
Abstract
Chemsex, defined as the intentional use of psychoactive substances (PS) to facilitate or enhance sexual activity, has emerged as an important public health and psychosexual medicine concern. It has been associated with increased sexual risk-taking, substance dependence, psychiatric morbidity, and impaired psychosocial functioning.
Objective:
This review aims to examine chemsex through an integrative framework by synthesizing current evidence from neurobiology, psychosexual medicine, and Ayurvedic perspectives.
Methods:
A literature review was conducted using PubMed, Scopus, Web of Science, and Google Scholar. Relevant literature on chemsex, reward neurobiology, sexualized drug use, addiction mechanisms, and Ayurvedic concepts related to mental regulation and vitality was reviewed.
Results:
From a neurobiological perspective, commonly used chemsex substances such as methamphetamine, mephedrone, and gamma-hydroxybutyrate (GHB) act primarily through dopaminergic and reward-related pathways, producing heightened pleasure, disinhibition, and reinforcement. Repeated exposure may contribute to neuroadaptation, compulsive use, impaired executive control, and reduced natural reward sensitivity. From an Ayurvedic perspective, chemsex may be interpreted as dysregulation of mental qualities, impaired judgment, and depletion of restorative vitality constructs such as ojas and shukra dhatu. These interpretations are conceptual and should not be considered claims of direct biological equivalence.
Conclusion:
Chemsex is a multidimensional phenomenon involving neurobiological, psychological, behavioral, and social determinants. Integrative approaches combining harm reduction, addiction treatment, psychosexual care, and supportive holistic interventions may offer broader management pathways. Further empirical research is needed to validate interdisciplinary models.
Introduction
Human sexual behavior is a multidimensional phenomenon shaped by complex interactions among neurobiological, psychological, interpersonal, and sociocultural factors. Sexual desire and arousal are regulated through interconnected dopaminergic, serotonergic, and oxytocinergic pathways that influence reward processing, motivation, emotional attachment, and pleasure perception. 1 Psychological factors such as personality traits, emotional regulation, self-esteem, and mental health status further modulate sexual functioning and behavior. 2 In addition, sociocultural influences, including stigma, relationship norms, and technology, play an important role in shaping sexual expression across populations. 3
The relationship between sexuality and psychoactive substance use has been recognized throughout history. 4 Substances have been used in various cultures and social settings to reduce inhibition, enhance intimacy, intensify sensory experiences, and facilitate interpersonal connection. In recent years, a specific phenomenon known as “chemsex” has gained increasing attention in psychosexual medicine. The term chemsex is derived from the words “chemicals” and “sex” and refers to the intentional use of certain psychoactive substances (PS) in the context of sexual activity. Commonly involved substances include methamphetamine, mephedrone, gamma-hydroxybutyrate (GHB), and gamma-butyrolactone (GBL), used before or during sexual encounters.5–7 These agents are often used to reduce psychological inhibitions, enhance sexual desire and pleasure, prolong sexual sessions, and intensify the overall sexual experience. 8 The phenomenon was initially reported primarily in certain urban populations but is now recognized globally. The practice has been most frequently reported among men who have sex with men (MSM). 9 Although chemsex has been predominantly studied among MSM populations, it may also occur in heterosexual, bisexual, and other groups in private or social network settings, where high-risk behaviors, such as unprotected intercourse, prolonged or rough sexual activity, and sharing injection equipment are common, with frequency ranging from multiple times per week to a few times per year. 10 It is more commonly reported among groups using dating apps and is most frequently connected to group sex practices. 11 Chemsex prevalence in the MSM community is reported between 3% and 32%. 12 Few studies have examined chemsex in the general population; one survey of 22,289 participants found that 20% of respondents had used drugs to enhance their sexual experiences. 13
From a neurobiological perspective, many chemsexassociated substances exert their effects through stimulation of the mesolimbic reward system, particularly by increasing dopamine availability in brain regions associated with motivation and pleasure. Repeated pharmacological activation of these pathways may lead to neuroadaptation changes, including dopamine receptor downregulation and altered reward sensitivity, which can subsequently impair natural sexual responsiveness.14–15
Ayurveda Framework for Sexual Health and Substance Use
Ayurveda, the traditional medical system of India, offers a distinct conceptual framework for understanding sexual behavior, substance use, and their interaction. Unlike the reductionist neurobiological model, Ayurveda adopts a holistic, psychosomatic approach in which sexual health is embedded within broader physiological, psychological, and spiritual domains. Central to this framework is shukra dhatu, the reproductive tissue and refined bodily tissue, which sustains fertility, vitality, and sexual vigor. When shukra dhatu is preserved, it supports healthy sexual function and overall well-being; disturbance of shukra dhatu may be conceptually related to impaired sexual well-being or reduced satisfaction. 16
Closely related to shukra dhatu is ojas, the subtle essence of all bodily tissues, responsible for immunity, mental clarity, and psychological resilience. In the Ayurvedic view, ojas is traditionally considered vulnerable to depletion by excessive, artificial, or unbalanced sensory stimulation, including substance-facilitated sexual activity. Decrease in ojas has been conceptually associated with diminished resilience and vulnerability to distress. 17 Thus, from an Ayurvedic perspective, chemsex is not only a behavioral issue but represents a state of ojas depletion.
The mental qualities, or manasika gunas, sattva, rajas, and tamas, further govern sexual behavior. Rajas is the quality of activity, impulsivity, and desire; when aggravated, it may be associated with compulsive seeking, hyperarousal, and inability to stop rewarding behaviors. Tamas is the quality of inertia, confusion, and emotional numbness; when increased, it impairs judgment, reduces self-control, and fosters denial of harm. Sattva, conversely, is the quality of clarity, balance, and self-regulation, which promotes healthy sexual expression and resistance to addiction. In chemsex, rajas and tamas become dominant, while sattva is suppressed. 17
Another key construct is prajnaparadha, often translated as “intellectual error” or “crime against wisdom.” This refers to knowingly engaging in harmful behavior despite understanding its negative consequences. In the context of chemsex, prajnaparadha may help explain why individuals may continue substance-facilitated sexual activity even when facing deteriorating physical health, psychiatric symptoms, and social consequences. 18 This concept parallels the modern understanding of impaired executive function and loss of insight in addiction disorders.
Classical Ayurvedic texts, including the Charak Samhita and Sushruta Samhita, explicitly warn against these substances, referred to as madya and vishadravya. These substances are described as artificially overstimulating the mind and body, disturbing the equilibrium of doshas, corrupting shukra dhatu, and severing the natural link between sexual activity and its intended purposes of vitality, reproduction, and emotional satisfaction.16,19–27 Rather than supporting regulated expression of kama (natural sexual desire), these substances may lay the groundwork for compulsive behavior and long-term psychophysiological depletion.
In summary, from an Ayurvedic interpretive perspective, chemsex may represent a broader state of dysregulation involving behavioral excess, impaired balance, and progressive depletion (shukra dhatu kshaya), loss of vital essence (ojas), aggravation of rajas and tamas mental qualities, and intellectual error (prajnaparadha). Unlike modern biomedical models that focus primarily on neurotransmitter systems, Ayurveda emphasizes the restoration of ojas. Rebalancing of mental qualities toward sattva and rebuilding of shukra dhatu may be considered therapeutic targets. 17
This review critically examines chemsex through an interdisciplinary framework integrating neurobiology, psychosexual medicine, and Ayurvedic theory. It summarizes current evidence regarding behavior patterns and associated risks, reviews relevant neurobiological mechanisms, explores potential Ayurvedic interpretive models, and discusses implications for prevention, harm reduction, and future research.
Methodology
This study was conducted as a comprehensive literature review to synthesize current knowledge regarding chemsex from multidisciplinary perspectives, including psychosexual medicine, addiction science, neurobiology, public health, and Ayurveda. A comprehensive review design was selected because the topic spans clinical, behavioral, sociocultural, neurobiological, and traditional conceptual domains that cannot be adequately addressed through a single, narrowly focused clinical question.
Search Strategy
A structured literature search was conducted in March 2026 using the following electronic databases:
PubMed, Scopus, Web of Science, Google Scholar.
To improve coverage, manual screening of reference lists from relevant review articles and key publications was also performed.
Search Terms
Search terms included combinations of the following keywords using Boolean operators (AND, OR) where appropriate:
“Chemsex,” “sexualized drug use,” “methamphetamine and sex,” “GHB and sexual behavior,” “MSM and chemsex,” “mephedrone,” “compulsive sexual behavior,” “substance use disorder (SUD),” “reward pathway,” “dopamine and addiction,” “psychosexual health,” “Ayurveda and addiction,” “ojas,” “shukra dhatu,” “prajnaparadha.”
Eligibility Criteria
Studies were considered eligible if they met one or more of the following criteria:
Peer-reviewed original research articles, observational studies, clinical studies, systematic reviews, or narrative reviews, reports relevant to chemsex epidemiology, psychosexual outcomes, neurobiology, addiction mechanisms, or harm reduction, scholarly sources relevant to Ayurvedic conceptual interpretation.
Exclusion Criteria Included
Duplicate records, non-English publications, editorials lacking substantive analysis, case reports without broader clinical relevance, and studies not directly related to chemsex or sexualized substance use.
Study Selection Process
A total of 294 records were initially identified through database searching and manual reference screening. After the removal of duplicate and clearly irrelevant records, titles and abstracts were screened for relevance. Potentially eligible full-text articles were then reviewed in detail. Following application of predefined inclusion and exclusion criteria, 51 sources were ultimately selected for inclusion in the final qualitative synthesis.
Methodological Limitations
The available chemsex literature remains heterogeneous in definitions, sampling methods, and geographic focus, with a substantial proportion derived from MSM populations in Western urban settings. This may limit generalizability to other groups and regions. In addition, Ayurvedic comparisons presented in this review are theoretical and interpretive in nature, intended to stimulate interdisciplinary discussion rather than imply direct empirical equivalence.
Epidemiology and Clinical Context of Chemsex
Chemsex has emerged as a growing concern in sexual health, addiction medicine, and public health, particularly in urban settings and digitally mediated sexual networks. It has been most frequently reported among MSM, although increasing evidence suggests its presence in heterosexual, bisexual, and mixed populations.9,12,13
Reported prevalence varies considerably across studies because of differences in definitions, recruitment settings, geographic location, and study methodology. Some studies define chemsex narrowly according to specific substances, whereas others include a broader range of psychoactive agents used in sexual contexts.
The clinical relevance of chemsex arises from its association with the following:
28
Repeated substance-associated sexual encounters. Prolonged sexual sessions. Multiple partners and group sexual encounters. Reduced condom use and increased sexually transmitted infection (STI) risk. Polysubstance consumption. Psychiatric morbidity. Impaired occupational or social functioning.
These associations highlight the multidimensional medical, psychological, and public health implications of chemsex.
Psychoactive Substances Commonly Associated with Chemsex
Several PS commonly associated with chemsex are summarized in Table 1. These agents are often used for their stimulant, disinhibitory, euphoric, empathogenic, or dissociative effects
Common PS Associated with Chemsex: Pharmacological Classes, Principal Mechanisms, and Reported Sexual Effects.
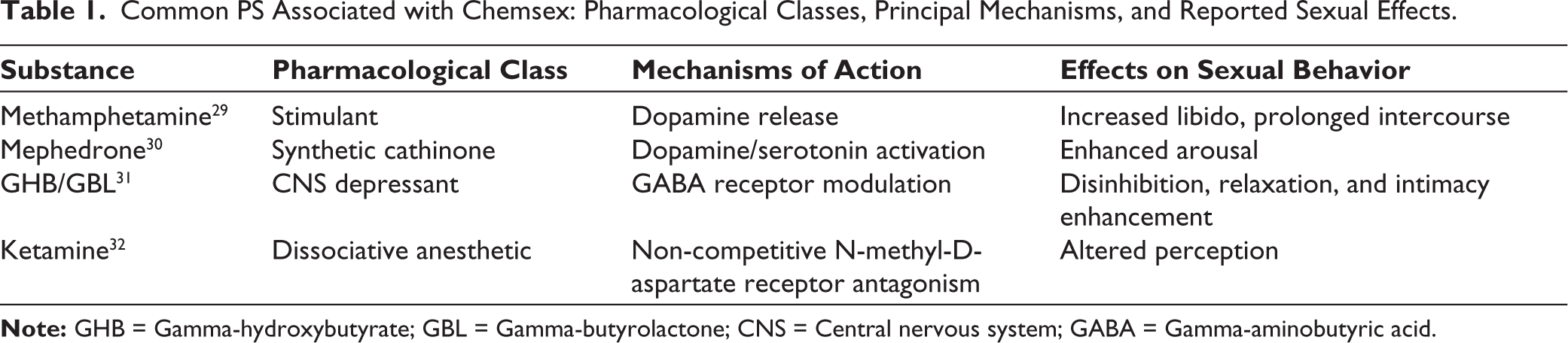
These substances may be used individually or in combination. Polysubstance use increases the risk of overdose, impaired judgment, dehydration, psychiatric complications, and medical emergencies.
Neurobiological Mechanisms Underlying Chemsex
The Natural Sexual Reward Pathway
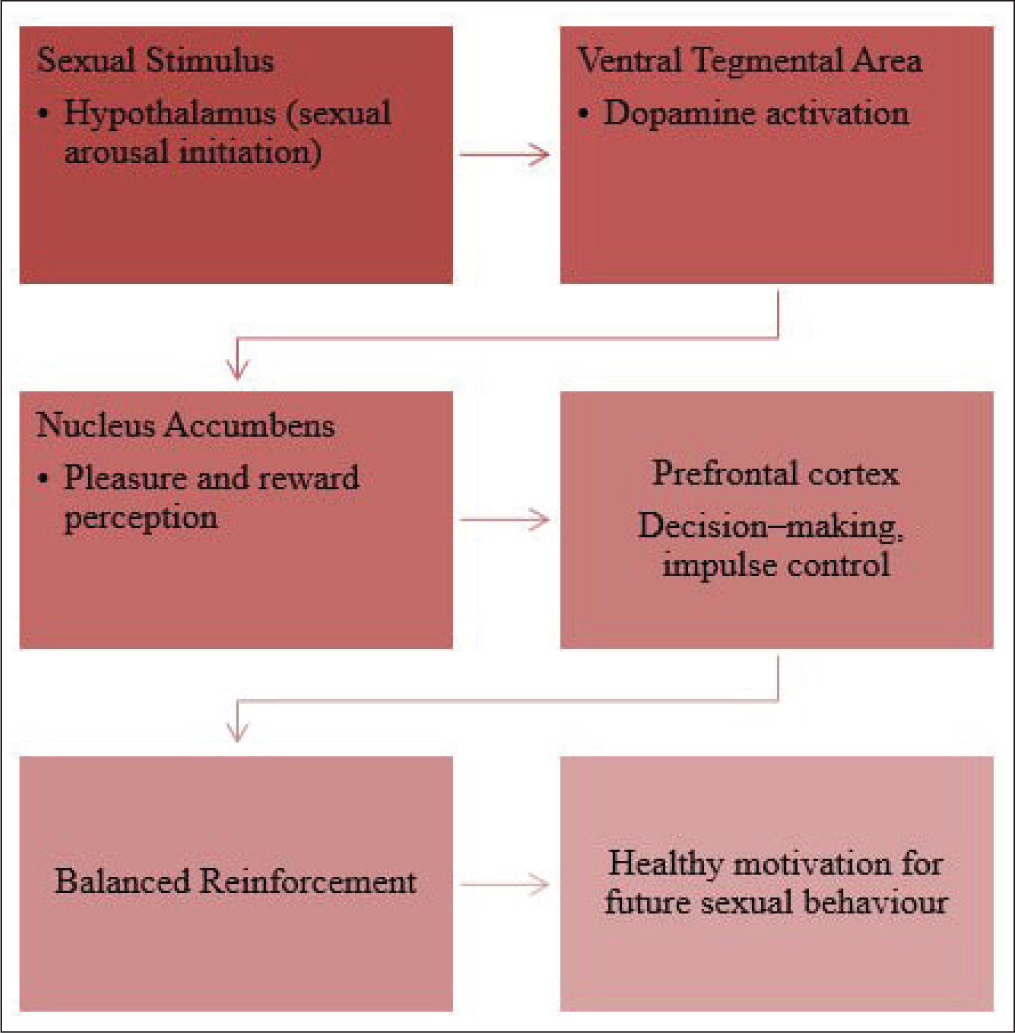
From a neurobiological perspective, sexual behavior is partly regulated by the mesolimbic reward system, particularly the dopaminergic pathway connecting the ventral tegmental area and nucleus accumbens. Under normal physiological conditions, dopamine release during sexual activity is regulated, promoting pleasure, bonding, and satisfaction without maladaptive consequences. Figure 1 illustrates the simplified natural sexual reward pathway involved in healthy sexual motivation and reinforcement. 33
Simplified Neurobiological Representation of the Natural Sexual Reward Pathway.
Chemsex-altered Reward Pathway
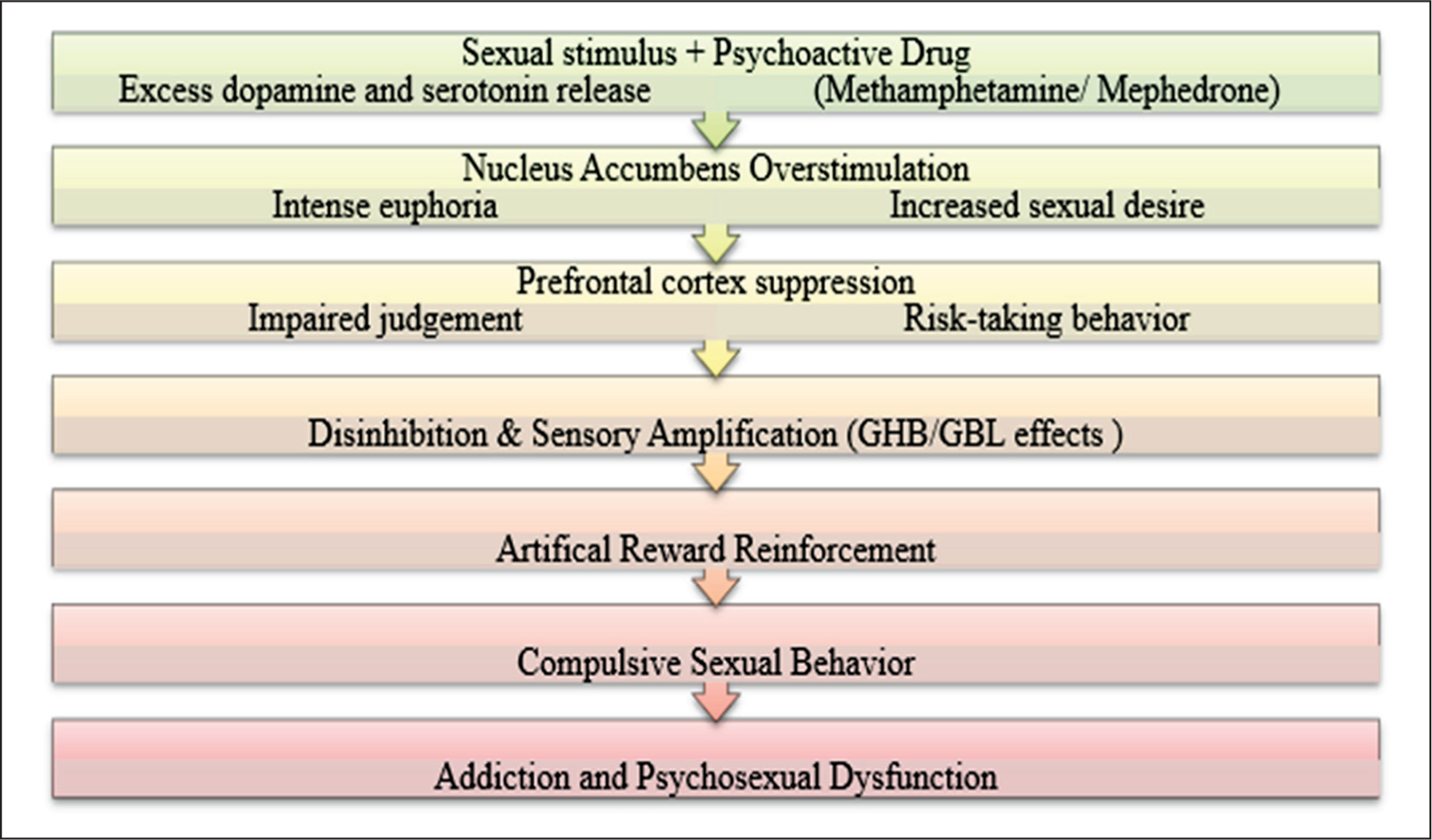
PS, commonly involved in chemsex, may enhance dopamine and serotonin release, amplifying sexual reward, emotional salience, and behavioral disinhibition. These effects may occur alongside reduced executive control mediated by the prefrontal cortex. Repeated pairing of drug intoxication with sexual activity reinforces conditioned reward circuits and contributes to compulsive sexual behaviors, substance dependence, and increased sexual risk-taking. 14 Figure 2 illustrates the proposed interaction between reward sensitization and impaired executive control in chemsex. 34
Proposed Behavioral and Neurobiological Effects of Chemsex on Reward Pathways and Executive Control.
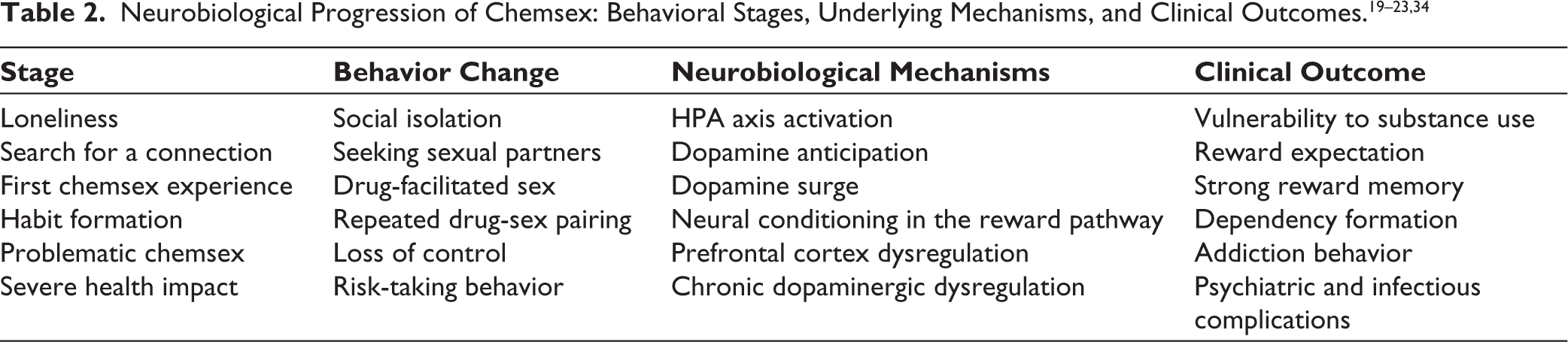
Neurobiological Progression of Chemsex
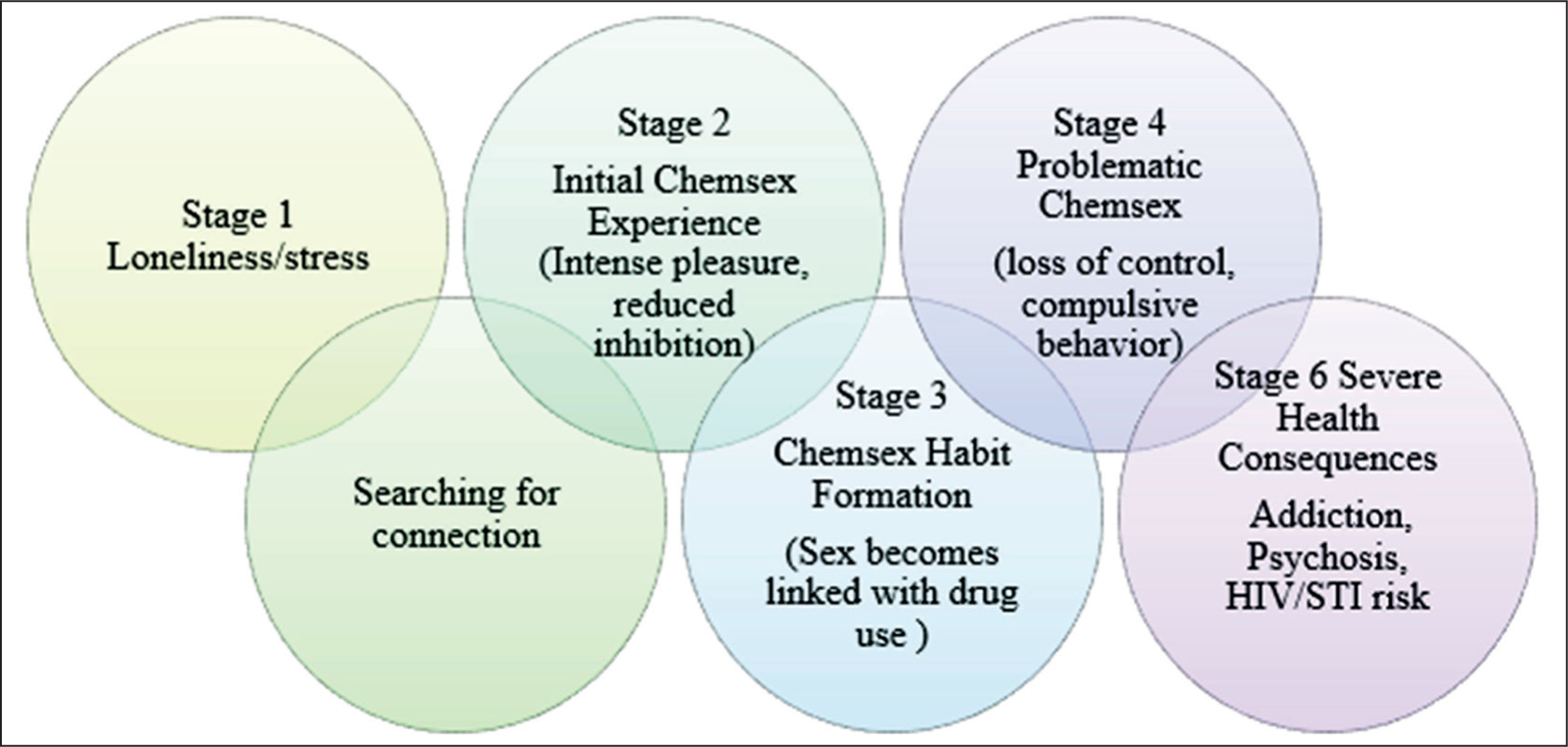
The chemsex trajectory represents a progression from psychosocial vulnerability to neurobiological dysregulation and behavioral loss of control. It often begins with loneliness and stress-induced activation of the hypothalamicpituitary-adrenal (HPA) axis, increasing susceptibility to substance use. Anticipatory dopaminergic activation during partner-seeking primes the reward system, while initial drug-facilitated sexual experiences may produce supraphysiological dopaminergic surges within the mesolimbic pathway, creating strong reward memories. Repeated pairing of drug use and sexual activity induces neuroplastic changes and conditioned reinforcement, shifting behavior from voluntary to habitual. Progressive dysfunction of the prefrontal cortex impairs impulse control and decision making, leading to compulsive sexual behavior and addiction. Chronic dysregulation of reward pathways may contribute to anhedonia, psychiatric morbidity, and high-risk sexual outcomes.19–23 The details of how problematic chemsex behavior may develop (behavioral model) are shown in Figure 3. 34
Proposed Behavioral and Neurobiological Progression from Initial Chemsex Use to Problematic Chemsex.
As summarized in Table 2, progression is likely multifactorial, involving interactions between psychosocial stressors, conditioned reward learning, and impaired executive control.
Psychological and Psychosexual Effects of Chemsex 8
Chemsex is associated not only with substance-related harms but also with significant psychological, emotional, relational, and psychosexual consequences. Although some individuals report short-term increases in confidence, intimacy, or pleasure, repeated involvement may contribute to substantial adverse outcomes.
Figure 4 summarizes common psychosexual, sexual, and relational complications associated with chemsex.
Major Psychological, Sexual, and Relational Consequences Associated with Chemsex.
Compulsive sexual behavior patterns: Repeated pairing of PS with sexual activity may reinforce conditioned reward loops and compulsive sexual behavior patterns.
Emotional dysregulation: Emotional sequelae may include loneliness, stigma, low self-esteem, anxiety, shame, and broader psychological distress.
Psychiatric comorbidities: Reported psychiatric comorbidities include anxiety disorders, depressive symptoms, and SUDs.
Repeated engagement in chemsex may also reinforce high-risk sexual behavior patterns. Drug-related disinhibition may result in reduced condom use, increased numbers of sexual partners, and elevated risk of STIs. Consequently, chemsex represents an important concern for public health, sexual medicine, and addiction services.
Ayurvedic Perspective on Substancefacilitated Sexual Behavior
Ayurveda conceptualizes sexual behavior within the domains of vajikarana (rejuvenative and reproductive health science) and manasika bhava (mental states). Vajikarana emphasizes the preservation of shukra dhatu (reproductive tissue), traditionally associated with reproductive vitality, regeneration, and aspects of well-being. 24 Within the framework, kama (natural sexual desire) is regarded as a normal human drive that, when expressed in balance, may contribute to well-being and relational satisfaction. 24
Classical Ayurvedic texts caution that intoxicating substances and toxic agents (madya and vishadravya) may disturb this equilibrium. Rather than supporting the regulated expression of kama, these substances are traditionally described as producing artificial overstimulation of the mind and body, potentially disturbing shukra dhatu and healthy behavioral regulation. This may be interpreted conceptually as predisposing to compulsive behavior patterns and long-term psychophysiological depletion.16,25
Ayurveda Perspective on Chemsex
Ayurveda conceptualizes health as a dynamic equilibrium of body, mind, behavior, and consciousness. Within this framework, excessive sensory indulgence, impaired judgment, depletion states, and disturbed mental balance are considered important contributors to suffering and disease.
Chemsex may be interpreted through selected Ayurvedic constructs as a behavioral state involving dysregulated desire, repeated overstimulation, and gradual reduction in adaptive resilience.
Prajnaparadha (impaired judgment) 26 : Prajnaparadha is traditionally described as behavior undertaken despite awareness of harmful consequences, reflecting disturbances in intellect, restraint, and memory.
In the context of chemsex, this concept may be heuristically related to:
Continued engagement despite health risks Repeated behavior despite emotional distress Impaired self-regulation Difficulty learning from negative consequences.
This should be regarded as a traditional behavioral analogy rather than a diagnostic or neurobiological label.
Rajas and tamas imbalance:
27
Ayurveda describes mental functioning through the gunas:
Sattva: Clarity, balance, awareness Rajas: Agitation, drive, restlessness Tamas: Inertia, confusion, dullness
Chemsex may be interpreted as involving alternating predominance of the following states:
Rajas: Cravings, stimulation, impulsivity, overactivity. Tamas: Intoxication, reduced awareness, fatigue, post-use lethargy.
These constructs should be understood as interpretive psychological analogies rather than measurable biomedical entities.
Ojas depletion 27 : Ojas is traditionally regarded as a refined essence associated with vitality, resilience, stability, and adaptive capacity. From an interpretive perspective, recurrent sleep deprivation, overstimulation, fatigue, poor recovery, and emotional burnout associated with chemsex may resemble states conceptually analogous to reduced ojas. Such parallels remain theoretical and require empirical validation.
Shukra dhatu disturbance 24 : It is associated with reproductive vitality, regeneration, and aspects of sexual well-being. Excessive sexual exertion, chronic depletion, and dysregulated sensual habits are traditionally viewed as disturbing this domain.
This may be conceptually related to reduced sexual satisfaction, exhaustion, diminished intimacy, or dysregulated sexual well-being. The integrative comparative framework of chemsex-related psychosexual and neurobiological features is summarized in Table 3.
Integrative Comparative Framework Between Contemporary Neurobehavioral Concepts and Ayurvedic Constructs (Theoretical Parallels, Not Equivalences).
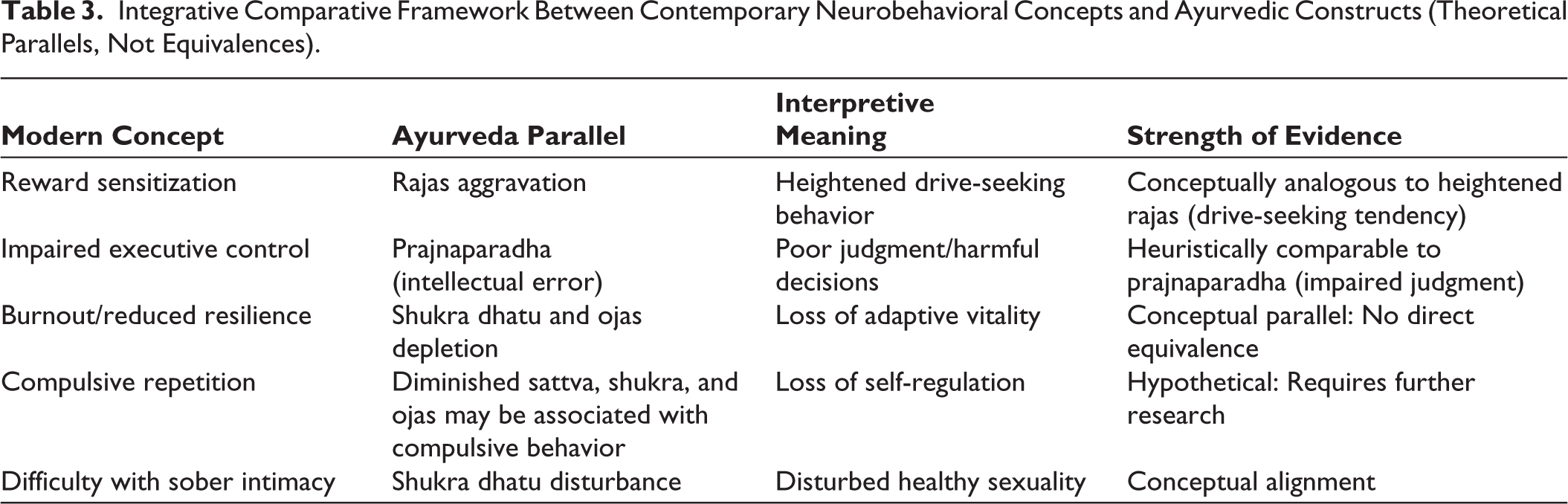
Integrative Comparative Model
Modern neuroscience and Ayurveda arise from distinct epistemological traditions; however, both recognize that repeated pursuit of intense short-term reward may lead to longer-term dysregulation and suffering.
The following comparisons are heuristic models intended to stimulate interdisciplinary dialogue rather than to imply direct biological equivalence.
Clinical Relevance of the Comparative Model
This interdisciplinary framework may help clinicians and researchers to:
Understand behavior through multiple lenses Reduce purely moralistic interpretations Improve culturally sensitive communication Integrate biomedical care with supportive lifestyle restoration strategies Generate future interdisciplinary hypotheses.
Caution in Interpretation
These parallels are conceptual in nature and should be interpreted cautiously. Ayurvedic constructs should not be interpreted as direct neurochemical mechanisms, and biomedical findings should not be retrofitted into traditional terminology without caution.
The integrative neurobiological Ayurveda model of chemsex is shown in Table 4.
Conceptual Integrative Model of Chemsex: Neurobiological Mechanisms and Ayurvedic Interpretive Correlates.

Clinical Management and Public Health Implications
Chemsex is a complex biopsychosexual and sexual health phenomenon that often requires individualized, nonjudgmental, and multidisciplinary care. Management should extend beyond substance cessation alone and address sexual health, psychological well-being, relapse vulnerability, relationship functioning, and broader social determinants.
Harm Reduction Strategies
As shown in Figure 5, effective interventions for chemsexrelated harms should be delivered in non-stigmatizing, culturally sensitive, and confidential settings. Comprehensive sexual health education may empower individuals to make informed choices while understanding associated risks. Targeted substance use treatment programs may provide pathways for reduction or cessation of problematic drug use. HIV prevention strategies, including pre-exposure prophylaxis, regular screening, and timely access to antiretroviral therapy, are important components of care. Alongside these, trauma-informed mental health counseling may help address underlying vulnerabilities such as past trauma, anxiety, depression, and shame, or minority stress that may perpetuate the cycle of chemsex. 36
Harm Reduction Framework for Chemsex: Four Core Intervention Pillars.

Integrating Modern and Ayurvedic Approaches
Chemsex-associated substances may increase dopaminergic signaling and alter reward-related processing. Repeated use may also be associated with fatigue, sleep disruption, emotional burnout, and impaired recovery. From a treatment perspective, modern therapeutic modalities offer evidence-based tools for addressing behavioral and neurobiological dimensions of chemsex, including cognitive behavioral therapy, relapse prevention models, motivational interviewing, and pharmacotherapy for withdrawal management or co-occurring psychiatric conditions.
15
When integrated cautiously with Ayurvedic principles, these approaches may be complemented by restorative lifestyle practices. Ayurveda suggests that effective management for chemsex must extend beyond behavioral modification and include:37,38
Restorative nutritional and recovery-focused approaches conceptually aimed at rebuilding vitality Sleep normalization and stress reduction strategies Structured routines (dinacharya) to improve behavioral regulation Meditation and mindfulness practices to cultivate sattva Selected rasayana or supportive herbal approaches where clinically appropriate and evidence-informed.37–39
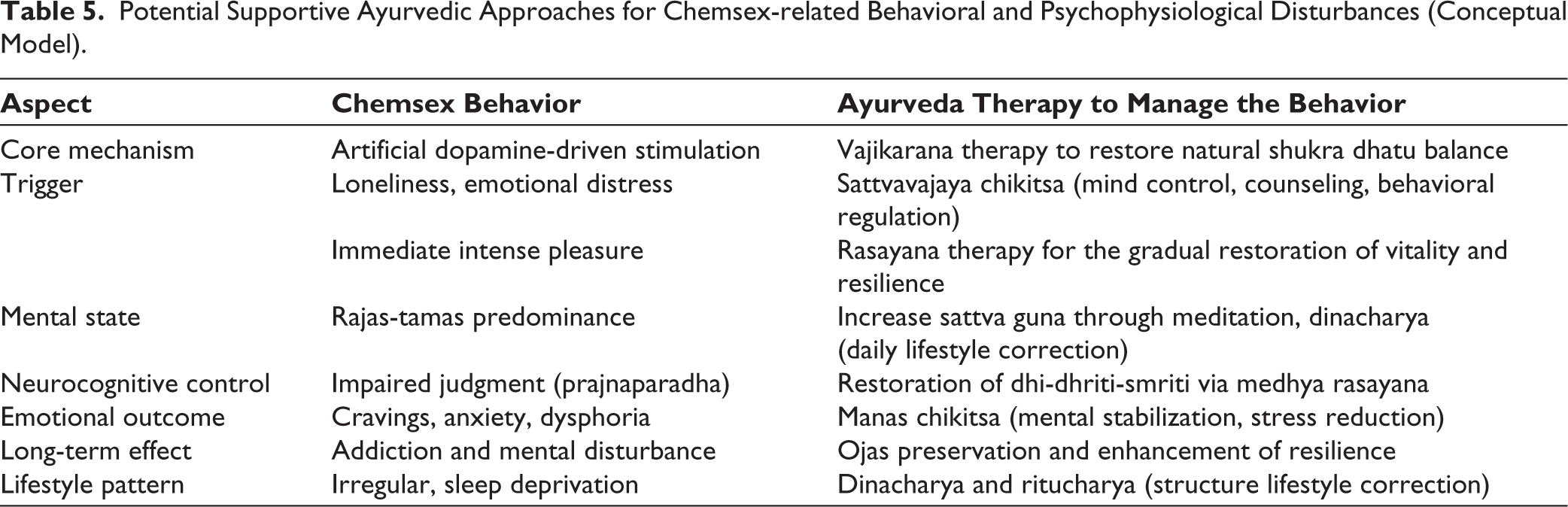
Such an integrative model may address not only compulsive behavior but also the psychosocial and lifestyle factors that may sustain the cycle. 24 It combines harm reduction, psychological interventions, and supportive restorative strategies within a broader recovery framework. It may offer a comprehensive recovery framework addressing biological, behavioral, and psychosocial dimensions of chemsex. Table 5 summarizes possible supportive Ayurvedic approaches within an integrative care framework.
Potential Supportive Ayurvedic Approaches for Chemsex-related Behavioral and Psychophysiological Disturbances (Conceptual Model).
Limitations
The Ayurveda-neuroscience correlations presented in this review are theoretical and currently lack direct empirical validation. Direct equivalence between constructs such as ojas and dopamine dysregulation should not be assumed and remains hypothetical. The integrative model proposed in Table 4 is a conceptual framework, not a proven biological mechanism.
Much of the available chemsex literature focuses on MSM populations, which may limit generalizability to heterosexual, female, transgender, or culturally diverse populations.
The search strategy was limited to English-language publications, potentially excluding relevant nonEnglish evidence.
Although this study employed a comprehensive review approach, formal risk-of-bias assessment, and quantitative meta-analytic synthesis were beyond its scope.
Publication bias and heterogeneity of available evidence may have influenced interpretation.
Future Directions
Empirical testing of culturally adapted and evidenceinformed Ayurveda-based supportive interventions for chemsex recovery.
Cross-cultural validation of integrative explanatory models across diverse settings.
Epidemiological and clinical research in South Asian and other underrepresented non-Western settings.
Longitudinal studies examining chemsex trajectories, relapse patterns, and treatment outcomes in diverse populations.
Prospective and interventional studies evaluating culturally adapted integrated treatment pathways are warranted.
Conclusion
Chemsex represents a complex intersection of sexuality, psychoactive substance use, mental health, and social context. Although some individuals report short-term enhancement of pleasure or intimacy, repeated involvement may be associated with dependence, psychological distress, infectious risk, and impaired functioning. From a neurobiological perspective, chemsex-associated substances may contribute to dysregulation of reward pathways and reinforce compulsive behavioral cycles. From an Ayurvedic perspective, the phenomenon may be interpreted through constructs related to impaired judgment, disturbed mental balance, depletion, and loss of resilience. These traditional interpretations are conceptual and should not be regarded as direct biological equivalence claims. Future clinical responses should prioritize compassionate, evidence-based, multidisciplinary, and culturally responsive approaches integrating sexual health, addiction treatment, and psychosocial recovery.
Footnotes
Acknowledgements
The authors sincerely thank mentors and colleagues whose guidance supported the preparation of this manuscript.
Authors’ Contribution
Dr Aashish Patel: Conceptualization, visualizations, writing, editing, validation, and methodology. Dr Suhas K Shetty: Writing, reviewing, and editing. Dr Vaishnavi G Kulkarni: Conceptualization, reviewing, validation, and methodology.
Data Availability Statement
No new datasets were generated or analyzed in this review.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethical permission was not applicable to this article, as this is a review article drafted from various research articles and not from patients directly.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Not applicable.