
Abstract
Aim: To assess the prevalence and typology of sexual dysfunction in female patients receiving antidepressant medications using the Arizona Sexual Experience Scale (ASEX).
Method: A cross-sectional design was employed. A total of 71 married women with various psychiatric disorders receiving antidepressants for at least 3 months’ were evaluated on ASEX, Brief Adherence Rating Scale, Medication Adherence Questionnaire, and Global Assessment of Functioning (GAF) scale. Subjects with a history of sexual dysfunction prior to psychotropic intake, menopause, severe interpersonal relationship problems with spouse, or chronic medical illness were excluded.
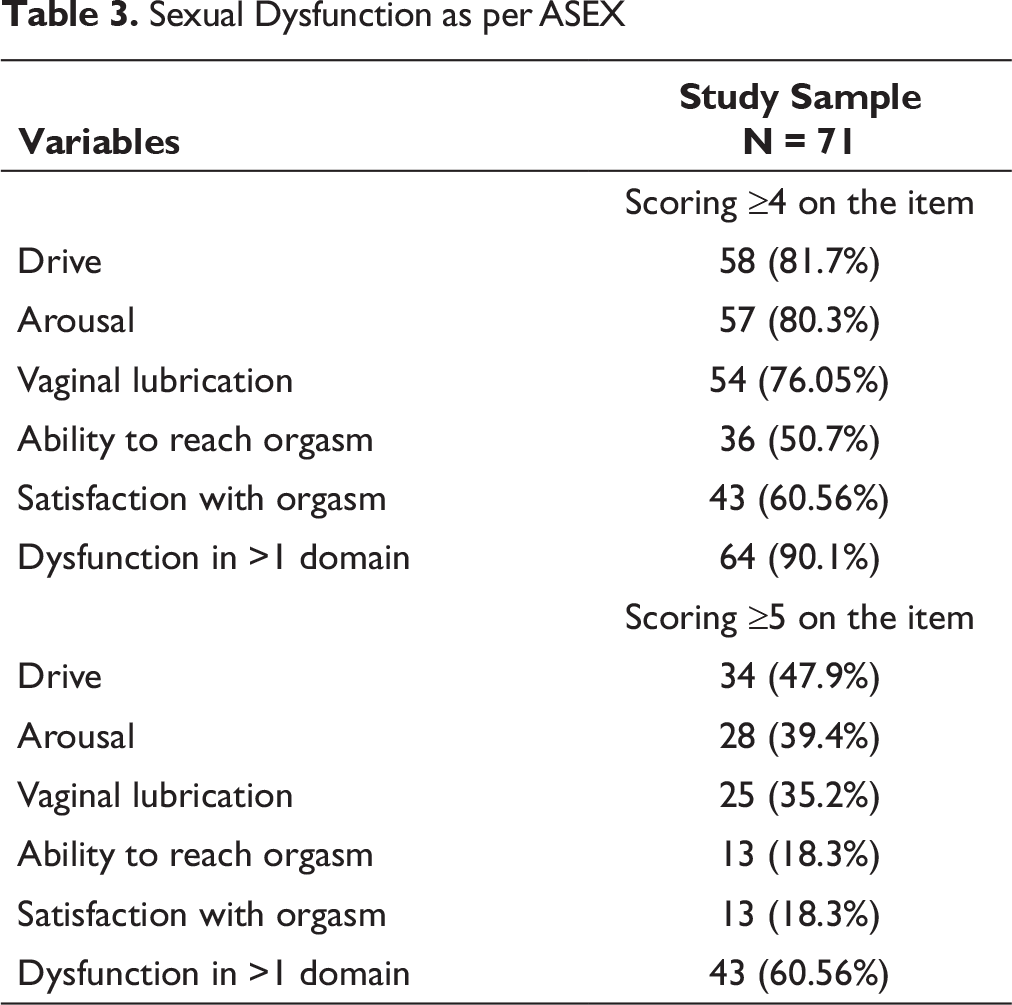
Results: The study sample had the mean age of 37.35 (SD: 6.82) years. More than four-fifth (80.2%) of patients had sexual dysfunction as per the ASEX. Using a cutoff score of 4 or more to define sexual dysfunction in various domains, decreased desire was seen in 81.7%, reduced arousal was seen in 80.3%, poor vaginal lubrication was seen in 76.1%, reduced satisfaction was seen in 57.7%, and reduced ability to reach orgasm was seen in 50.7%. Despite this, few patients (13.3%) discussed their sexual dysfunction with their treating psychiatrist. Sexual dysfunction did not influence the medication adherence.
Conclusions: Sexual dysfunction is quite prevalent in female patients receiving antidepressant medications; however, this is not adequately discussed by the patient or the treating psychiatrist.
Introduction
Sexual dysfunction with antidepressant medications is a well-known side effect. 1 Almost all the antidepressants have been implicated to cause sexual dysfunction, although incidences differ between the different antidepressants. 2 Antidepressant-induced sexual dysfunction is known to be associated with significant distress, 2 poor medication compliance, and treatment discontinuation.2, 3 However, more literature is available on antidepressant-induced sexual dysfunction in males compared to females. 4 The prevalence of antidepressant-induced sexual dysfunction among females has varied across different studies and different antidepressants with the prevalence range of 2% to 82%. 5 In general, studies suggest that prevalence of sexual dysfunction with antidepressants with serotonergic mechanism is higher compared to that with antidepressants primarily acting on noradrenergic, dopaminergic, or non-monoaminergic neurotransmitters.6, 7 Data from different metanalysis suggest that antidepressant-induced sexual dysfunction among females is about 40%, compared to 14% among those receiving placebo.6-8
In terms of various domains of sexual functioning, higher prevalence of dysfunction is reported for the domains of sexual desire (72%) and sexual arousal (83%). Compared to these domains, dysfunction in other domains is less commonly reported.6-9
Compared to the data from other countries, there are limited number of studies from India which have evaluated antidepressant-emergent sexual dysfunction in females.10-13 All these studies have relied the upon Female Sexual Function Index (FSFI)10-13 with some of studies additionally using Arizona Sexual Experience Scale (ASEX). The sample size in these studies for patients receiving antidepressants has varied between 30 and 135 and the prevalence of sexual dysfunction varied from 40% to 70.3%, when the total FSFI scores are considered and prevalence as per the ASEX has been 46.66% to 73.3%.11, 13 Further, the studies which have used a comparison group suggest that the prevalence is significantly higher among patients receiving antidepressants compared to the healthy controls. However, when the prevalence of sexual dysfunction is evaluated as per the various subscales of FSFI, the prevalence of dysfunction in the domain of sexual desire has been reported to be as high as 90%, that for decreased arousal has been reported to be 86%, decreased orgasm to be 68%, decreased satisfaction to be 62%, decreased lubrication to be 54%, and pain during sexual activity to be 32%. 12 However, previous studies from India have not evaluated the association of antidepressant-emergent sexual dysfunction with medication compliance and the reaction of the partner to the sexual dysfunction. Accordingly, there is a need to expand the literature. This study aimed to assess the prevalence and typology of sexual dysfunction in married female patients receiving antidepressants for at least 3 months and currently in clinical remission, using the ASEX.
Methodology
This study was carried out at the psychiatry outpatient facility of a tertiary care hospital. The study was approved by the ethics committee of the institute and the study participants were recruited after obtaining written informed consent. The inclusion criteria for the study included age between 19 and 55 years, married, and currently in a stable relationship with a partner of opposite gender, receiving antidepressant medications for at least a period of 3 months, free from any comorbid chronic physical illness which can impair sexual functioning, currently not pregnant, not taking any other medications which can alter the sexual functioning, and currently asymptomatic or having mild symptoms. This was determined by the treating clinician, based on the clinical judgment. Similarly, lack of comorbid physical illness was determined by the information as given by the patient and their caregivers and review of records of previous treatment. The psychiatric diagnosis was based on the International Classification of Diseases, Tenth Revision (ICD-10) criteria. Subjects with a history of sexual dysfunction prior to psychotropic intake, menopause, and those experiencing severe interpersonal relationship problems with spouse were excluded.
The study participants were recruited using a convenient sampling technique. ASEX
14
was used to assess the current level of sexual functioning. The participants were also assessed for any kind of sexual dysfunction (involving libido, delayed orgasm, orgasm, vaginal lubrication) by using a semistructured interview by a psychiatrist with the patient and their partner, and these dysfunctions were recorded as “present” or “absent.” Brief Adherence Rating Scale (BARS)
15
and Medication Adherence Questionnaire were used to evaluate the medication adherence of the patients in the previous month.
ASEX is a brief 5-items, self-report scale, which is one of the most commonly used instruments to assess the sexual dysfunction associated with use of various psychotropic medications. It covers 5 domains of sexual functioning, that is, drive, arousal, vaginal lubrication, ability to reach orgasm, and satisfaction from orgasm. The patient is asked to rate their sexual functioning in last 1 month on a 6-point scale. A higher score on any of the item suggests higher level of sexual dysfunction. A total score ≥19 or a score of ≥5 on any one item or a score of ≥4 on any 3 items of ASEX is considered to be indicator of clinical sexual dysfunction. In some of the studies, score of ≥4 or ≥5 on each item has also been used to quantify sexual domain in various domains. The scale has good psychometric properties in the form of high internal consistency (alpha value: 0.9) and excellent test-retest reliability (0.8-0.89). For the current study, the Hindi translated version was used. BARS
15
is a brief scale, which is completed by a clinician to quantify medication adherence in the last 1 month. Medication adherence is quantified on the basis of number of days and the amount of medication missed and also in the form of percentage of medications consumed in the previous 1 month by using a visual analogue scale. Medication Adherence Questionnaire is a 4-items “yes/no” questionnaire to assess the ways in which the person fails to take their medications. The non-adhernece is indicated by lower scores and higher scores suggest better medication adherence. The scale has adequate psychometric properties in the form of reliability and validity and it has been widely used to evaluate medication adherence. A semistructured interview was administered by a trained psychiatrist to evaluate for presence of any sexual dysfunction, spontaneous reporting on sexual dysfunction when enquired about any side effects experienced with use of ongoing antidepressants and did the patient discuss about the sexual dysfunction with their treating psychiatrist. As part of the interview, distress associated with sexual dysfunction and reaction of the partner was also noted. Additionally, menstrual problems associated with use of antidepressants were also noted.
Data was analyzed by using Statistical Package for Social Sciences, 20th version (SPSS-20). Descriptive analysis was done by computing mean and standard deviation with range for continuous variables. Categorical variables are represented as frequency and percentages. T-test or the Mann–Whitney U test was used to compare the continuous variables of with and without sexual dysfunction. Categorical variables were compared by using Chi-square test and Fisher’s exact test.
Results
The study included 71 females, with a mean age of 37.35 (SD: 6.82) years. The mean duration of education of the study sample was 10.57 (SD: 4.75) years. Those from nuclear families and urban locality outnumbered those from joint/extended families and rural locality, respectively.
As per the ASEX cutoff, 57 (80.3%) of the participants had sexual dysfunction. When those with and without sexual dysfunction, as per ASEX were compared, it was seen that those with sexual dysfunction were less educated and more often belonged to joint/extended families and rural locality (Table 1). Both the groups did not have any significant difference with respect to age (Table 1).
Sociodemographic and Clinical Profile of Study Sample
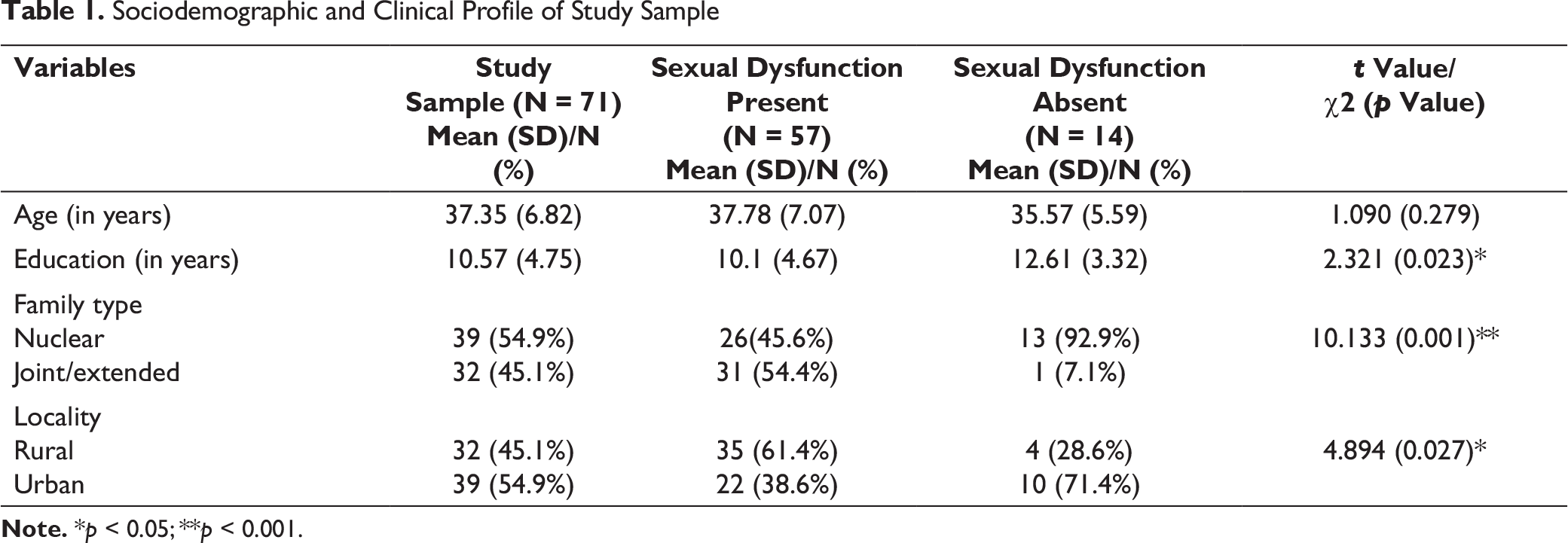
Note. *p < 0.05; **p < 0.001.
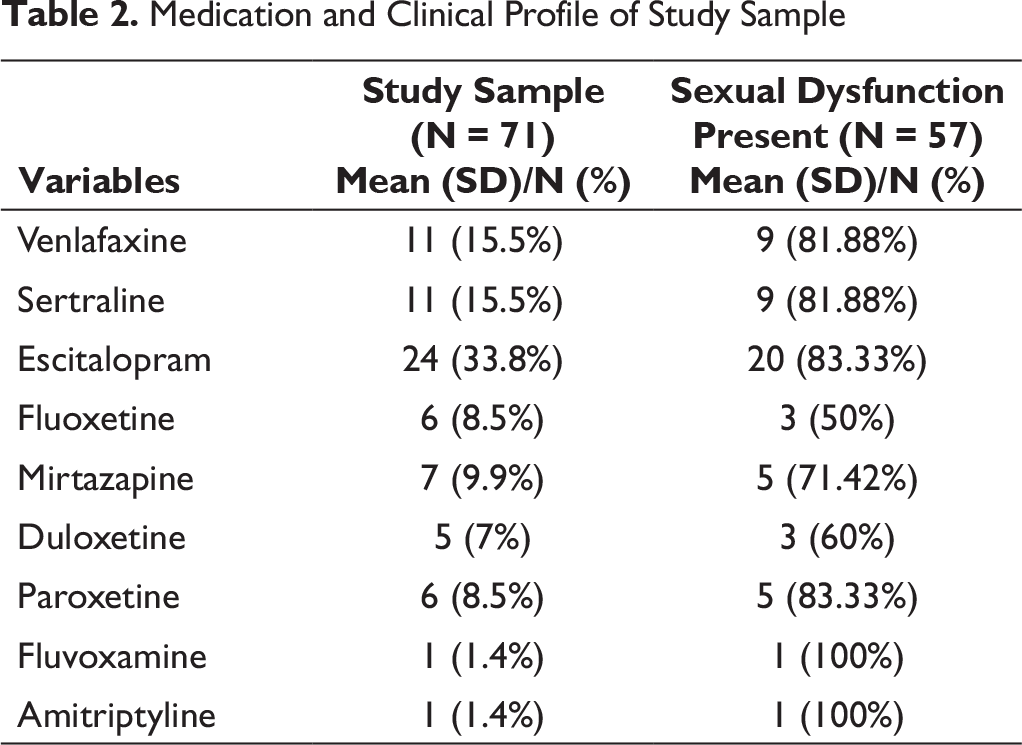
In terms of antidepressant medications, escitalopram was the most commonly prescribed antidepressant medication and this was followed by venlafaxine and sertraline (Table 2). When the prevalence of sexual dysfunction was evaluated for each antidepressant, highest prevalence was noted for fluvoxamine (100%) and amitriptyline (100%), followed by escitalopram (83.33%) and paroxetine (83.33%), and this was followed by venlafaxine (81.88%) and sertraline (81.88%). Least prevalence was noted among those receiving fluoxetine (50%) (Table 2).
The mean GAF score for the whole study sample was 68.45 (SD: 9.22), with no significant difference between the 2 groups (Table 2).
Medication and Clinical Profile of Study Sample
Sexual Dysfunction as per ASEX
When the participants were evaluated for sexual dysfunction as assessed on semi-structured interview, very few participants reported about their sexual dysfunction on their own and had discussed the sexual dysfunction with their treating psychiatrist. There was lack of any significant difference between those with and without sexual dysfunction in terms of self-report of sexual dysfunction and discussing the sexual dysfunction with the treating psychiatrist (Table 3). In terms of specific dysfunction, 59.1% reported decreased libido and 18.3% reported delayed orgasm (Table 4). When those with and without sexual dysfunction as per ASEX were compared, significantly higher proportion of those with sexual dysfunction as per ASEX reported decreased libido and significantly higher proportion of those without sexual dysfunction reported increased libido (Table 4). About one-fourth (28.2%) were distressed about their sexual dysfunction and half (50.7%) reported that their partner react adversely to their sexual dysfunction. However, those with presence or absence of sexual dysfunction as per ASEX did not differ from each other in terms of these variables.
In terms of reproductive side effects and weight-related issues, 32.4% reported weight gain, 25.35% reported menorrhea, and 11.3% reported amenorrhea, after starting of antidepressants. However, those with and without sexual dysfunction as per ASEX, did not differ significantly on these variables. None of the patients denied missing the antidepressants because of sexual dysfunction (Table 4).
Sexual Dysfunction as per the Semi-structured Interview, Menstrual Issues Related to Antidepressants and Medication Adherence
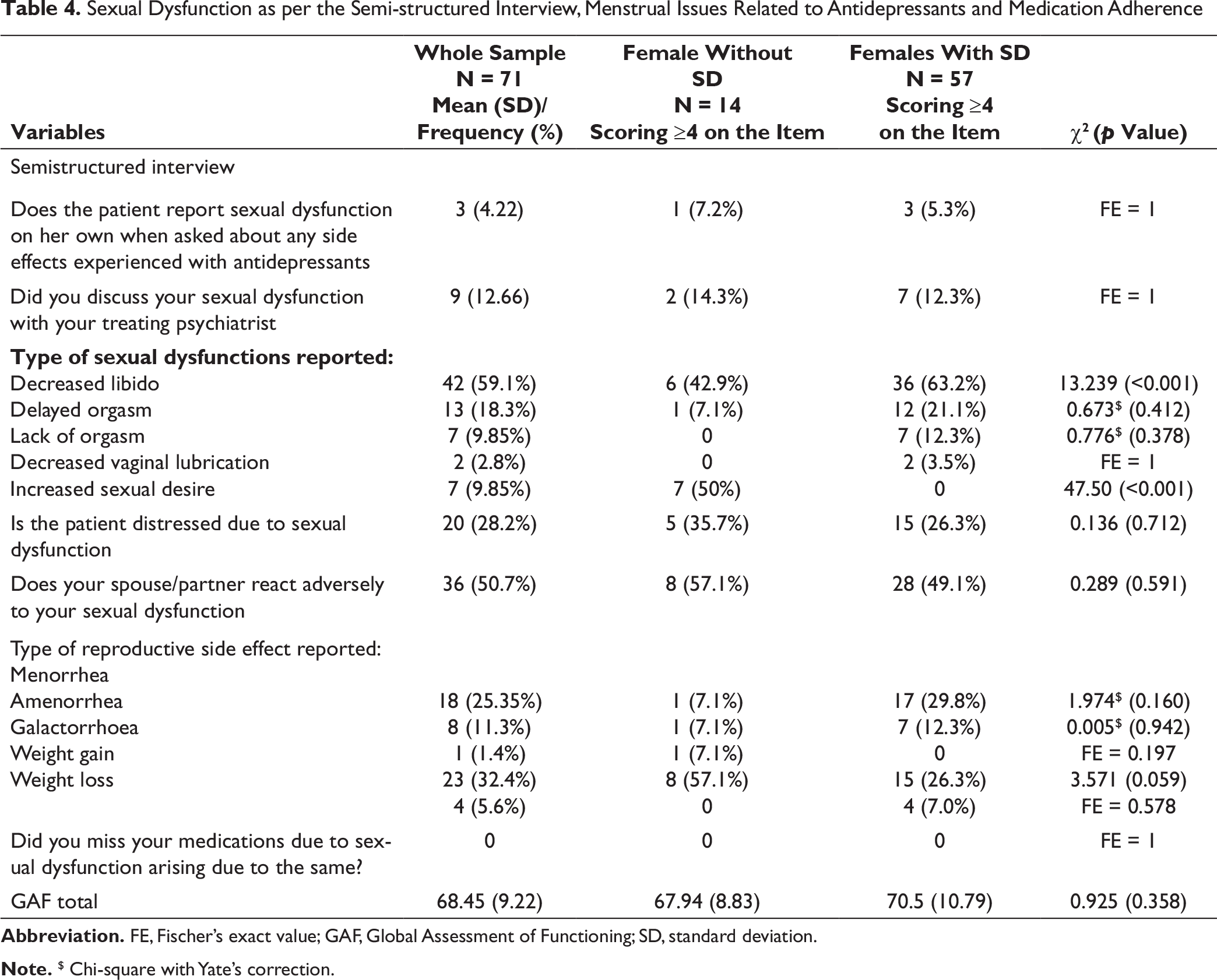
Note. $ Chi-square with Yate’s correction.
Abbreviation. FE, Fischer’s exact value; GAF, Global Assessment of Functioning; SD, standard deviation.
Comparison of Medication Compliance of Subjects With and Without Sexual Dysfunction as per ASEX
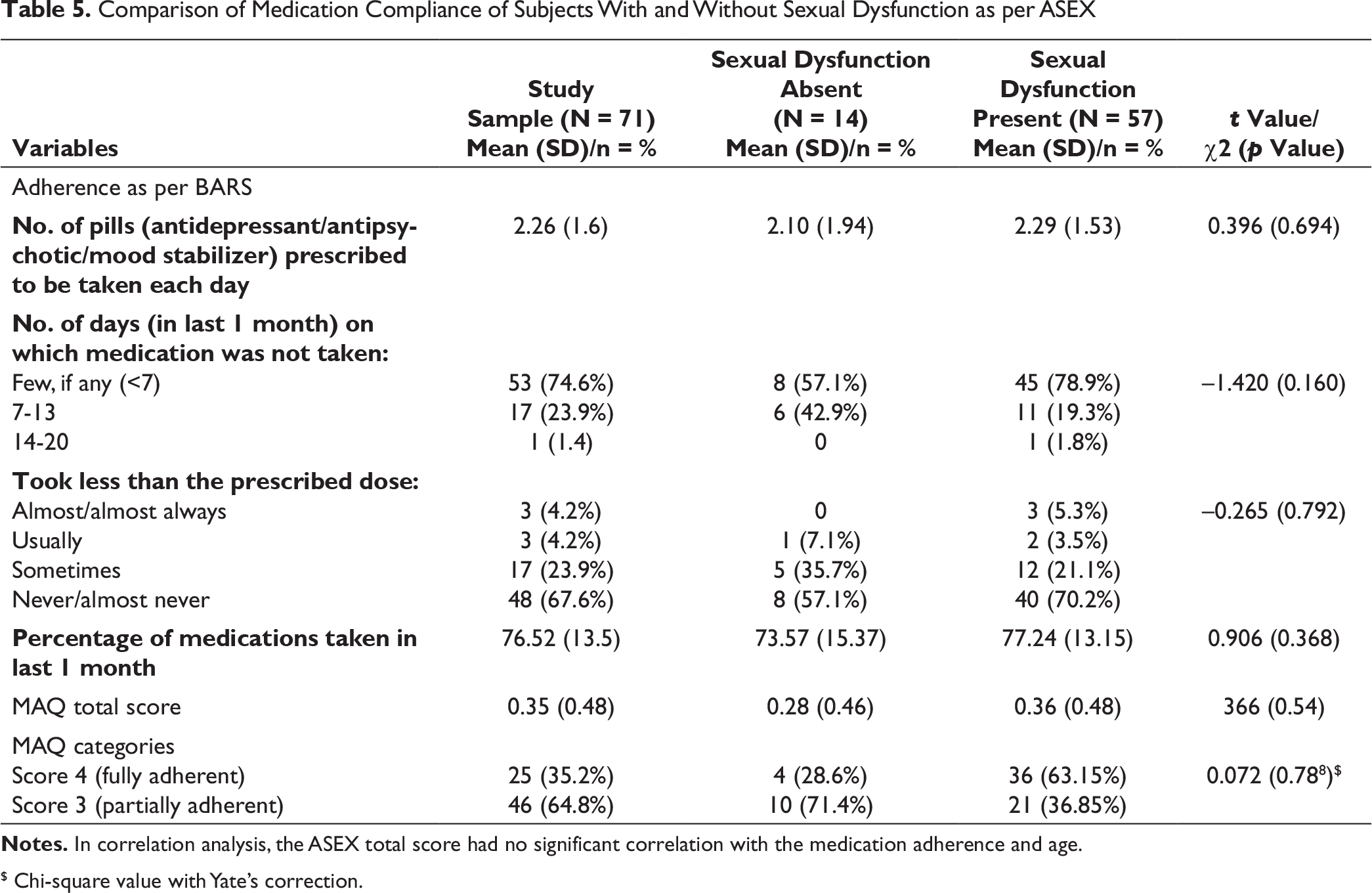
Notes. In correlation analysis, the ASEX total score had no significant correlation with the medication adherence and age.
$ Chi-square value with Yate’s correction.
Discussion
This study suggests that about four-fifths of the female patients receiving antidepressants, for about 3 months or more, who did not have sexual dysfunction prior to starting of antidepressants, even after achieving clinical stability have sexual dysfunction. Studies from different parts of the globe have reported the prevalence rate of sexual dysfunction among females receiving antidepressants to vary from 2% to 82%, 5 depending on the assessment method and time of assessment. Studies from India have reported prevalence of 40% to 70.3% when the total FSFI scores are considered, and 46.66% to 73.3% when the sexual dysfunction is assessed using ASEX.11, 13 When we compare our findings with these studies, the prevalence as seen in our study is close to the upper end of the reported range.
Previous studies have evaluated the prevalence of sexual dysfunction in various domains and these suggest that the prevalence is significantly high for the domains of sexual desire and arousal.6-9
In terms of various domains of sexual functioning, higher prevalence of dysfunction is reported for the domains of sexual desire (72%) and sexual arousal (83%). Compared to these domains, dysfunction in other domains is less commonly reported.6-9 Previous studies from India, which have evaluated the prevalence of sexual dysfunction by using FSFI have reported decreased desire in 90% of the participants, followed by the dysfunction in the arousal (86%), decreased orgasm (68%), decreased satisfaction (62%), decreased lubrication (54%), and pain during the sexual activity (32%). 12 In the present study, we used both the cutoffs of ≥4 and ≥5 to evaluate the prevalence of sexual dysfunction in various domains, and the highest prevalence was found in the domain of sexual desire or drive (47.9-81.7%), followed by dysfunction in the domains of arousal (39.4-80.3%), vaginal lubrication (35.2-76.05%), satisfaction (18.3-60.56%), and difficulty in the ability to reach orgasm (18.3-50.7%). When the dysfunction was evaluated in terms of the number of domains involved, it was seen that in 60.56% to 90.1%, participants had dysfunction in more than one domain. These findings are comparable to the existing literature.10, 16, 13 These findings suggest that the prevalence of sexual dysfunction in various domains and overall prevalence is influenced by the assessment scales and the cutoff used to define sexual dysfunction. In this study, sexual dysfunction was also evaluated by using, a semistructured interview. According to this, the prevalence of decreased libido was 59.1% and that of delayed orgasm was 18.3%. Prevalence of orgasmic dysfunction was 9.85% and decreased vaginal lubrication was reported by only 2.8%. These findings suggest significant difference between the prevalence of sexual dysfunction as reported on ASEX and as evaluated by using semi-structured interview. Additionally, about one-tenth of the participants reported increased sexual desire while evaluated using a semistructured interview. This domain of the sexual dysfunction is not tapped by using ASEX. The presence of increased sexual desire could be an indicator of the presence of antidepressant-induced side effect—a feeling of general well-being with the antidepressants or antidepressant-induced switch. However, clinical evaluation did not support the latter.
However, an important finding of this study was that only one-eighth (12.66%) of the participants discussed about their sexual side effects with their treating psychiatrist and when asked about any side effects experienced with antidepressants, only 4.22% participants spontaneously reported the same. Hence, it is important for the treating clinicians to take a lead to assess these side effects. Additionally, this study shows that about one-fourth (28.2%) of the females are themselves distressed because of their dysfunction and about half of them reported that their partners reacted adversely to their changed sexual participation in the last 1 month. These findings suggest that sexual dysfunction among females receiving antidepressants not only leads to the distress among the patients, but also leads to distress among their partners. Taken together, these findings suggest that female patients while receiving antidepressants usually do not report sexual dysfunction spontaneously, also they do not report about these side effects to the treating clinicians, are distressed because of the same, and also possibly face adverse reaction of their partners because of sexual dysfunction.
In this study, the participants took 76.52% of the prescribed medications in the previous 1 month. These findings support the existing literature which suggests high rates of medication non-adherence in patients receiving antidepressant.17, 18 However, in this study, unlike expected, sexual dysfunction did not have any adverse impact on the medication adherence. These findings are contrary to the existing literature, which suggest association of sexual dysfunction with poor medication adherence.17, 18 This possibly suggests a cultural variation in terms of the social role of females in the Indian society, in that, they follow the advice to take medications, even at the cost of suffering.19, 20
This study has multiple limitations, which must be kept in mind, while interpreting the findings of the study. The study sample was small, assessment was cross-sectional and we did not evaluate the interpersonal dimension in detail. We did not evaluate the residual psychopathology in the study sample. Association of sexual dysfunction with dose of antidepressants was not evaluated due to use of variable doses in different patients. There were very few patients or actually 1 patient on specific antidepressant; hence, the finding of the prevalence of sexual dysfunction, as noted in this study, for that antidepressant cannot be generalized. Future studies must attempt to overcome these limitations.
To conclude, this study suggests that about four-fifths of the female patients on antidepressants experience sexual dysfunction. In terms of specific domain of sexual function, higher proportion of patients report decreased desire and this is followed by reduced arousal, poor vaginal lubrication, reduced satisfaction, and reduced ability to reach orgasm. Despite this, few females discussed about their sexual dysfunction with their treating psychiatrist. Sexual dysfunction among females does not influence the medication adherence. About one-fourth of the females are themselves distressed due to sexual dysfunction and about half report that their partners react adversely to their changed sexual participation.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.