
Abstract
Meningiomas are tumors arising from leptomeninges. Malignant counterpart of them is known as anaplastic meningioma which are WHO grade III tumors. Intraventricular location of these tumors is rare and is clinic-radiologically challenging. Histopathology and immunohistochemistry are confirmatory. We present case of a 27-year-old girl, who presented with usual symptoms of intraventricular mass in emergency. After shunt surgery, clinical diagnosis of ependymoma was formed with differential of high-grade glioma. Squash tissue was difficult to crush displaying tight clusters of spindle cells with necrosis in background. Definitive histology revealed high grade spindle cell neoplasm disposed in sheets with brisk and atypical mitosis. Only focal whorling pattern was seen. Large cells with eccentric cytoplasm, reminiscent of rhabdoid cells were also seen. Immunohistochemistry was positive for vimentin and EMA, negative for GFAP. Final diagnosis of Anaplastic meningioma was dispatched. The histological pattern of the present case, young age of presentation and presence of Rhabdoid cells make it unusual. Though rare but intraventricular meningiomas must also be kept in clinical radiological differentials apart from the usual ependymoma at this location.
Keywords
Introduction
Meningioma is commonly a benign neoplasm which arises from leptomeninges. It accounts for 20% of all brain neoplasms. 1 It is usually seen intracranially but extracranial meningiomas have been reported as well. Within intracranial locations intraventricular meningiomas are rarely seen. They only account for approximately 0.5% to 3.7% of intracranial meningiomas.2-4 Interestingly the intraventricular meningioma is not attached to the duramater. They usually arise in the lateral ventricle most commonly in trigone. They may also arise from choroid plexus or tela choroidea.2-5
Intraventricular meningiomas are usually asymptomatic initially until they become large enough to produce pressure symptoms. Pressure symptoms caused can be obstructive hydrocephalus or compression of vitals areas in cerebral cortex resulting in sensory motor dysfunction or optic chiasm atrophy or seizures. The intraventricular location is challenging surgically because of proximity to vitals sensorimotor areas in cerebral hemispheres including optic area, language area, motor, and sensory cortical area. 2
Even in 2021 WHO classification of CNS neoplasms meningiomas are graded in 3, namely Grade 1 (benign), 2 (intermediate) and 3 (malignant or anaplastic). 6 Moreover, 15 cytomorphological and histological variants have also been recognized. 80% of meningiomas are benign which are managed by surgical resection and 10 years survival rate is 90% to 96%. Fifteen percent to 18% tumors are of WHO grade 2 and only 2% to 4% are in WHO grade 3 or anaplastic. Intraventricular anaplastic (Grade 3) meningioma accounts for only <1% of all meningiomas. 7
Anaplastic meningiomas have high recurrence rate and aggressive growth. Surgical resection is not curative for these tumors. These tumors have poor prognosis with 10 years survival rate of 14% to 34%.8,9
In the present case report, we discuss the presentation, diagnosis and management of an intraventricular meningioma which turned out to be WHO grade 3. The clinical presentation and the diagnostic and radiological challenges faced in the present case make it interesting. The diagnosis and age of presentation makes it rare.
Clinical Summary
Clinical history and examination
An apparently asymptomatic 27 years right-handed lady, educated up to intermediate presented in emergency with headache, vomiting for 15 days, multiple episodes of Generalized tonic clonic seizures (GTCS) for 10 days and altered sensorium for 4 days. Her headache was usually nocturnal and got relieved with vomiting. On physical examination, she was conscious but disoriented although occasionally following commands. Fundus examination revealed grade 5 papilledema and rest of the central nervous system (CNS) examination could not be elicited.
Radiology
Emergency computed tomography (CT) reflected a well-defined heterogenous space occupying lesion with necrotic areas (Figure 1a) displaying mass effect over third ventricle with bilateral lateral ventricle dilatation and trans ependymal cerebrospinal fluid (CSF) ooze. Contrast magnetic resonance imaging (MRI) following stabilization revealed a well-defined extra axial intraventricular heterogeneously enhancing soft tissue lesion of around 4 cm × 3 cm × 4 cm with internal necrotic areas (Figure 1b), epicenter was at third ventricle. T1 hyperintense lesion showed blooming on SW1 reflecting hemorrhage within. The lesion was found to abut bilateral basifrontal lobe, thalami, and optic chiasma.
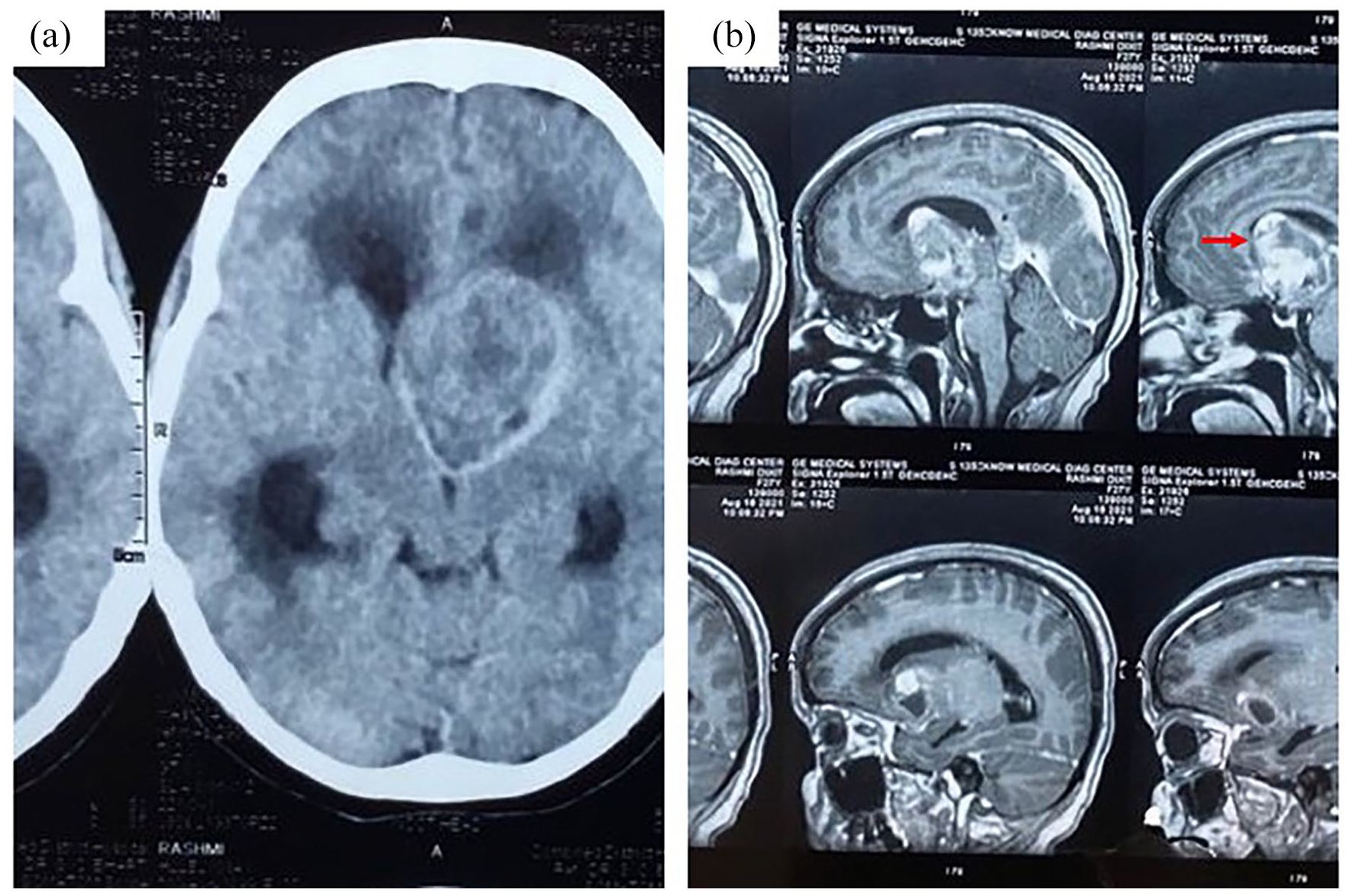
Radiological picture of the lesion CT plain image in (a) displaying well circumscribed lesion with heterogenous areas. MRI contrast image in (b), sagittal section shows smooth outline of tumor (arrow) with altered signals.
Management
She underwent Emergency CSF diversion procedure. Provisional diagnosis of ependymoma with differential of glioma was made as per clinical and radiological findings. She was planned for definitive surgery and underwent Left Frontoparietal craniotomy with ultrasound guided tumor localization and subtotal excision of tumor with extra ventricular drain (EVD) insertion. Inoperative the tumor was grayish white, firm in consistency, mildly vascular, easily breakable, and partially suck able.
Pathological Findings
Intraoperative tissue was not easily squashable, with tight clusters of spindle cells in background of necrosis (Figure 2a). Focal whorl pattern and one psammomatous calcific like deposit was seen. In view of moderate nuclear pleomorphism, clumped chromatin, necrosis, meningioma was reported, possibly high grade (Figure 2b). On discussion with operating team possibility of ependymoma was also not completely denied and rest was differed for histology.

Cytology images show tumor disposed in tight clusters (a; H&E×100) with spindled cells displaying coarse chromatin and moderate pleomorphism (b; H&E×200). Follow-up histology shows tumor disposed in sheets (c; H&E×200) focal whorl formation. On higher magnification nuclear anaplasia, mitosis (arrow) is seen (d; H&E×400). Inset shows cells with rhabdoid morphology.
Hematoxylin and eosin-stained tissue section from the processed tissue displayed a neoplasm disposed predominantly in sheets and intersecting fascicles with focal whorl formation (Figure 2c). Brisk mitosis was noted (30/10 hpf) with atypical forms. Nuclear atypia was evident (Figure 2d). Few cells were large and displayed eccentric nuclei with dense cytoplasm; overall percentage area of these cells was less than 5% of total tumor area. These cells were morphologically thought to be either dedifferentiated rhabdoid cells or gemistocytes (Figure 2d inset).
On basis of morphology, radiology and clinical findings following differentials were considered in the given order (1) gliosarcoma, (2) anaplastic meningioma, and (3) anaplastic ependymoma. Further immunohistochemistry was performed (Figure 3a-e). The tumor cells were positive for Vimentin, and negative for GFAP and synaptophysin. Ki67 was 50%. EMA displayed diffuse cytoplasmic expression rather than dot like golgi zone seen in ependymoma. Desmin highlighted the large, atypical cells with eccentric nuclei suggesting that they were rhabdoid cells. Finally, it was reported as anaplastic meningioma WHO Grade 3.

Immunohistochemistry images show no immunoexpression for GFAP in a, diffuse expression for both vimentin and Cytokeratin in b and c. Desmin highlights the rhabdoid cells in d. Ki67 is high as seen in e. (IHC×200).
The case underwent radiological review. The smooth outline of the tumor and contour suggested that it was intraventricular meningioma indeed rather than previously reported glioma with differential of ependymoma. The patient however succumbed to complications related to secondary infection of the shunt surgery.
Discussion
Lateral ventricle is the most common site of intraventricular meningiomas followed by third and fourth ventricles. Tumors located at these sites are usually seen on left side and approximately 90% at the trigone region. 10 Radiologically the present tumor was quite large occupying both lateral ventricles along with third as well. However, the epicenter was suggested in third ventricle.
Symptomatically lateral intraventricular anaplastic meningioma produces symptoms due to pressure either due to (1) increase in intracranial pressure or (2) direct pressure on brain parenchyma. The symptoms thus produced include headache, vision defect, seizures, cognition impairment, ataxia, amnesia as seen in the present case. 1
Meningiomas at this location can be diagnosed by radiological imaging (CT and MRI) and histopathology is confirmatory. The radiology has been described in literature as hyperdense with contrast enhancement. It may have calcification in some areas. On MRI these lesions are isointense or hypointense on T1W images and hyperintense on T2W images with strong contrast enhancement. The heterogeneous signal areas or hypointense areas signify tissue necrosis, intratumoral hemorrhage or cystic changes within tumor. These hypointense areas were due to necrosis in this case. MR Spectroscopy can be of help in this scenario. It reveals raised alanine to phosphocreatinine ratio in meningiomas. However, in the present case it was also not helpful as it suggested a glial lesion. The plausible reason could be the high-grade nature of lesion with extensive necrosis. 11
The intraoperative cytology was effective as it was the first investigation which pointed toward the actual diagnosis, unpredicted clinico- radiologically. The unsquashable nature of the tissue, tight spindle cell cluster, small psammomatous like calcification and vague whorling supported the morphological opinion. Mostly squash cytology confirms already made radiological and clinical diagnosis. Still, it multiple times leads to totally surprising results and guides toward correct management. 12
Spindle cell intracranial lesion with high grade morphological features have few differentials like gliosarcoma, anaplastic meningioma, high grade ependymoma or metastatic/primary sarcoma. Both ependymoma and glioma have a fibrillary background and display GFAP expression on immunohistochemistry. Meningioma on the other hand is GFAP negative and display both EMA and vimentin expression. EMA expression is seen in ependymomas as well, but its localization is in Golgi zone. The expression seen is dot like contrasting to cytoplasmic expression evident in meningiomas.
Rhabdoid differentiation in meningiomas is well known and signifies high grade lesions. 13 According to WHO classification of tumors of central nervous system, meningioma with rhabdoid cells and morphological features of malignancy is classified as Rhabdoid meningioma. There is no mention of any cutoff as far as the percentage are of rhabdoid cell distribution is considered. 6 Vaubel et al 14 in their study had semi quantitively scored presence of rhabdoid cells as <20% versus 20%-50% versus >50%. They suggested that meningiomas with rhabdoid features should be classified analogous to their non rhabdoid counterpart. In the present tumor even though malignant features were seen with rhabdoid cells it was not labeled as rhabdoid meningioma as the percentage area was too small and the cells were present in few foci only.
Few cases of anaplastic meningiomas have been reported in literature.5,15-18 All these anaplastic or grade 3 meningiomas reported have found to be arising from lateral ventricle and commonly from right trigone. This contrasts with the radiological location of present case. Moreover, in all these cases patients were from ages 40 or above. The age of presentation of our patient was very young that is 27 years. This makes the present reported case a rarer occurrence.
Main treatment modality of these tumors is surgical. Tumors can be approached surgically via several routes depending upon location of tumor, for example, transcallosal approach, transcortical, parieto occipital, transtemporal approach. Lateral ventricle trigone tumors are best approached via parieto-occipital transcortical approach. Role of radiotherapy as an adjuvant treatment is controversial. It was observed in studies that radiotherapy is effective to prevent progression of primary or recurrent meningioma. 19 Chemotherapy has been used mainly for recurrent tumors after surgical and radiation treatment.
Multiple complications of intraventricular surgeries have been reported including subdural hygroma, intracranial hemorrhage, postoperative seizure, infection, and hydrocephalus. Nosocomial infections being resistant and difficult to manage. 20 Unfortunately, our patient succumbed to the complications related to the shunt placed.
Conclusion
Intraventricular anaplastic meningioma is a rarely seen malignant tumor. They are aggressive in nature and show high degree of recurrence. Rhabdoid differentiation and young age of presentation is even rarer. Though rare but meningiomas must be kept in clinical radiological differentials apart from the usual ependymoma at intraventricular location.
Footnotes
Acknowledgements
We are thankful to King George’s Medical University for providing the infrastructure to perform our work.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Contributions
Data Availability
All data generated or analyzed during this case are included in this article. Further enquiries can be directed to the corresponding author.