 could decrease cell proliferation and arrest the cell cycle in glioblastoma cells and breast cancer cells, and a dominant-negative form of SPHK1 was able to suppress tumor formation in nude mice.17-19 Moreover, SPHK1 has been found to be upregulated in several tumor types, such as glioblastoma multiform, intestinal adenoma, acute erythroleukemia, prostate cancer, gastric cancer, and colon cancer.19-23
Recently, bioactive sphingolipid is clearly relevant to lung physiology. The relationship of the bioactive sphingolipid pathway to pulmonary disease has been studied in cellular, tissue, and animal model, including lung cancer models.24-26
In this study, we characterized the SPHK1 expression in NSCLC and evaluated correlation between SPHK1 expression and prognosis.
Materials and Methods
Patients and tissue specimens
Paraffin-embedded, representative NSCLC samples were obtained from 53 patients diagnosed with NSCLC between June 2009 and May 2014 at the department of thoracic surgery at Kanazawa Medical University. The smoking history was assessed using the Brinkman index, which is calculated as the numbers of cigarettes smoked per day multiplied by the number of years for which the subject has smoked. The histologic characterization and clinicopathological staging of the samples were determined according to the world health organization (WHO) criteria and current International Union Against Cancer tumor-node-metastasis (TNM) classification. Pathological factors were the histological type, differentiation, lymphatic invasion (Ly), vascular invasion (V), pathological stage (pStage). In the part of samples, paired samples of fresh normal lung tissues and lung cancer tissues from same patient were collected by the department of pathology in Kanazawa Medical University and were stored at −70°C until use.
Immunohistochemistry
Immunohistochemical (IHC) analysis was performed to study altered protein expression in 53 human NSCLC tissues. Paraffin-embedded specimens were cut into 4 μm sections and baked at 65°C for 30 min. The sections were deparaffinized with xylenes and rehydrated. Sections were submerged into Tris-ethylenediaminetetraacetic acid antigenic retrieval buffer and heated for 5 min at 121°C by autoclave. The sections were treated with 3% hydrogen peroxide in methanol to quench the endogenous peroxidase activity followed by incubation with 1% bovine serum albumin to block the nonspecific binding. Rabbit anti-SPHK1 (1:25 dilution; Sigma) was incubated with the sections overnight at 4°C. After washing, the tissue sections were treated with biotinylated antirabbit secondary antibody (Zymed) followed by a further incubation with streptavidin-horseradish peroxidase complex (Zymed). The tissue sections were then immersed in 3,3′-diaminobenzidine and counterstained with 10% Mayer’s hematoxylin, dehydrated, and mounted. IHC analysis of vimentin, E-cadherin, and Ki-67 were performed by Labeled Streptavidin-Biotin Method.
The degree of immunostaining was jointly reviewed and scored jointly by 2 observers based on the proportion of positively stained tumor cells and intensity of staining. The proportion of positively stained tumor cells was graded as follows: 0 (no positive tumor cells), 1 (<10% positive tumor cells), 2 (10-50% positive tumor cells), and 3 (>50% positive tumor cells). The cells at each intensity of staining were recorded on a scale of 0 (no staining), 1 (weak staining, light yellow), 2 (moderate staining, yellowish brown), and 3 (strong staining, brown). The staining index was calculated as follows: staining index = staining intensity × proportion of positively stained tumor cells. Using this method of assessment, we evaluated the IHC score of SPHK1, vimentin, E-cadherin, and Ki-67 in NSCLC by staining index (scored as 0,1,2,3,4,6, or 9). Cutoff values to define the high and low expression of SPHK1 were chosen based on a measure of heterogeneity with the log-rank test statistics with respect to overall survival. An optimal cutoff value was identified. The IHC score ⩾6 was used to define tumors with high expression, and IHC score ⩽4 as tumor with low expression of SPHK1.
Western blotting
Protein concentration was determined by Bradford assay (Bio-Rad Laboratories). Equal amounts of proteins were applied to 9% polyacrylamide SDS gels (SDS-PAGE), separated electrophoretically, and transferred onto polyvinylidene fluoride membranes (Amersham Pharmacia Biotech). The membrane was incubated with anti-SPHK1 rabbit antibody (1:80, Cayman). SPHK1 expression was detected with horseradish peroxidase-conjugated goat antirabbit IgG (1:3000; Amersham Pharmacia Biotech) and an enhanced chemiluminescence kit (Amersham Pharmacia Biotech) according to the manufacturer’s instructions. Anti-β-actin antibody (1:10 000 dilution; Sigma) was used as the loading control.
Statistical analyses
The cumulative survival rates were calculated by the Kaplan-Meier methods, and survival curves were compared using the log-rank test. All statistical analyses were 2-sided, and statistical significance was defined as a P value of less than .05. The statistical analyses were conducted using the JMP software program (Version 13.2; SAS Institute Inc., Cary, NC, USA).
This study was conducted in accordance with the amended Declaration of Helsinki. The Institutional Review Boards of Kanazawa Medical University approved the protocol (approval number: I392), and written informed consent was obtained from all of the patients.
Results
Patients characteristics
The clinicopathologic characteristics of the 53 included patients are listed in Table 1. Thirty patients were men, and the median age was 71 years. The median Brinkman index was 380, the median carcinoembryonic antigen (CEA) was 3.5 ng/mL. The pStage was IA in 21, IB in 20, IIA in 6, IIB in 3, and IIIA in 3. Adenocarcinoma was diagnosed in 37 and squamous cell carcinoma in 16. Differentiation was divided into 3 categories: grade 1 (G1) in 10, grade 2 (G2) in 35, and grade 3 (G3) in 8. Ly was present in 28 patients, and V was present in 30.
Patient characteristics.

Abbreviations: AD, adenocarcinoma; CEA, carcinoembryonic antigen; Ly, lymphatic invasion; pStage, pathological stage; SPHK1, sphingosine kinase 1; SQ, squamous cell carcinoma; V, vascular invasion.
Immunohistochemistry
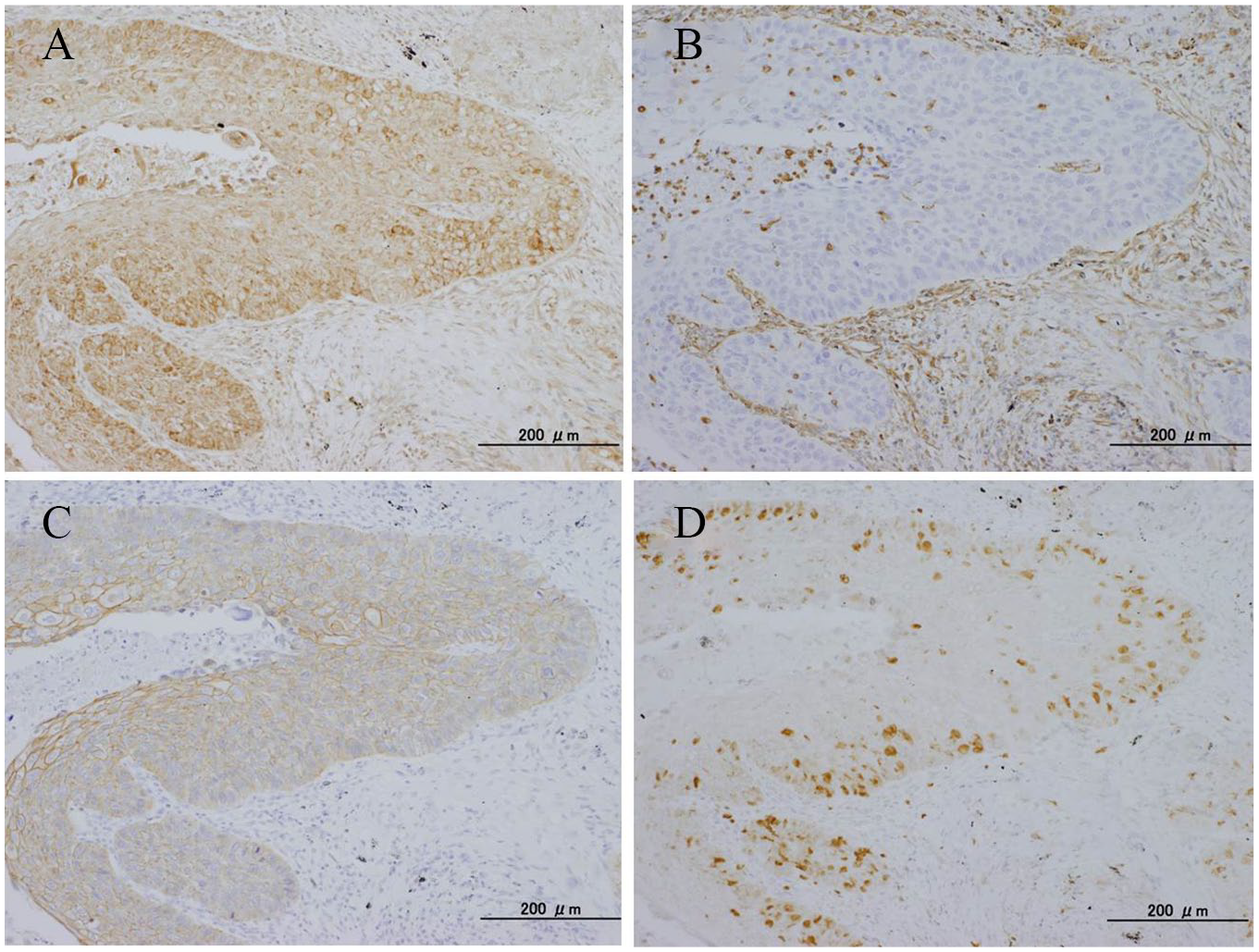
Both invasive adenocarcinoma cell and squamous cell carcinoma cell were well stained by SPHK1, and fibroblasts were also well stained by SPHK1 (Figures 1A and 2A). The IHC score of SPHK1, fibroblast, vimentin, E-cadherin, and Ki-67 were scored by staining index (Table 1). Furthermore, the comparisons of the IHC score of SPHK1, fibroblast, vimentin, E-cadherin, and Ki-67 between adenocarcinoma and squamous cell carcinoma were performed (Table 2). Although the IHC score of SPHK1 was not significantly differed between invasive adenocarcinoma and squamous cell carcinoma, the IHC scores of fibroblast, vimentin, and Ki-67 were higher in squamous cell carcinoma than invasive adenocarcinoma. On the contrary, the IHC score of E-cadherin was higher in adenocarcinoma. Correlation among IHC scores in each of invasive adenocarcinoma and squamous cell carcinoma was performed (Table 3). SPHK1 had positive correlation with both fibroblast and Ki-67, and fibroblast and Ki-67 had also positive correlation in invasive adenocarcinoma. On the contrary, SPHK1 had no significant correlation with fibroblast and had negative correlation with Ki-67 in squamous cell carcinoma.

Immunohistochemistry in invasive adenocarcinoma: (A) sphingosine kinase 1, (B) vimentin, (C) E-cadherin, and (D) Ki-67.
Immunohistochemistry in squamous cell carcinoma: (A) sphingosine kinase 1, (B) vimentin, (C) E-cadherin, and (D) Ki-67.
Comparison immunohistochemistry score between adenocarcinoma and squamous cell carcinoma.

Abbreviations: AD, adenocarcinoma; SPHK1, sphingosine kinase 1; SQ, squamous cell carcinoma.
Correlation among immunohistochemistry scores in each of invasive adenocarcinoma and squamous cell carcinoma.

Abbreviation: SPHK1, sphingosine kinase 1.
Western blotting
Western blotting for SPHK1 in NSCLC was shown in Figure 3. SPHK1 expression was detected at 52 kDa in both adenocarcinoma and squamous cell carcinoma.

Western blotting for sphingosine kinase 1 in invasive adenocarcinoma and squamous cell carcinoma.
Survival analyses
The survival rate is shown in Figure 1. Although there was not significant prognostic difference in SPHK1 score (P = .09), IHC score high group tended to be worse on relapse-free survival (Figure 4A). Overall survival was also not significantly different in SPHK score (P = .15, Figure 4B).

Survival curve of invasive adenocarcinoma grouped by sphingosine kinase 1 score: (A) relapse-free survival and (B) overall survival. SPHK1 indicates sphingosine kinase 1.
Discussion
The key findings made in this study are 2. First, there are the differences of correlation among IHC scores in between invasive adenocarcinoma and squamous cell carcinoma. Although the IHC score of SPHK1 was not significantly differed between invasive adenocarcinoma and squamous cell carcinoma, the IHC scores of fibroblast, vimentin, and Ki-67 were higher in squamous cell carcinoma than invasive adenocarcinoma. SPHK1 had positive correlation with Ki-67, and fibroblast and Ki-67 had also positive correlation in invasive adenocarcinoma. Furthermore, SPHK1 tended to correlate with fibroblast in invasive adenocarcinoma. In recent study, it was reported that cancer-associated fibroblasts modify lung cancer metabolism involving ROS and TGF-β signaling. 27 On the contrary, SPHK1 had no significant correlation with fibroblast and had negative correlation with Ki-67 in squamous cell carcinoma. Based on this result, the expression of SPHK1 in lung-invasive adenocarcinoma might be related with invasion and cell proliferation but that in lung squamous cell carcinoma might not. Recently, compelling evidence has linked SPHK1 up-regulation to cancer development and progression,28,29 and the up-regulation of SPHK1 has been revealed in several types of solid tumor, including glioblastoma, intestinal adenoma, acute erythroleukemia, prostate cancer, and colon cancer.19-23 It was reported that the induction of SPHK1 expression could be mediated by various mechanisms. For example, numerous growth factors and oncogenes, including platelet-derived growth factor, epidermal growth factor, nerve growth factor, glial cell line-derived neurotropic factor, BCR/ABL, and hypoxia-inducible factor-1α, were shown to upregulate SPHK1 through activation of the cis-acting element in the SPHK1 promoter, such as the hypoxia-inducible factor-responsive elements, the SP1 motifs, via multiple signaling pathway, the phosphoinositide 3-kinase pathway, and the Janus kinase 2 pathway.30-37 Increased expression of SPHK1 has been found to enhance the antiapoptotic ability of the MCF-7 breast cancer cells, increase cell proliferation, and promote estrogen-dependent tumorigenesis.15-17 Ectopic expression of SPHK1 could promote G1S transition and stimulate cell growth, colony formation in soft agar, and tumor growth in immunodeficient mice.13,19 Overexpression of SPHK1 elevates the expression of cyclooxygenase-2 in colon cancer. 23
Second of the key findings of this study is that SPHK1 might be related with recurrence of lung-invasive adenocarcinoma. It was reported that SPHK1-induced epithelial mesenchymal transition (EMT) in lung adenocarcinoma cell line. 38 Furthermore, it has been suggested that S1P promotes EMT in cancer by remodeling the glycocalyx and inhibiting the Snail-matrix metalloproteinases signaling pathway. 39 EMT is believed to ultimately promote tumor metastasis by promoting the migration of tumor cell across the basement membrane and their invasion into the surrounding microenvironment.40,41 Understanding the mechanism underlying EMT has profound results with regard to the responsiveness of a tumor to a range of available treatment. Recently, it was reported that microRNA-506-3p inhibited the expression of SPHK1 and the treatment of SPHK1 inhibited the EMT. 42
Previous study showed that SPHK1 plays an important role in antiapoptosis of NSCLC that is relatively insensitive to chemotherapy, both in vivo and in vitro. 43 Furthermore, it was reported that high SPHK1 expression is associated with shorter overall survival and increased risk of disease relapse in patients with NSCLC treated with adjuvant chemotherapy in recent study. 44 Ectopic expression of SPHK1 in NSCLC cells dramatically enhances their resistance to apoptosis induced by doxorubicin or docetaxel, 2 commonly used chemotherapeutics, whereas suppressing SPHK1 expression with small-hairpin RNAs or inhibiting SPHK1 activity with a specific SPHK1 inhibitor (SK1-I) markedly abrogated the ability of NSCLC cells to resist cytotoxic reagent-induced cell death, suggesting that SPHK1 activity contributes to sustaining the unwanted survival of NSCLC cells under the treatment of chemotherapeutics. In fact, injection of SK1-I potently enhanced the tumor suppression effect to docetaxel, a clinically well-established, proapoptotic chemotherapy drug against breast, ovarian, and NSCLC.45,46 Furthermore, it was recently reported that high SPHK1 mRNA expression is significantly correlated to worse OS in NSCLC patients. 47 In the future, SK1-I might become an important drug of chemotherapy for NSCLC.
Several limitations associated with this study warrant mention. First, the study is retrospective and small sample size, and there is a possibility of unobserved cofounding and selection bias. Second, this study was performed at a single institution.
In conclusion, the results of this study demonstrate that SPHK1 might be a prognostic factor in lung-invasive adenocarcinoma and a novel target for drug against lung-invasive adenocarcinoma.
Footnotes
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Kanazawa Medical University (grant no. S2016-17).
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
N.M. performed the research, and collected and wrote the paper. Y.U. and M.S. contributed to diagnose the pathological status and analyze. S.I., Y.I., and K.U. contributed to sample collection. H.U. contributed to supervision of this study and revision of the manuscript.
Patient Consent to Publication
Consent for publication was obtained from the patient.