
Abstract
Background:
Sexual health is a crucial determinant of overall quality of life (QOL), encompassing physical, psychological, and interpersonal well-being. Female sexual dysfunction (FSD) is a multifactorial condition involving disturbances in desire, arousal, orgasm, and sexual pain. Despite affecting up to 40% of women globally, as reported in epidemiological studies, FSD remains underreported and inadequately addressed due to sociocultural barriers and limited awareness.
Objective:
To explore FSD through a comparative analysis of contemporary biomedical science and Ayurvedic principles, focusing on an integrative perspective and management approaches.
Methods:
A narrative review was conducted using classical Ayurvedic texts and contemporary scientific literature retrieved from PubMed, Scopus, and Web of Science. Relevant articles published between 2010 and 2026 were screened using predefined inclusion and relevance criteria, focusing on psychosexual, neurobiological, and Ayurvedic perspectives.
Results:
Conventional management includes pharmacological agents, hormonal therapies, and psychosexual counseling, although outcomes are often variable due to heterogeneity in response and potential adverse effects. Ayurvedic concepts, including vajikarana and apraharsha bhava, offer a holistic approach emphasizing mind-body interactions. Certain behavioral approaches described in classical texts parallel psychosexual mechanisms involving neuroendocrine and limbic pathways. Additionally, vrishya dravyas (aphrodisiac substances) are traditionally described to support reproductive and psychological health, although current clinical evidence remains insufficient.
Conclusion:
An integrative model combining contemporary biomedical insights with Ayurvedic principles may offer a more comprehensive and culturally contextual understanding of FSD. However, further clinical and translational research is required to validate these correlations and establish evidence-based applications.
Introduction
Sexual health is a fundamental component of overall quality of life (QOL), influencing physical, psychological, and relational well-being. Disturbances in sexual function may result in stress, emotional imbalance, reduced selfesteem, anxiety, and impaired interpersonal relationships. In women, these disturbances commonly present as female sexual dysfunction (FSD), a spectrum of conditions involving impairments in sexual desire, arousal, orgasm, and sexual pain. Epidemiological studies suggest that approximately 40% of women report sexual problems, although only a subset experience clinically significant distress.1,2
FSD is a complex condition with multifactorial etiology, involving biological, psychological, and social determinants. Neurohormonal regulation, vascular function, mental health status, and relational dynamics all contribute to sexual functioning. Despite its high prevalence, FSD remains underrecognized and underreported due to sociocultural stigma, lack of awareness, and limited clinical dialogue. 3 Conventional management strategies include pharmacological, hormonal, and psychosexual interventions; 4 however, these approaches often show variable efficacy and may not holistically address the condition.
In this context, traditional systems of medicine such as Ayurveda offer a broader perspective for understanding sexual health. The principles of vajikarana (aphrodisiac therapy) and the concept of apraharsha bhava (absence of sexual excitation) provide insights into the psychophysiological dimensions of sexual dysfunction. This review presents a comparative and integrative analysis of FSD by examining parallels and distinctions between contemporary biomedical science and Ayurvedic perspectives. Despite advances in pharmacological and psychotherapeutic interventions, a comprehensive integrative framework addressing neurobiological, psychosocial, and culturally contextual dimensions of FSD remains insufficiently explored.
This review proposes an integrative model that bridges neurobiological mechanisms with traditional Ayurvedic constructs.
Methodology
Study Design
This study is a narrative review aimed at synthesizing concepts of FSD from both contemporary biomedical science and Ayurvedic literature.
Data Sources and Search Strategy
A comprehensive literature review was conducted using electronic databases (PubMed, Scopus, and Web of Science) to retrieve articles from 2010 to 2026. Classical Ayurveda texts, including Charaka Samhita, Sushruta Samhita, Ashtanga Hridayam, and the Kamasutra of Vatsayayana, along with their authoritative commentaries, were also reviewed.
Search terms included: “FSD,” “hypoactive sexual desire disorder (HSDD),” “psychosexual health,” “Ayurveda,” “vajikarana.”
A total of approximately 85 articles were included after screening for relevance and removing duplicates.
Inclusion and Exclusion Criteria
Articles were included if they:
Addressed female sexual desire or arousal disorders Discussed psychosexual or neurobiological mechanisms Explored Ayurvedic concepts related to sexual health Included pharmacological or non-pharmacological interventions
Articles lacking relevance to the study objective were excluded.
Analytical and Translational Approaches
Analytical and translational approaches were used to identify correlations between Ayurvedic principles, and a translational methodology was applied to map these principles to modern psychosexual frameworks. This involved an interpretative analysis of Sanskrit terminology, contextual correlation, and interdisciplinary synthesis.
Psychosexual and Neurobiological Basis of Female Sexual Desire Disorders
Sexual Response Cycle and Desire Regulation
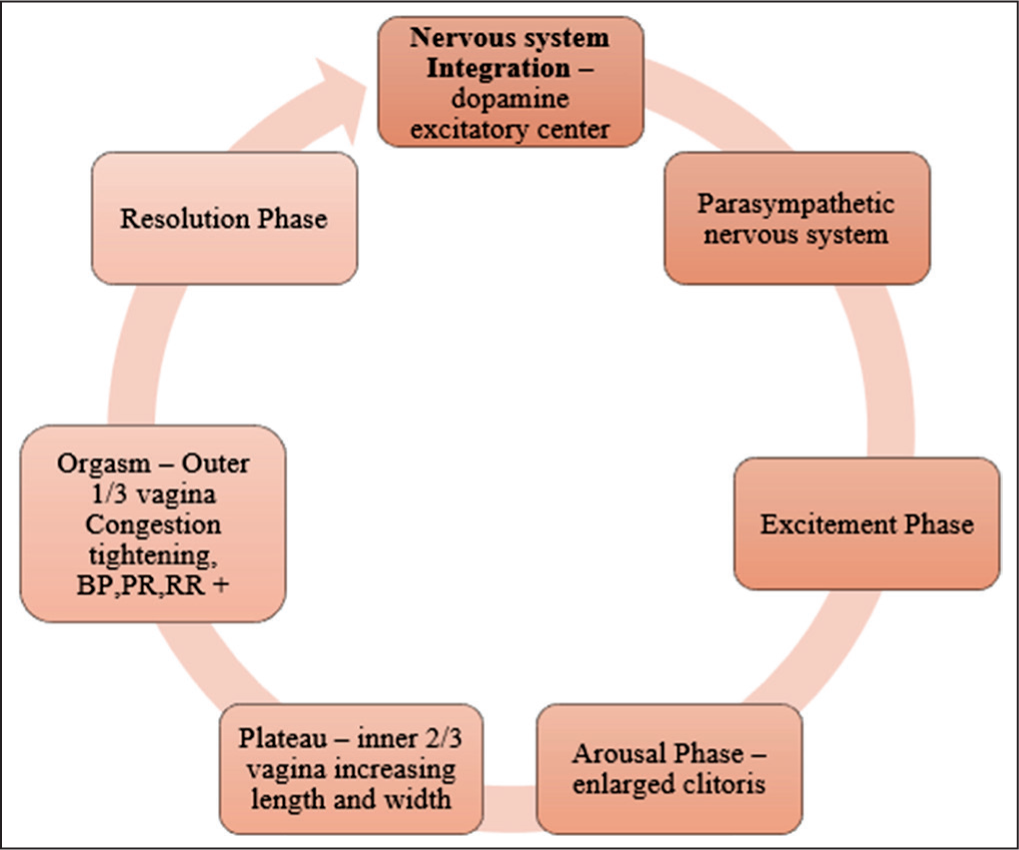
The female sexual response cycle is a dynamic and non-linear process influenced by physiological, psychological, and relational factors. To describe the sexual response, Masters and Johnson proposed a four-phase model comprising excitement, plateau, orgasm, and resolution. 5 Despite its historical significance, this model does not fully capture the complexity and variability of female responses.
Neuroendocrine Mechanisms of Sexual Desire
Sexual response in both men and women typically begins with the desire phase, which is regulated by a balance between excitatory and inhibitory neural pathways. Dopaminergic activity within the mesolimbic system plays a central role in motivation and reward, facilitating sexual desire, whereas serotonergic pathways exert an inhibitory effect. 6
The arousal phase is primarily mediated by the parasympathetic nervous system, leading to increased genital blood flow and engorgement. This includes enlargement of the clitoris, dilation of paravaginal arterioles, and expansion of the inner two-thirds of the vagina, referred to as the tenting effect. Estrogen contributes to this process by promoting transudation across the vaginal mucosa, thereby facilitating lubrication. 7
The plateau phase represents a continuation of sexual arousal, during which the level of sexual excitement is sustained before orgasm. At this stage, the inner two-thirds of the vagina further expands, while the outer one-third becomes congested with blood, forming the “orgasmic platform.”
The orgasmic phase is characterized by rhythmic contractions of pelvic floor muscles, accompanied by increases in heart rate, blood pressure, and respiratory rate. This is followed by the resolution phase, during which the body gradually returns to a baseline, unaroused state. Unlike men, women may not have a well-defined refractory period, allowing the possibility of multiple orgasmic responses. 7
As illustrated in Figure 1, these physiological changes reflect the coordinated interaction of neural and vascular mechanisms.
Role of Psychological and Relational Factors
Psychological well-being is a key determinant of sexual desire. Conditions such as depression, anxiety, and chronic stress are known to impact libido and sexual responsiveness. Additionally, interpersonal factors, including communication, emotional intimacy, and partner satisfaction, play a critical role in shaping sexual experiences.
The biopsychosocial model emphasizes the integrated influence of biological, psychological, and relational factors in the development and persistence of FSD.5,6
Classification of Female Sexual Dysfunction
According to the revised DSM-5 classification, female sexual interest/arousal disorder is classified as a combined disorder of desire and arousal. It is characterized by a significant reduction or absence of sexual interest and/or arousal, including both subjective excitement and genital response.
The diagnosis requires the presence of at least three of the following symptoms, persisting for a minimum duration of six months, and associated with clinically significant distress.
8
Absent or reduced interest in sexual activity Absent or reduced sexual or erotic thoughts or fantasies Reduced initiation of sexual activity and typically unreceptive to a partner’s attempts Absent or reduced sexual excitement or pleasure during sexual activity in most encounters Reduced sexual interest or arousal in response to internal or external erotic stimuli Reduced genital or non-genital sensations during sexual activity.
For descriptive and comparative purposes, FSD has also been traditionally categorized into the following domains:
Sexual desire disorders:
HSDD: Characterized by persistent or recurrent deficiency or absence of sexual fantasies and desire for sexual activity, associated with personal distress. Sexual aversion disorder: Marked by persistent or recurrent phobic aversion to sexual contact, leading to avoidance behavior and distress. Sexual arousal disorder: Persistent or recurrent inability to attain or maintain adequate sexual excitement. Orgasmic disorders: Characterized by delayed, infrequent, or absent orgasm following sufficient sexual stimulation. Sexual pain disorders:
Vaginismus: Recurrent or persistent involuntary contraction of vaginal musculature interfering with penetration. Dyspareunia: Recurrent or persistent genital pain associated with sexual intercourse, with reported prevalence ranging from 14% to 18%.
9
Pathophysiology of Female Sexual Arousal
Female sexual arousal involves the coordinated interaction of neural, vascular, and hormonal mechanisms, as described in Section 3. Disruption of this coordinated system contributes to the development of FSD.
At a functional level, sexual arousal depends on effective neurovascular integration, resulting in genital vasocongestion, lubrication, and associated extragenital responses. Impairment at any level of this integrated system may lead to arousal dysfunction.9–12
The Key Pathophysiological Mechanisms Include
Neurotransmitter imbalances: Altered dopaminergic and serotonergic activity affecting sexual motivation and reward pathways.
Neuroendocrine dysregulation: Chronic stress-related activation of the hypothalamic-pituitary-adrenal (HPA) axis, potentially suppressing reproductive hormonal function.
Hormonal imbalance: Reduced levels of estrogen, testosterone, or progesterone contribute to impaired libido and arousal.
Vascular factors: Endothelial dysfunction and reduced genital blood flow affecting arousal responses.
Psychological factors: Depression, anxiety, interpersonal conflict, and prior sexual trauma influence sexual responsiveness.12–15
Understanding Through Ayurveda
Concept of Sampraharshana (Sexual Excitation Cycle)
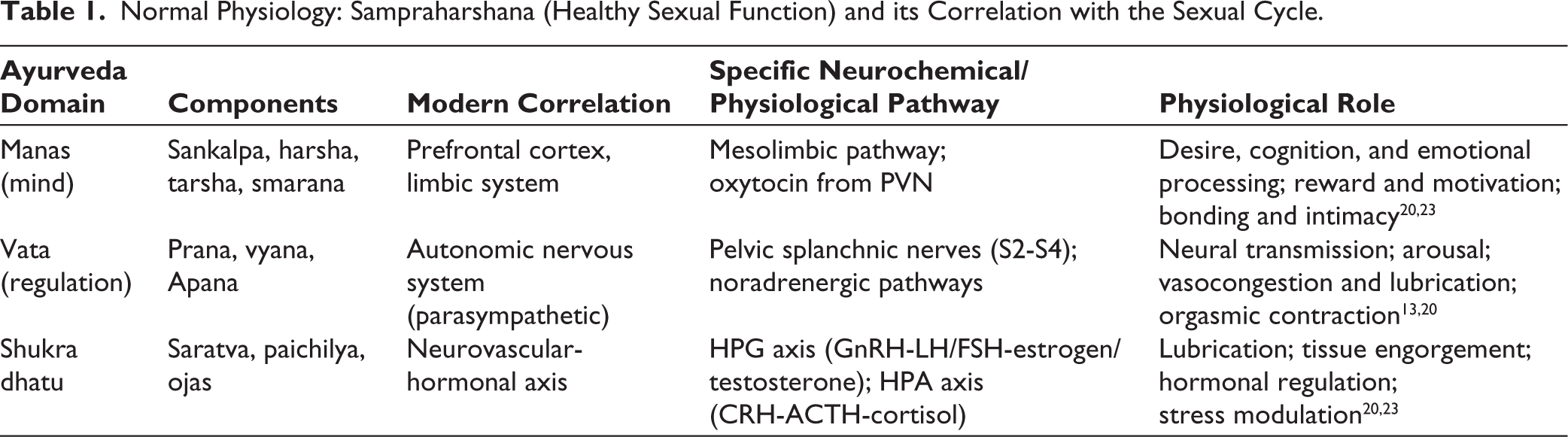
Healthy sexual function is the coordinated interaction of neurochemical, hormonal, vascular, and psychological factors. In Ayurveda, a comparable concept is described as sampraharshana, referring to the state of sexual excitation or activation. This process is understood as a dynamic interaction between mental intention (sankalpa), sensory stimulation, and the functional integrity of vata dosha, which governs movement and regulation within the body.16,17
Sampraharshana may be understood as a psychophysiological process in which cognitive and sensory inputs contribute to the initiation and progression of sexual response. However, such interpretations represent conceptual parallels and should not be regarded as claims of direct biological equivalence. 16
Role of Manas (Mind) in Sexual Desire
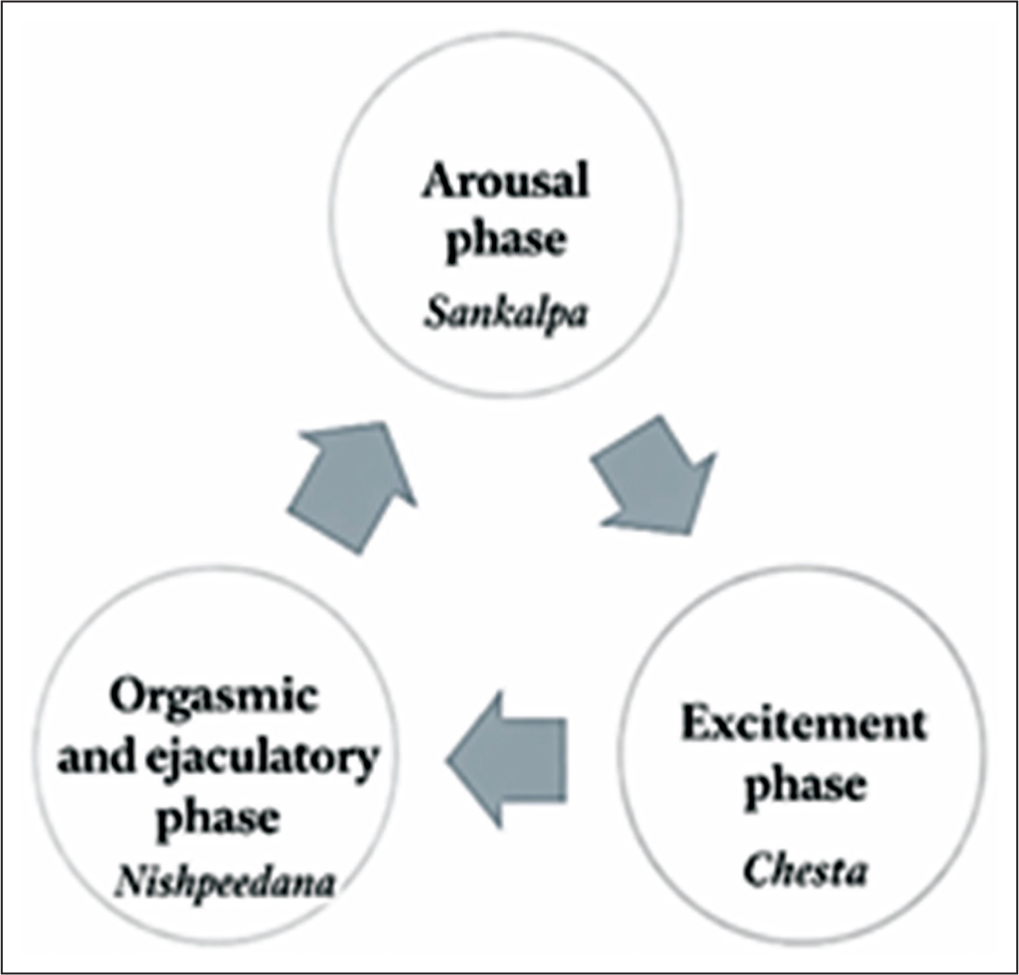
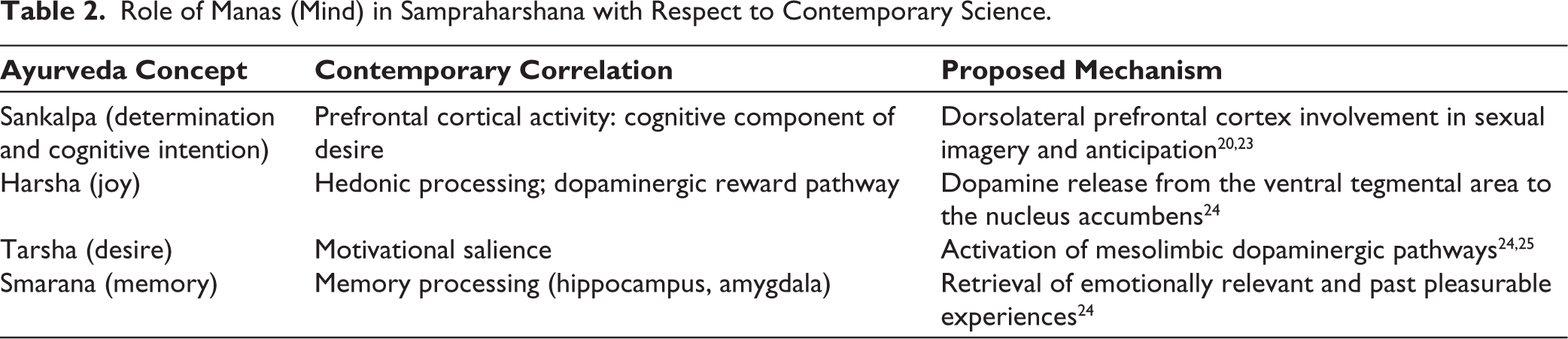
In Ayurveda, manas (mind) plays a central role in regulating sexual desire, perception, and emotional engagement. The initiation of sexual activity is influenced by various mental states, including sankalpa (intention), harsha (joy), tarsha (desire), smarana (memory), and adhyavasaya (determination). Additionally, behavioral and interpersonal expressions such as chesta (activity), guhyabhashana (intimate communication), kreeda (play), keertana (praise), and nishpeedana (physical interaction) are described as facilitators of sexual engagement.18,19
The Involvement of Vata in the Sexual Cycle
Vata dosha, particularly its subtypes, is considered to play a regulatory role in the sexual response cycle. Prana vata is associated with neural functions and sensory perception, vyana vata with circulation and vascular responses, and apana vata with pelvic functions, including orgasmic release, and reproductive processes.16,20
These functional descriptions may relate to neural transmission, hemodynamic changes, and pelvic neuromuscular activity observed in contemporary physiology. However, these associations should be interpreted cautiously, as Ayurvedic concepts are qualitative and system-based rather than directly anatomical or biochemical.
The sexual response cycle described in Ayurveda is illustrated in Figure 2.
Sexual Cycle in Terms of Ayurveda.
Shukra Dhatu and Ojas: Reproductive and Vital Essences
In Ayurveda, shukra dhatu is considered the reproductive tissue associated with vitality, regeneration, and reproductive capacity. It is described as contributing to sampraharshana bhava (state of sexual excitation), which is regarded as essential for reproductive function and overall sexual well-being.
Psychological and emotional factors such as harsha (joy), praharsha (enhanced pleasure), preeti (affection), and bala (strength) are described as influencing the functional expression of shukra. These factors highlight the close interrelationship between mental states and reproductive function in Ayurvedic thought.
Ayurvedic texts also describe shukra as being present throughout the body, with systemic regulation involving hrudaya (heart), which is considered central to coordinating rasa, shukra, ojas, manas, and vata. This may reflect a holistic view in which physiological and psychological processes are interdependent.
The functional expression of shukra is further characterized by qualitative attributes such as saratva (fluidity), paichilya (unctuousness), gourava (heaviness), pravana bhava (tendency to flow), and drutatva (quickness), modulated by the action of vata. Additionally, harsha (excitement) and tarsha (desire) emphasize the role of psychological activation in sexual response. These descriptions may reflect the integration of psychological, fluid, and dynamic aspects of reproductive function. However, such interpretations represent conceptual frameworks rather than direct physiological correlates.20–22
The relationship between these factors and the sexual response cycle is illustrated in Table 1, with the role of manas further detailed in Table 2.
Normal Physiology: Sampraharshana (Healthy Sexual Function) and its Correlation with the Sexual Cycle.
Role of Manas (Mind) in Sampraharshana with Respect to Contemporary Science.
Pathology of FSD
The normal sexual response cycle, as discussed from both contemporary and Ayurvedic perspectives, reflects a coordinated interaction of physiological and psychological processes. Disruption of this integration may lead to FSD. Ayurveda offers a conceptual framework to understand such disturbances through the notion of apraharsha bhava, which denotes the absence or reduction of sexual excitement and pleasure. Apraharsha bhava is described as a state characterized by diminished ananda (joy) and harsha (sexual excitation). This condition is influenced by factors such as dehabala (physical strength), sattvabala (mental resilience), and vrushattva (sexual capacity). The interplay among these factors may act as a determinant of overall sexual function, suggesting that impairment in either physical or manasika domains can contribute to dysfunction.22,26
The initiation and maintenance of sexual activity depend on coordinated sensory perception, mental engagement, and physiological responsiveness, which are governed by the functional integrity of vata dosha. Disturbances in motivation, intention, or emotional readiness to engage in sexual activity may therefore contribute to impaired sexual response.
Psychological Factors (Manasika Bhavas)
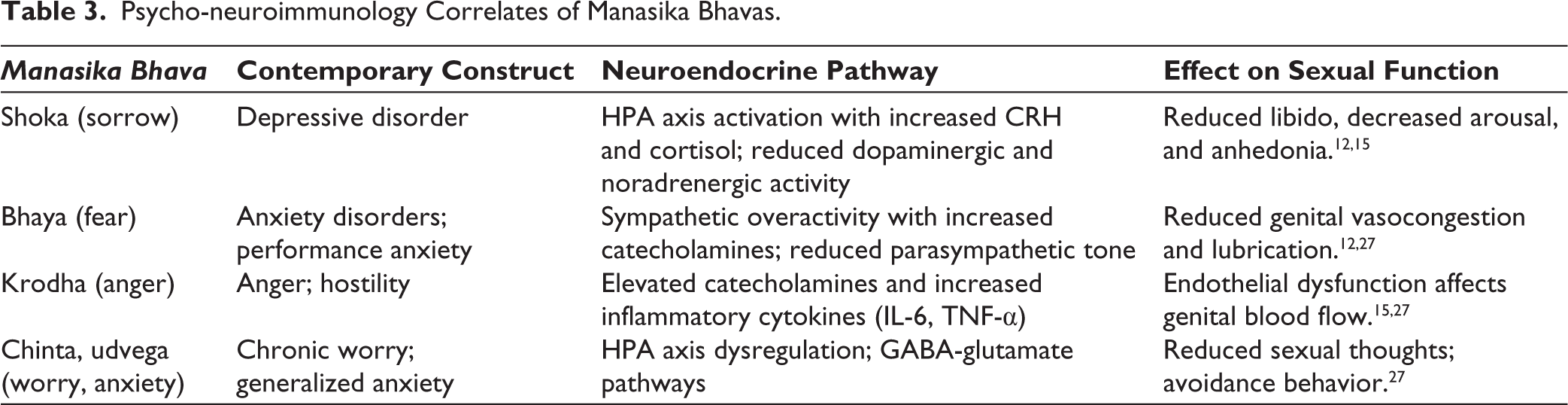
The role of manasika bhavas (psychological states) is emphasized in Ayurveda as a key determinant of sexual function. Emotional states such as shoka (sorrow), bhaya (fear), krodha (anger), chinta (worry), and udvega (anxiety) are described as negatively influencing desire and arousal.
Shoka, being antagonistic to harsha, may contribute to reduced sexual interest and diminished emotional engagement. Similarly, bhaya and chinta may lead to mental distraction and performance-related anxiety, thereby impairing sexual responsiveness. Krodha and bhaya are also described to provoke pitta dosha, which, when aggravated, may affect shukravaha srotas (channels associated with reproductive function), leading to functional disturbances.
These descriptions may align with contemporary understanding of the impact of psychological stressors, such as depression, anxiety, and emotional conflict, on neuroendocrine regulation and sexual function.21,26
The role of these psychological factors in relation to contemporary mechanisms is further elaborated in Table 3.
Psycho-neuroimmunology Correlates of Manasika Bhavas.
Interpersonal and Sociocultural Factors
Interpersonal dynamics between partners, including communication quality, emotional intimacy, and relational conflict, play a significant role in the development of apraharsha bhava. Ayurvedic literature emphasizes the concept of “soumanasya garbha lakshyate,” which highlights the importance of a harmonious mental state between partners for successful conception and healthy sexual interaction.
This concept underscores the role of praharsha bhava (sexual excitement) as a prerequisite for maithuna kriya (sexual activity), facilitated through components such as sankalpa (intention), chesta (effort), and nishpeedana (physical engagement). These elements may be conceptually aligned with contemporary perspectives that emphasize emotional intimacy, cognitive readiness, and mutual responsiveness as key determinants of healthy sexual function.17,26
Management
Conventional Management
Conventional management of HSDD primarily focuses on pharmacological and hormonal interventions targeting neurotransmitter pathways, endocrine balance, and genital hemodynamics. 28 Among pharmacological agents, flibanserin, a centrally acting serotonergic modulator, and bremelanotide, a melanocortin receptor agonist, are approved for the treatment of HSDD. These agents have shown modest efficacy in improving sexual desire; however, their use is often limited by variable efficacy and potential adverse effects.29,30
Hormonal therapies, including transdermal testosterone, estrogen, tibolone, and vaginal dehydroepiandrosterone, are employed to address hormonal deficiencies and improve genital symptoms such as vaginal dryness and discomfort. 31
In addition, off-label pharmacological options such as bupropion, buspirone, and sildenafil have been explored to enhance sexual desire and arousal, particularly in cases associated with selective serotonin reuptake inhibitor-induced dysfunction. 32
Other agents, including oxytocin, ginseng, Ginkgo biloba, and L-arginine, have also been investigated; however, current evidence supporting their efficacy remains limited and inconclusive. 19
Non-pharmacological interventions such as cognitive behavioral therapy, mindfulness-based therapy, and couple-based sex therapy have demonstrated potential effectiveness in certain contexts in addressing psychogenic and relational aspects of FSD. 33
Overall, while conventional therapies provide symptomatic benefit in selected populations, their effectiveness may be constrained by heterogeneity in response, adverse effects, and limited long-term data. This highlights the need for more comprehensive and individualized approaches to management.
Ayurvedic Therapeutic Framework
In Ayurveda, manas (mind), which governs perception and cognition, is considered integral to overall health and is functionally associated with atma (consciousness). The management of disorders involving psychophysiological components, such as FSD, is approached through three principal therapeutic modalities:
Yuktivyapashraya chikitsa (rational therapy): Includes pharmacological and non-pharmacological interventions based on logical and clinical reasoning. Daivavyapashraya chikitsa (spiritual therapy): Encompasses faith-based and ritualistic practices aimed at restoring manasika balance. Sattvavajaya chikitsa (psychological therapy): Focuses on the regulation of the mind through behavioral and cognitive approaches.
Within this framework, manaso harshanam (promotion of mental satisfaction and excitation) is considered fundamental and is achieved by strengthening dhi (intellect), dhriti (emotional control), and smriti (memory), which collectively contribute to improved psychological resilience and cognitive balance.20,26
Behavioral and Non-pharmacological Correlates
Classical texts such as the Kamasutra of Vatsyayana describe various non-pharmacological approaches to enhance sexual arousal, including alingana (embracing), kissing, gentle tactile stimulation (lalita-sparshana), and playful interaction. These practices emphasize sensory engagement and interpersonal connection, which may contribute to improved arousal and emotional intimacy. 34
From a contemporary perspective, such tactile interactions may involve activation of afferent C-tactile fibers, which respond to gentle, slow stroking. These fibers project to the insular cortex and are linked to affective touch processing, potentially facilitating oxytocin release and enhancing bonding, relaxation, and sexual receptivity. 27 However, these correlations are interpretative and should be understood as conceptual parallels rather than direct physiological equivalence.
Environmental Factors (Kamottejaka Bhavas)
Ayurveda highlights the role of kamottejaka bhava
Such factors may be conceptually aligned with contemporary understanding of contextual modulation of sexual arousal through sensory integration and limbic system activation. In particular, olfactory inputs have direct connections to the amygdala and hypothalamus, which may influence emotional and sexual responses.21,27
Guidelines for Sexual Activity
Classical Ayurvedic texts emphasize the importance of preparedness, mutual readiness, and environmental comfort in sexual activity. Recommendations include engaging in intercourse in a relaxed mental state, after appropriate nourishment, and within a pleasant and comfortable setting. 18
These guidelines reflect an understanding of the influence of psychological and contextual factors, such as emotional state, stress, and interpersonal harmony, on sexual function. Such principles are broadly consistent with contemporary approaches in sex therapy, which emphasize communication, emotional intimacy, and reduction of performance-related anxiety. 24
Pharmacological Interventions
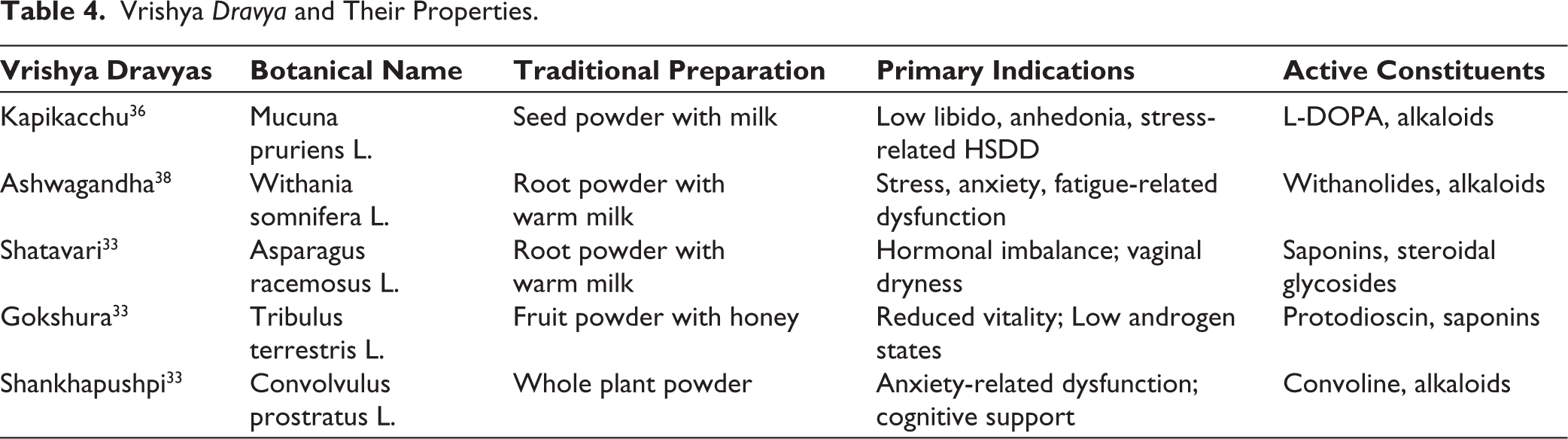
The use of vrishya dravyas (aphrodisiac formulations) is described in Ayurveda as part of the management of sexual dysfunction, with an emphasis on enhancing physical vitality, reproductive function, and psychological well-being. These agents are traditionally considered to promote harshanam (sexual excitation) and improve overall sexual capacity.
Classical texts, including those of Acharya Bhavamishra, describe several vrishya dravyas, such as kapikacchu (Mucuna pruriens L.), gokshura (Tribulus terrestris L.), ashwagandha (Withania somnifera L.), shankhapushpi (Convolvulus prostratus L.), mushalikanda (Chlorophytum borivilianum), shatavari (Asparagus racemosus L.), and varahi kanda (Dioscorea bulbifera L.), which are traditionally used in conditions associated with reduced libido and stress.35–38
These agents may exert effects through multiple pathways, including neuroendocrine modulation, stress reduction, and improvement of tissue nourishment. However, current evidence is largely derived from preclinical studies and limited clinical data; therefore, well-designed randomized controlled trials are required to establish their efficacy in female populations.
Some commonly described Vrishya Dravya are summarized in Table 4.
Vrishya Dravya and Their Properties.
Local Procedures for Painful Conditions
For conditions such as vaginismus and dyspareunia, Ayurveda describes localized therapeutic approaches aimed at reducing pain, improving tissue flexibility, and promoting relaxation. These interventions are traditionally used as supportive measures and should be applied with appropriate clinical discretion.
Sthanika abhyanga (local oil massage): Gentle massage of the pelvic region, lower abdomen, and inner thighs using medicated oils such as mahanarayana taila, bala taila, or shatavari taila. This approach may help reduce muscular tension, improve local circulation, and promote relaxation.
Dhoopana (medicated fumigation): Application of herbal fumes using substances such as guggulu (Commiphora Mukul L.), devadaru (Cedrus deodara), and agaru (Aquilaria agallocha L.).
Yoni pichu (intravaginal oil application): Placement of sterile gauze soaked in medicated oil within the vaginal canal for a specified duration. This procedure is described to support lubrication and local tissue health. However, it should be performed under proper aseptic conditions and clinical supervision.20,21
Conclusion
Human sexuality is a complex, multidimensional phenomenon influenced by biological, psychological, interpersonal, and sociocultural factors. FSD reflects this complexity and requires a comprehensive approach beyond symptom-based management.
The present review highlights that while conventional therapies target specific neuroendocrine and physiological mechanisms, their effectiveness may vary across individuals due to heterogeneous patient responses and associated adverse effects. In contrast, Ayurvedic principles provide a holistic approach integrating mind-body interactions, emphasizing the role of manas, sampraharshana, and apraharsha bhava in sexual function.
Therapeutic approaches such as vajikarana and sattvavajaya chikitsa focus on enhancing psychological well-being, interpersonal harmony, and physiological balance. These perspectives may complement contemporary models by addressing domains that are often underrepresented in biomedical approaches, particularly emotional and relational dimensions of sexual health.
This integrative framework may support the development of more personalized, culturally sensitive, and holistic strategies for managing female sexual health. Combining evidence-based biomedical interventions with contextually appropriate Ayurvedic principles may enhance therapeutic personalization, improve QOL, and encourage further interdisciplinary clinical research.
Footnotes
Acknowledgements
We want to express our heartfelt gratitude to them for their unwavering support and resources throughout this journey. Their guidance and encouragement have been invaluable in the successful completion of our work.
Authors’ Contribution
Dr Vaishnavi G Kulkarni: Conceptualization, visualizations, writing, editing, validation, and methodology. Dr Kashavva V Hiremath: Writing, reviewing, and editing. Dr Aashish Patel: Conceptualization, visualizations, writing,
Data Availability Statement
Not applicable.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and publication of the article.
Ethical Approval
Ethical permission was not applicable to this article, as this is a review article drafted from various research articles and not from patients directly.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Not applicable.