
Abstract
Background:
Female sexual dysfunction (FSD) is a multifaceted health concern encompassing disturbances in desire, arousal, orgasm, and satisfaction, significantly impacting women’s quality of life. Despite growing female participation in night-shift occupations, data on their sexual health remain scarce in India.
Aim:
This study aimed to determine the prevalence of FSD among Indian women engaged in night-shift work, identify associated sociodemographic and occupational factors, and evaluate the impact of work duration and shift frequency on the severity of sexual dysfunction.
Methods:
A cross-sectional study was conducted among 154 female healthcare workers aged 21–45 years employed in night shifts for six months or more. Participants completed a semi-structured sociodemographic and occupational proforma and the validated 19-item Female Sexual Function Index (FSFI). Data were analyzed using descriptive statistics, chi-square tests, and tests for linear trend, with a P value < .05 considered significant.
Results:
The prevalence of FSD was 55.2%. Desire and arousal were the most affected domains, followed by satisfaction and pain. The prevalence of FSD was significantly higher among older women, those in upper socioeconomic classes, and participants working ≥ 15-night shifts per month or with shift durations ≥ 6 hours.
Conclusion:
FSD is highly prevalent among Indian women working night shifts, with occupational stress, irregular sleep schedules, and longer shift durations as major contributors. Addressing these modifiable factors through workplace interventions, counseling, and health education may improve sexual and overall well-being in this population.
Keywords
Introduction
Female sexual dysfunction (FSD) is a multidimensional health issue encompassing disturbances in desire, arousal, orgasm, and sexual pain, significantly affecting a woman’s quality of life and interpersonal relationships. Despite being highly prevalent, FSD remains underreported and poorly understood, particularly in conservative societies like India, where discussions on sexual health are often stigmatized.1,2 Globally, the prevalence of FSD ranges from 30%–60%, depending on the population studied and the assessment tools used.3,4 In India, community-based studies indicate prevalence rates of 40%–55% among women, with higher rates observed among those experiencing psychological stress and chronic medical conditions.5,6
The increasing participation of Indian women in the workforce, particularly in sectors such as healthcare and information technology, has led to an expansion of non-traditional work patterns, including night shifts. Night-shift work disrupts the body’s circadian rhythm and sleep-wake cycle, leading to hormonal imbalances and psychosocial stress. These disruptions are known to adversely affect emotional stability, relationship satisfaction, and sexual function.7,8 The imbalance in melatonin and cortisol levels associated with shift work may influence estrogen and testosterone secretion, further contributing to decreased libido and sexual arousal. 9
Women working night shifts often experience fatigue, insomnia, irritability, and menstrual irregularities, which can exacerbate sexual dysfunction.10,11 Additionally, work-related stress, limited social interaction, and reduced partner communication may further impair intimacy and sexual satisfaction. Indian studies focusing on FSD among night-shift workers remain scarce, and the issue is often overlooked in occupational and mental health research. 12 Furthermore, cultural norms and reluctance to discuss sexual concerns contribute to significant underdiagnosis and inadequate management of FSD in India. 13
Understanding the prevalence and correlates of FSD among Indian women working night shifts is essential for formulating preventive and therapeutic interventions. This study aims to explore the prevalence, associated factors, and sociodemographic correlates of FSD among Indian women employed in night-shift occupations.
Materials and Methods
Study Design and Setting
Before commencing the study, ethical approval was obtained from the Institutional Ethics Committee (IEC) of a tertiary care center in Udaipur. This hospital-based cross-sectional study was conducted among adult women employed in night-shift healthcare roles at our institution. The study was carried out over a three-month period from October to December 2025.
Study Population and Sampling
The sample size was estimated using the formula:
where P represents the estimated prevalence of FSD, taken as 73.3% from a previous study; 14 d denotes the allowable margin of error (10%); Z₁₋α/₂ = 1.96 corresponds to a 95% confidence interval, and Z₁₋ᵦ = 0.8413 corresponds to 80% study power. The minimum required sample size thus calculated was 154 participants.
Inclusion and Exclusion Criteria
Female healthcare professionals aged 21–45 years, engaged in night-shift work for at least the preceding six months, sexually active within the past six months, and willing to provide written informed consent were included in the study. Participants were excluded if they had diagnosed psychiatric disorders; known gynecological or endocrine disorders affecting sexual health (e.g., polycystic ovarian syndrome, diabetes mellitus, hypothyroidism); were pregnant or within six months postpartum; were using medications known to impair sexual function (such as selective serotonin reuptake inhibitors or beta-blockers); had current or past substance use (including alcohol, tobacco, or psychoactive substances); or had a history of spinal cord injury or pelvic/perineal trauma known to impair sexual function.
Data Collection Procedure
Data were collected using a structured, self-administered questionnaire that included the Female Sexual Function Index (FSFI).
Tools
The FSFI is a validated 19-item scale designed to assess key domains of female sexual function: desire, arousal, lubrication, orgasm, satisfaction, and pain. The FSFI was used as it is a widely applied, psychometrically validated instrument for assessing FSD across six domains and has been reliably utilized in Indian populations.5,14,15
Participants who met the inclusion criteria were briefed about the study, and those who provided informed consent completed the FSFI along with a semi-structured sociodemographic and occupational proforma including age (years), occupation, relationship status, living arrangement, residence, family type, socioeconomic status (SES), number of children, night shifts per month, and average shift duration. FSFI domain scores were calculated as per standard procedures, and a total FSFI score <26.55 was used to define FSD. The questionnaire was distributed during work hours in a private setting to ensure confidentiality and minimize response bias. All responses were anonymized prior to analysis. Participation in the study was entirely voluntary. The confidentiality of all personal and health-related data was strictly maintained, and participants retained the right to withdraw from the study at any point without any penalty.
Statistical Analysis
The data was entered into Microsoft Excel and analyzed using the Statistical Package for Social Sciences (SPSS) software version 16. Descriptive statistics (mean, standard deviation, frequency, and percentage) were used to summarize sociodemographic, occupational, and sexual function variables. The FSFI total score was dichotomized at 26.55 to classify participants as having FSD or normal sexual function. Associations between participant characteristics and FSD status were examined using chi-square tests. Domain-specific dysfunction (FSFI domain score below the respective cut-off) was compared across occupation and relationship categories using chi-square tests, and across ordered categories of night-shift frequency and shift duration using chi-square tests for linear trend. A P value < .05 was considered statistically significant.
Results
Table 1 shows that a total of 154 female healthcare workers participated in the study. More than half of the participants were aged 21–30 years (53.2%), and nurses formed the largest occupational group (44.2%). Nearly half were married (49.4%), and 50.6% lived with their families. The majority were urban residents (66.2%), belonged to nuclear families (63.6%), worked fewer than 15-night shifts per month (54.5%) and reported shift durations of ≥ 8 hours (58.4%).
Sociodemographic and Occupational Characteristics of Participating Female Healthcare Workers (N = 154).
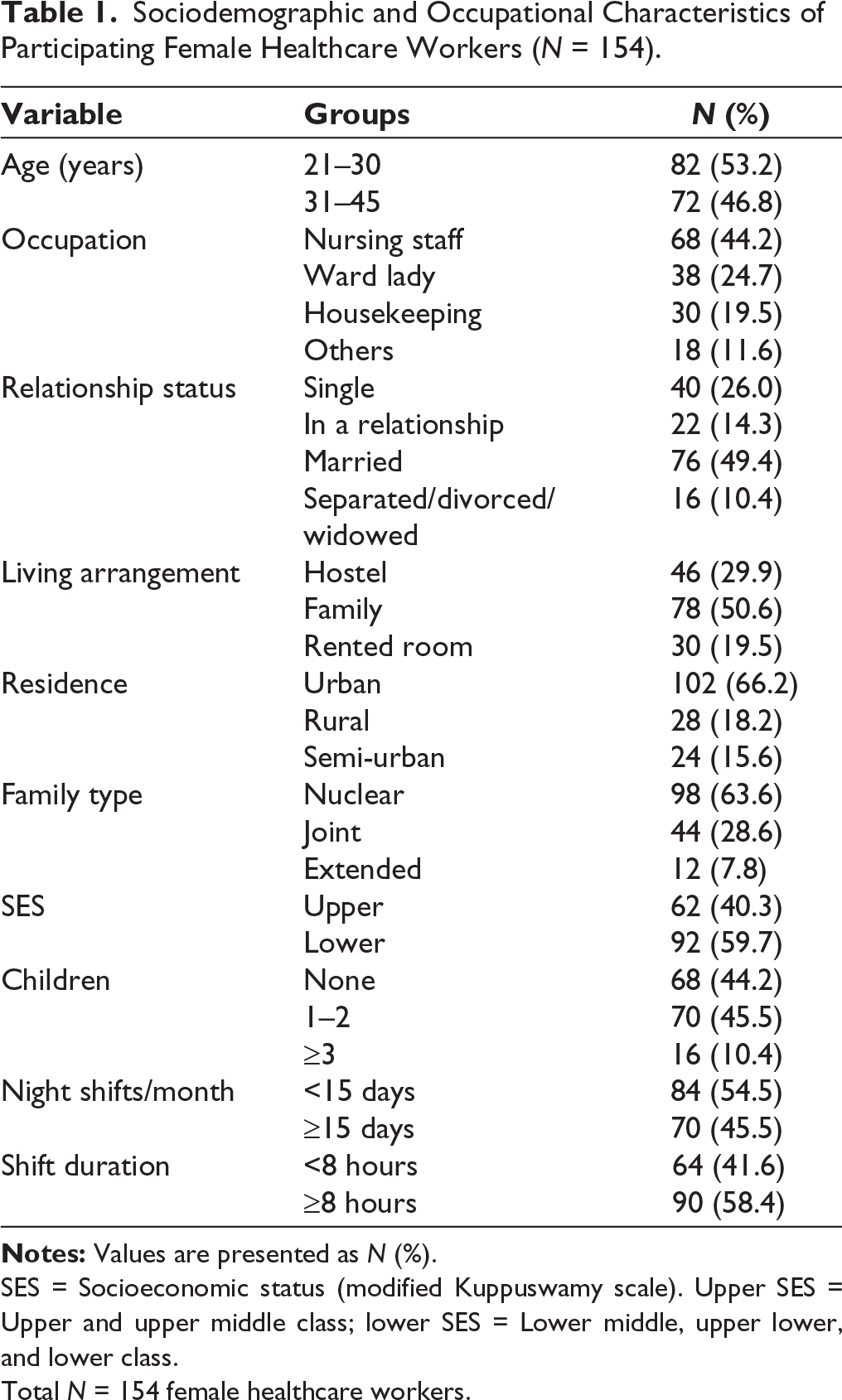
SES = Socioeconomic status (modified Kuppuswamy scale). Upper SES = Upper and upper middle class; lower SES = Lower middle, upper lower, and lower class.
Total N = 154 female healthcare workers.
The overall mean FSFI total score was 25.1 ± 5.9, and 55.2% of participants were identified as having FSD. The orgasm (4.0 ± 1.1) and lubrication (3.9 ± 1.0) domains had the highest mean values, followed by satisfaction (3.8 ± 1.2) and pain (3.7 ± 1.3). The lowest mean scores were observed in the arousal (3.5 ± 1.2) and desire (3.2 ± 1.1) domains (Table 2).
FSFI Total and Domain Scores, and Prevalence of FSD.
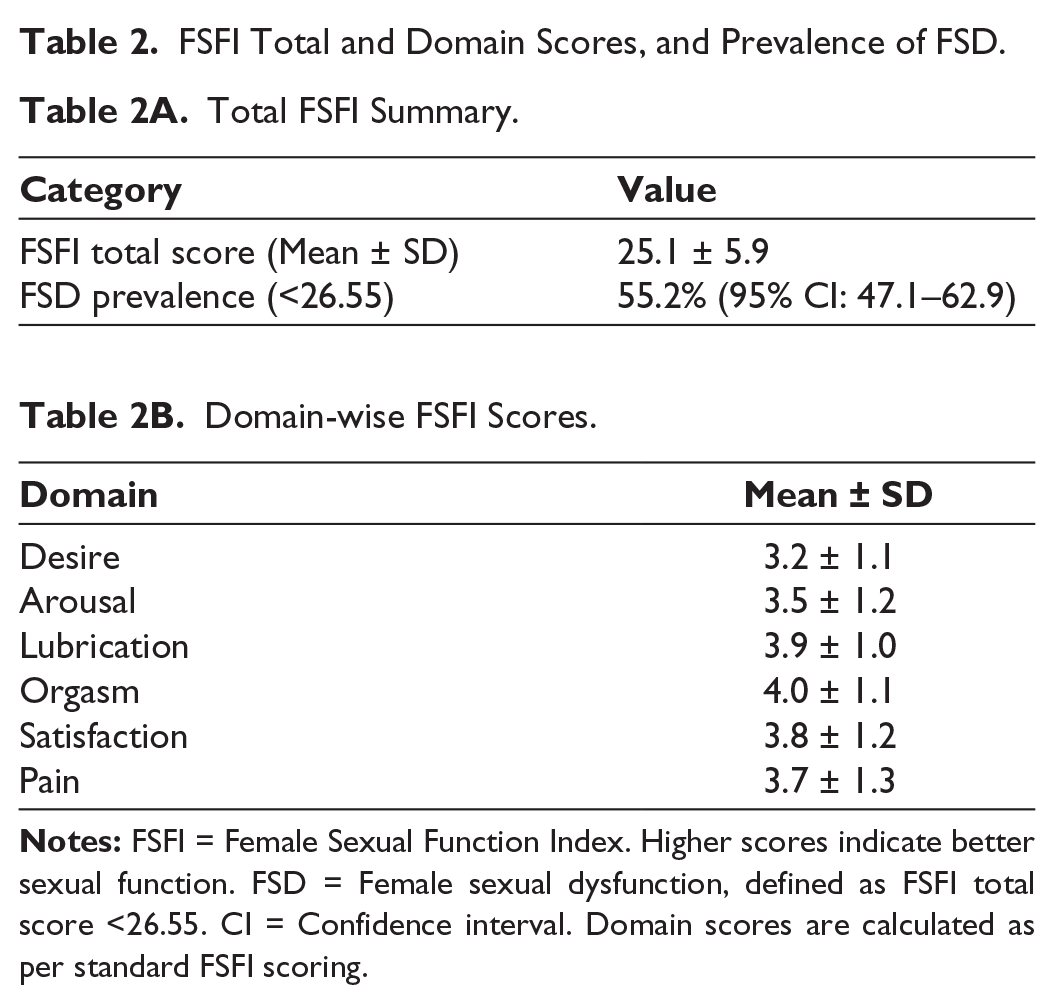
Table 3 shows that women aged 31–45 years, separated/divorced/widowed women, those with higher parity, higher night-shift frequency, longer shift duration, and upper SES reported significantly higher dysfunction (P = .028, P = .002, P = .015, P = .010, P = .025, and P = .006, respectively).
Prevalence of FSD (FSFI < 26.55) by Participant Characteristics.
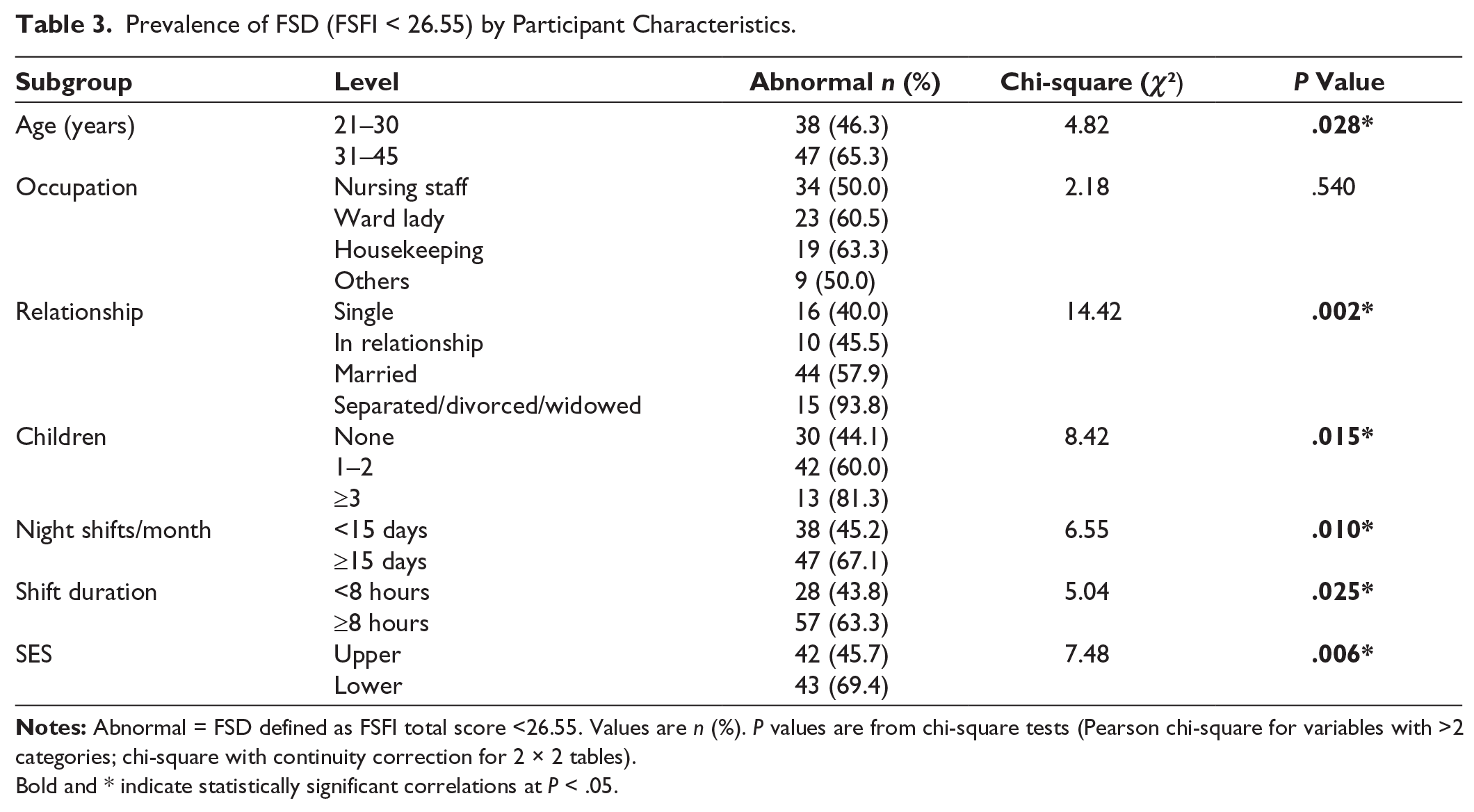
Bold and * indicate statistically significant correlations at P < .05.
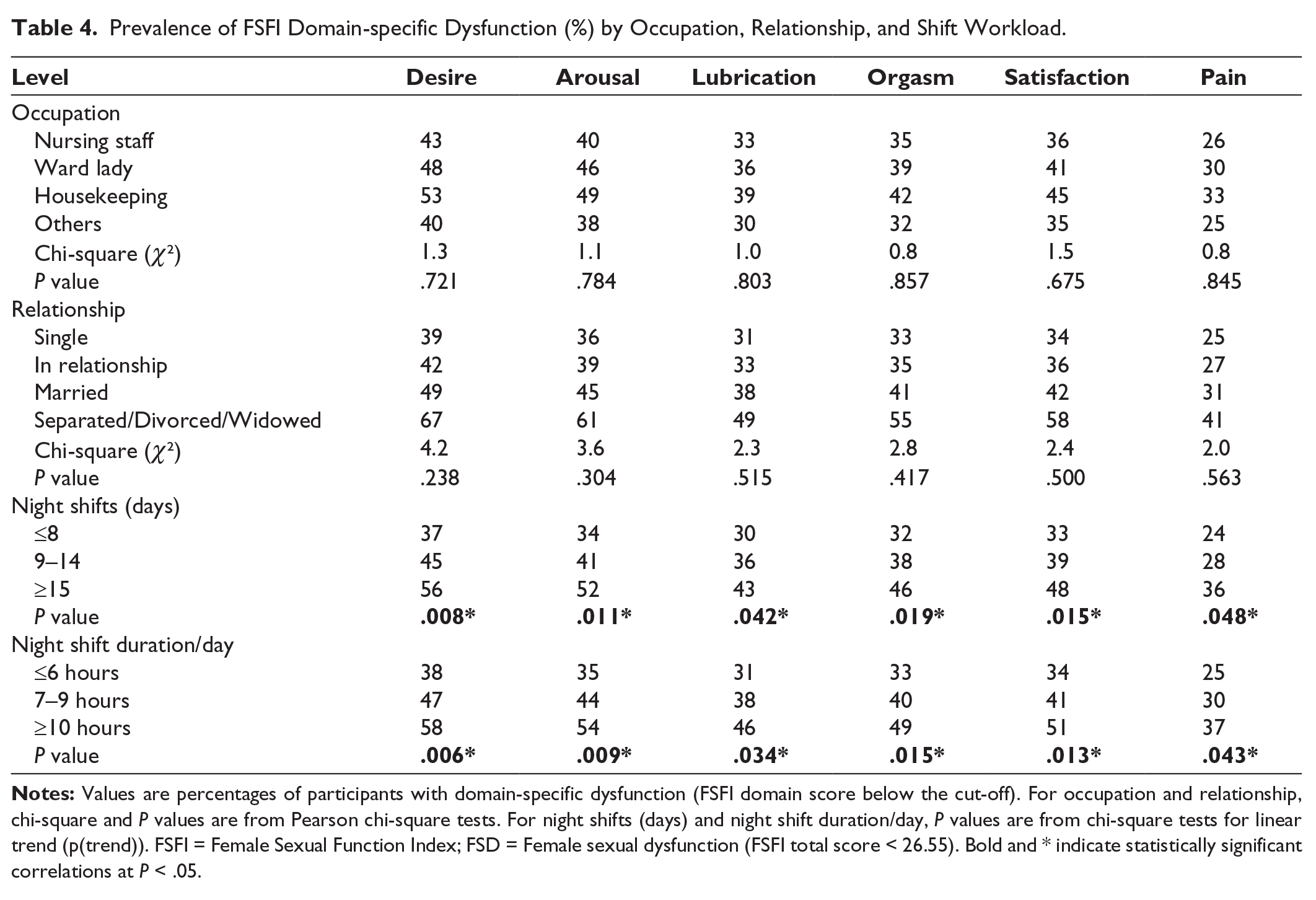
Increasing night-shift frequency per month was significantly associated with higher proportions of domain-specific dysfunction, with P for trend ranging from 0.008 to 0.048. Longer night-shift duration per day showed a similar progressive increase in dysfunction across all FSFI domains, with P for trend ranging from .006 to .043 (Table 4).
Prevalence of FSFI Domain-specific Dysfunction (%) by Occupation, Relationship, and Shift Workload.
Discussion
The present study observed that the majority of the participants were younger women, with nursing staff representing the largest occupational group. These findings align with prior Indian studies on women working night shifts, where hospital-based samples are predominantly composed of younger nurses and other female healthcare workers.10,12 Most participants were married and resided with their families. Singh JC et al. and Singh N et al. found that marital responsibilities, relationship demands, and psychosocial stressors can contribute to fatigue and poorer sexual well-being in women.5,6 The predominance of nuclear families and urban residency in our study mirrors the profile of urban women working night shifts reported in previous Indian research, which also highlights that these factors are associated with sleep disturbance, stress, and health problems that increase the risk of FSD.10,12
The distribution of FSFI scores in this study indicates that more than half of the women experienced sexual dysfunction, demonstrating that FSD is common among night-shift workers. These findings are consistent with earlier Indian research.5,6,14 James et al. and Bracci et al. emphasized that shift work adversely affects hormonal regulation and emotional stability, which explain the high proportion of women reporting dysfunction in the current study.7,9 Collectively, the findings suggest that night-shift work exerts a substantial influence on sexual health.
Domain-wise analysis revealed that desire and arousal were the most affected areas. Similar patterns, with greater impairment in emotional and motivational components of sexual function than in purely physiological domains, have been reported in previous international and Indian studies.4,5,14 Lower desire scores in the present study align with prior research linking sleep disturbance and psychosocial strain to sexual dysfunction in women.7,11 This pattern likely stems from chronic fatigue, sleep deprivation, and reduced partner interaction. Reduced arousal further mirrors the hormonal and circadian imbalances associated with night work, as observed by Bracci et al. 9 Overall, these results emphasize that psychological and interpersonal factors, rather than physical limitations alone, are key contributors to FSD in this occupational group.
FSD was more prevalent among older women, those in upper socioeconomic groups, and participants with longer or more frequent night shifts. Similar age and socioeconomic gradients in sexual dysfunction have been reported in Indian studies using the FSFI,5,6,14 while studies of female shift workers highlight that higher night-shift burden is associated with greater psychological strain and impaired sexual life.8,10,12 Marital status also influenced outcomes in our study, with separated or divorced women showing the highest levels of dysfunction, consistent with international and Indian research that found non-cohabiting or distressed marital relationships are linked to more sexual problems.3,6,13,14 Overall, these findings underscore the need for targeted strategies focusing on workload distribution, shift management, and the compounded effects of psychosocial stress, irregular sleep, and family responsibilities on sexual well-being among working women.
The progressive increase in dysfunction with rising night-shift frequency and longer daily shift duration in our study is consistent with Bilge Ç et al., where female nurses having heavier shift loads have been linked to higher depressive symptoms and poorer sexual life, 8 and with studies showing that extended night work disrupts circadian and hormonal regulation and is associated with poorer quality of life.7,9 An Indian multicentric study further demonstrated that greater night-shift intensity and rotating schedules are associated with more sleep-related and health problems among nurses, which may in turn contribute to reduced sexual well-being. 10 Taken together, these findings underscore that FSD among night-shift workers is multifactorial and therefore requires holistic management interventions.
Strengths and Limitations
The present study is one of the few Indian studies assessing FSD among night-shift working women using a validated instrument (FSFI). Inclusion of varied healthcare job categories and analysis of night-shift frequency and duration enhanced the comprehensiveness and applicability of the findings. However, its cross-sectional design limits causal inference, and the single center setting limits generalizability. Reliance on self-reported data may have introduced response bias, especially given cultural sensitivities surrounding sexual health. Additionally, other confounding factors such as partner variables, sleep quality, stress, and hormonal influences were not assessed, which could have affected the observed associations.
Conclusion
In conclusion, this study highlights a high prevalence of FSD among Indian women working night shifts, emphasizing that occupational stress, irregular sleep-wake patterns, and longer and more frequent night duties significantly affect sexual well-being. Desire and arousal emerged as the most affected domains, reflecting the combined influence of physiological fatigue, disrupted circadian rhythm, and psychosocial strain. Older age, marital status, and upper socioeconomic background further contributed to increased vulnerability. These findings underscore the need for workplace policies promoting balanced shift schedules, adequate rest periods, and psychological support systems to safeguard women’s reproductive and mental health. Awareness, destigmatization, and routine screening for sexual dysfunction should be integrated into occupational and women’s health programs to enhance overall quality of life for female night-shift workers.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Before conducting the study, approval from Human Research Ethics Commitee (HREC) was taken (GU/HREC/EC/2025/2734).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
The participants who provided their written informed consent, participated in this study.