
Abstract
Background:
Negative sexual cognition and sexual anxiety create a substantial amount of distress and guilt in an individual, which in turn can lead to reduced well-being. However, the impact of sexual cognition and sexual anxiety on mental health are less researched topics, especially in the Indian context.
Aim:
To investigate the effect of sexual cognition and sexual anxiety on mental health.
Method:
124 participants of age range 18–35 years were recruited using purposive sampling method. Sexual Cognition Checklist, Sexual Anxiety Inventory, and Mental Health Inventory were used to assess sexual cognition, sexual anxiety, and mental health respectively.
Results:
Mental health was significantly negatively associated with sexual anxiety and negative sexual cognition. Also, a significant positive correlation was found between positive sexual cognition and mental health. Negative sexual cognition and sexual anxiety emerged as significant predictors, accounting for approximately 20% and 6% of the variance in mental health, respectively. Finally, an independent sample t-test suggests that males and females significantly differ in their level of sexual cognition, mental health, and sexual anxiety.
Conclusions:
Negative sexual cognition and sexual anxiety are associated with poor mental health while positive sexual cognition is associated with better mental health. Unmarried Indian women tend to experience more negative sexual cognition and sexual anxiety than married women.
Introduction
Sexual cognitions are very common among youth. Sexual cognition refers to a wide range of thoughts, images, and fantasies related to sex or sexual activity. 1 These cognitions are mostly considered as pleasurable and positive in nature. However, it can also be negative, undesirable, disturbing, and unacceptable. 2 As any other undesirable experiences, negative sexual cognitions create significant stress, anxiety, guilt, etc., which in turn can lead to reduced overall well-being. Previous researches have mainly focused on the positive aspects of sexual cognition 3 and there is a paucity of studies regarding negative sexual cognition and its impact on the overall health.
Sexual health is an integrated aspect of mental health.4–6 Healthy and proper sexual functioning adds positively to the well-being which in turn promotes overall health of an individual. 7 People who are sexually fit and healthy experience better mental health. Similarly, people with poor sexual life feel worse mental health because it creates a feeling of inadequacy and embarrassment.5 Previous researches reported a positive association between positive sexual health and mental health. 8 Likewise, in a study, Hensel et al. 9 found that positive sexual health was significantly positively associated with better health. The association of mental and sexual health has been well documented in western, but is less explained in the Indian society.
Sexual anxiety is defined as the tendency to experience tension, discomfort, and anxiety about the sexual aspects of one’s life. 10 Sexual anxiety is often related to concern about performance, worries, sexual health, and body image. Sexual anxiety and worry are found among people of all ages. 11 These anxieties can be related to self-adequacy, 8 performance as well as to the sustainability of better sexual relationship with the partner. Research suggests a strong and positive association between anxiety and functional impairment, 12 this is also found true in case of sexual anxiety and sexual functioning. In a study, Montesi et al. 13 assessed 115 undergraduate students and found a significant association between sexual anxiety and lower sexual satisfaction. Similarly, Mourikis et al. 14 reported that men with more anxiety face higher sexual dysfunction. Anxiety has been considered as the major factor that plays role in sexual dysfunctions. 15 As, sexual dysfunction and mental health are found to be associated, sexual anxiety can also affect mental health, however, the role of sexual anxiety on the overall mental health has not been well explored especially in the Indian context. India perceives sex as a taboo thing, which is not discussed or educated openly. 16 In youth, the unavailability of proper sex education plays a major role in sexual anxiety and self-doubt. Hence, there is a good reason to explore various sexual anxieties among married and unmarried Indian youth.
Gender and sexuality have been found to be associated with each other.17,18 Previous studies found significant gender difference1,19 in sexual desires and behaviors. Males feel sexual desires more strongly than females. 1 Similarly, Carvalho and Nobre 20 reported a significant gender difference in sexual attitudes and beliefs. However, in another study, Dawson and Chivers 21 reported no gender difference on the level of sexual desires. On the other hand, it has been reported that females experience more anxiety and mood disorders than men. 22 However, no Indian study has been found which examined the gender difference in the context of sexual anxiety and sexual cognition.
On the basis of literature review, it can be said that there is a dearth of research concerning the sexual cognition and sexual anxiety of the Indian youth and its association with mental health. Most of the available researches are conducted in western countries. However, these finding cannot be generalized in Indian Societies for two major reasons, first, in India sex is more tabooed topic than western, and second, sexuality and gender roles are viewed and defined differently from western countries. 16 Therefore, the present study aimed to investigate the effect of sexual cognition and sexual anxiety on the mental health of Indian youth.
Objectives
This research aims to investigate the relationship of sexual anxiety and sexual cognition with mental health. Also, the study sought to identify the potential predictor of mental health in terms of sexual cognition and sexual anxiety. Lastly, the study aimed to examine the gender difference in mental health, sexual cognition, and sexual anxiety among youth.
Subjects and Methods
A total of 124 participants (male = 62, female = 62) were selected for the study, using purposive sampling method. All the participants were 18–35 years old and had educational qualification 8th grade and above. Only the participants who gave consent to participate were included in the study. The mean age of the female participants was 25 years, while the mean age of male participants was 26 years. Out of 124 participants, 62% were belonging from rural area and 38% were from urban area. Approximately, 51% (n = 63) of the participants were educated up to undergraduate level and 49% (n = 61) were educated up to postgraduate level.
Ethical Approval and Patient Consent
The Institutional Ethics Committee, Institute of Medical Sciences, B.H.U., gave permission to conduct the research. Anonymity of all participants was maintained and informed consent was taken from all the participants. No personal details such as name, contact number, and address were asked from the participants and their responses on questionnaires were not discussed outside the research context.
Tools
Sexual Cognition Checklist 23
The Sexual Cognitions Checklist (SCC) measures positive and negative sexual cognitions. 23 It consists of 56 items. The SCC is appropriate for men and women of any age and sexual orientation. The total score ranges from 0 to 336, with higher scores indicating more frequent positive or negative cognitions. Internal consistency of the scale ranged between 0.66 and 0.84.
Sexual Anxiety Inventory (SAI) 24
The SAI measures anxiety related to sexual activity. It is a 25-item scale, with one alternative representing an anxiety response and the other a nonanxiety response. The respondents circle the letter of the alternative that comes closest to describing their feelings. Internal consistency of the scale was found 0.86 and test–retest reliability was reported 0.85. Validity of the scale was also found high.
Mental Health Inventory 25
Mental Health Inventory assesses the overall mental health of an individual. This scale consists of 56 items. The reliability of the scale is 0.73, while the validity of the scale is 0.56. This scale consists of items with four alternative responses that is “always” (4), “often” (3), “rarely” (2), and “never” (1).
Procedure
All the participants were communicated separately by the researcher and educated about the study. Most of the data was collected personally by the researcher and some data were collected via internet to increase the reach. Informed consent was obtained from participants and asked to complete questionnaire such as socio-demographic datasheet, SCC, Sexual Anxiety Questionnaire, and Mental Health Inventory. Finally, scoring was done using standard scoring procedure.
Statistical Analysis
After the data collection, obtained responses were analyzed with the help of IBM Statistical Package for Social Sciences-19. Pearson’s product moment correlation coefficients were calculated to assess the association between sexual cognition and sexual anxiety and mental health. Further, regression analysis was carried out to assess the extent to which sexual cognition and sexual anxiety predict mental health. Lastly, independent sample t-test was also carried out to measure gender differences in terms of positive and negative sexual cognition, sexual anxiety, and mental health.
Results
Correlation Result
Correlation coefficient was calculated in order to determine the strength of the relationship among sexual cognition, sexual anxiety, and mental health. The obtained correlation coefficient is presented in Table 1.
Correlation Analysis of Mental Health, Sexual Cognition, and Sexual Anxiety.

Table 1 reveals that mental health was significantly positively correlated to positive sexual cognition (r = 0.26, p < .01). It suggests that individual who experience more positive sexual cognition have better mental health. On the other hand, scores of mental health were significantly negatively correlated to negative sexual cognition (−0.41, p < .01) and sexual anxiety (r = −0.40, p < .01). Poor mental health is linked with higher level of negative sexual cognition and more sexual anxiety. Moreover, scores of sexual anxiety were significantly negatively correlated with the scores of negative sexual cognition (r = −0.30, p < .01). The findings further indicate that higher sexual anxiety leads to higher negative sexual cognition or vice-versa.
Table 2 presents the result of regression analysis. In the first model, negative sexual cognition was entered. Further, in the second model, sexual anxiety was added to the regression, in addition to the negative sexual cognition. Among these two predictors, negative sexual cognition explained the largest portion (19%) of variance, followed by sexual anxiety, explaining 6% of variance in predicting mental health. Altogether, these two variables explained 25% variance.
Summary of Stepwise Regression Analysis of Negative Sexual Cognition and Sexual Anxiety as Predictors and Mental Health as Criterion.

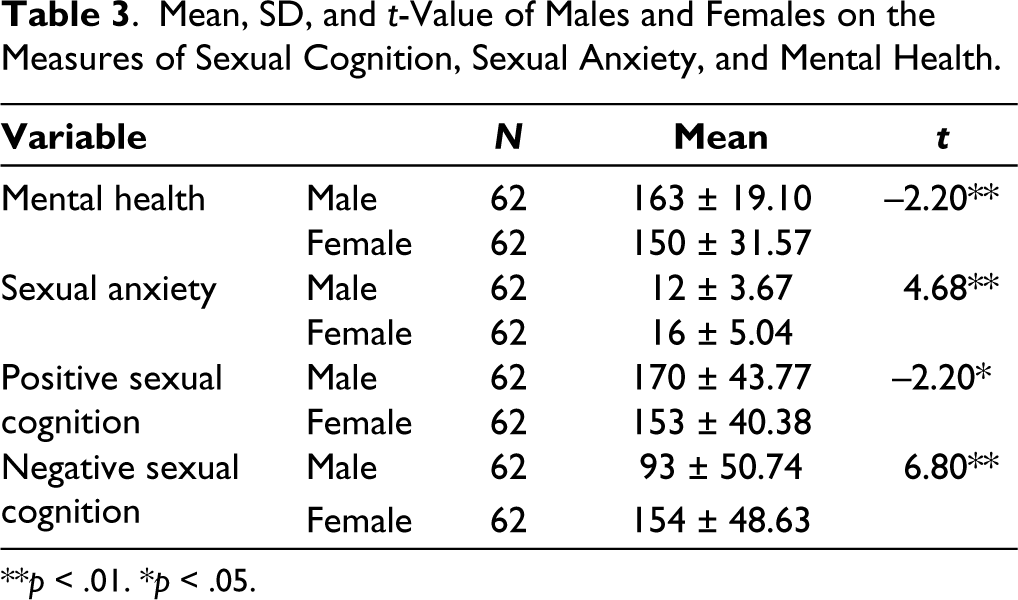
Table 3 presents the group comparison by gender for sexual cognition, sexual anxiety, and mental health. Women scored significantly higher (mean = 154 ± 48.63) than men (93 ± 50.74) on negative sexual cognition. Further, females also scored significantly higher (16 ± 5.04) than men (12 ± 3.67) on sexual anxiety. On the other hand, males scored higher on positive sexual cognition and mental health. Mean scores for male on positive sexual cognition and on mental health were 170(±43.77) and 163(±19.10), respectively, while for female it was 153(±40.38) and 150(±31.57), respectively. Overall the present finding shows that females experience higher negative sexual cognition and sexual anxiety than males.
Mean, SD, and t-Value of Males and Females on the Measures of Sexual Cognition, Sexual Anxiety, and Mental Health.
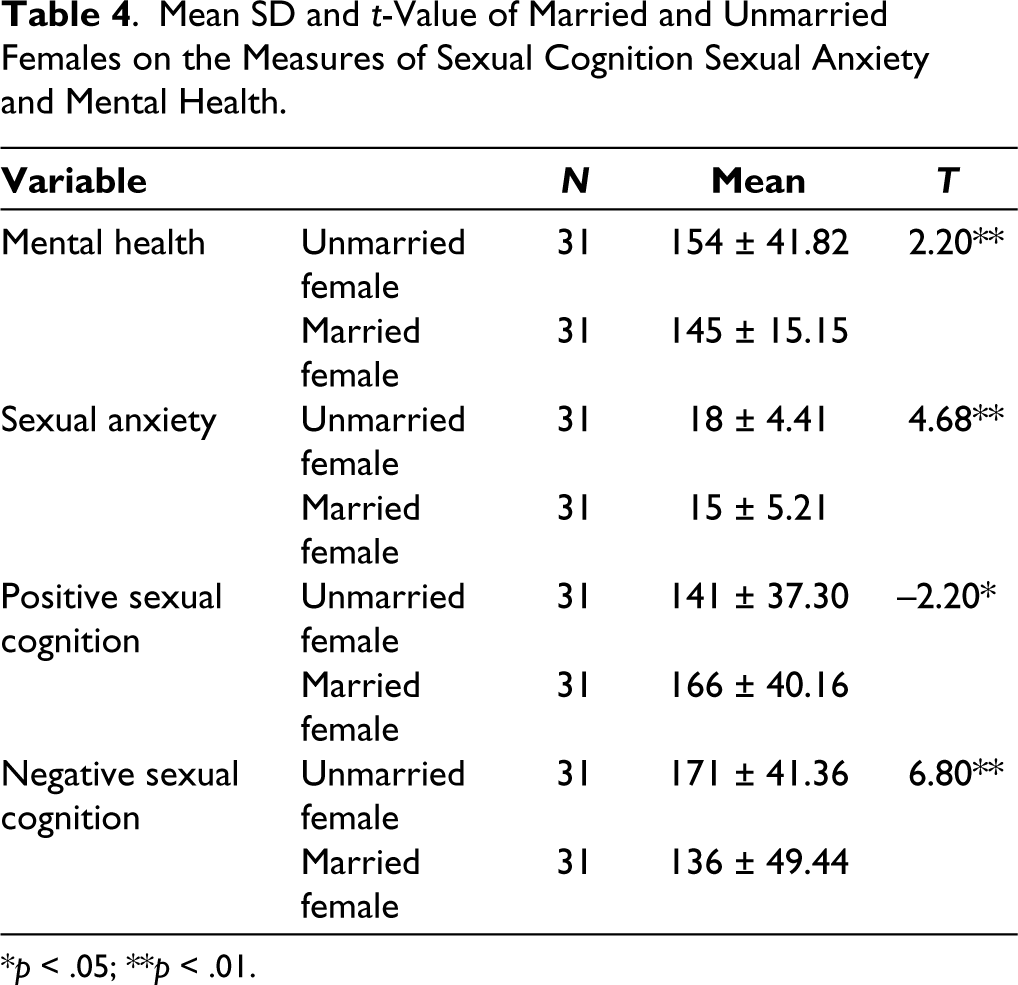
Results of independent sample t-test (Table 4) show that unmarried females scored higher on negative sexual cognition (171 ± 41.36), sexual anxiety (18 ± 4.41), and mental health (154 ± 41.82) than married females. Unmarried females mean score for mental health, sexual anxiety, and negative sexual cognition was 145(±15.15), 15(±5.21), and 136(±49.44), respectively. On the other hand, married females showed higher level of positive sexual cognition (166 ± 40.16) than unmarried females (141 ± 37.40).
Mean SD and t-Value of Married and Unmarried Females on the Measures of Sexual Cognition Sexual Anxiety and Mental Health.
Discussion
This research work aimed to investigate the relationship of sexual cognition and sexual anxiety with the mental health of youth. Findings revealed that negative sexual cognition was negatively associated with mental health, while positive sexual cognition was found to be significantly positively correlated with mental health. It suggests that individuals with higher level of negative sexual cognition have shown poor mental health. On the other hand, individual with higher level of positive sexual cognition reported better mental health. The probable reason for it can be that negative sexual cognitions are often ego-dystonic, 2 and create a feeling of distress, anxiety, and sometimes disgust. Also, positive sexual cognition creates pleasurable and positive affect and helps in better sexual adjustment, while negative sexual cognition leads to poorer sexual satisfaction. 2 These negative feelings can adversely impact the mental peace and well-being. 26
Further present study also emphasizes that sexual anxiety is negatively associated with mental health, which means individuals with higher sexual anxiety experience poor mental health. This finding is corroborated by the other researchers also. 27 Anxiety is known to play a crucial part in sexual dysfunction28,29 as it interferes with normal sexual arousal and enjoyment.30,31 Mourikis et al. 14 found that state anxiety is linked with sexual dysfunction. Involvement in sexual activity in anxious mental state can cause fear about desirability and performance and sometimes feelings of embarrassment. As sexual satisfaction and pleasure is strong predictor of general well-being32,33; higher sexual anxiety can be seen as a predictor of poor mental health.
Negative sexual cognition and sexual anxiety have been found to be the significant predictors of poor mental health among youth. Negative sexual cognitions and sexual anxieties are the results of misconceptions, frustrations, and lack of knowledge. Sexuality is essentially a decent aspect of one’s life and not something bad, disgraceful, or shameful. Expression of desires, sexual identity, and orientation is a vital part of a healthy lifestyle. When these desires are suppressed, it creates a problem and leads to various anxieties.
Finally, with respect to gender, present study also demonstrated that men have more positive sexual desire than women. 34 Beck and Bozman 35 also reported gender difference in desires. Results of the present study show that female had higher sexual anxiety and negative sexual cognition than male. These outcomes are similar to the previous findings.2,17 One of the reasons for it can be that in India women sexuality is still not given that much consideration and in most cases women are not allowed to complain about sexual dissatisfaction or pain. 6 It is not accepted to talk about sexuality openly. Sex for the sake of pleasure and enjoyment often get associated with feelings of guilt or shame, especially in women, 6 so desiring about sex creates negative feelings. These societal pressure and misconceptions might play a role for sexual anxiety and negative cognitions.
In context with marital status, it was found that married women reported higher positive sexual cognition and lower sexual anxiety as well as lower negative sexual cognition than unmarried women. One reason for it can be that the tabooed nature of sex in India especially before marriage. 36 It is considered bad and unacceptable for unmarried youth, which might be the reason for higher negative sexual cognition and sexual anxiety among unmarried females.
A major difference was observed in the mental health of males and females. It was found that females were more vulnerable to poor mental health than males. The results are in line with the previous findings.37,38 In a recent study, Gulland 39 found that women, particularly young women are more likely to have mental health issues than males. One reason of it can be the existing gender differences in access of educational and health facilities. 39 Social and cultural factors might be one significant reason. 40 Gender disparity or inequity is still a crucial reality in India 40 and several Indian studies highlighted gender as a critical determinant of mental health. In context of sex, most often Indian men assume authority over women and most of the times retain it forcefully.37,41 Sexual violence, harassment, strict code of conduct, poor educational status, and common mentality of seeing women as a machine for childbirth and rearing 42 are responsible for the pathetic health status of females.
Present study can play very relevant role in the present scenario of India. Sexual violence and harassments have increased in India. Present finding will help to better understand the sexual desires and anxieties among youth, which might help in planning. Also, present study recommends that there is a need of well-planned sexual education for Indian adolescents and youths. Mental health workers believe that human being should have knowledge about their sexuality. Good scientific knowledge about sex empowers an individual to be able to make informed sexual choices, which further help everyone, whether young or old, to experience sex and sexuality as a healthier and better experience.
The findings of the present study must be interpreted in the light of certain limitations. First, a self-report measure was used to collect the data regarding sexual anxiety, sexual cognition, and mental health; therefore, there is a chance of biasness in the responses. Another limitation of the study is that it is a cross-sectional study; longitudinal studies might provide better understanding in this area. Also, the sample size of this study is relatively small. Apart from these limitations, there are few important factors that could influence sexual cognition and sexual anxiety namely, duration of sexual experience, use of family planning methods, sexual orientation, relationship with partner, desire to conceive, etc. The present study has not studied the impact of these factors, future studies should focus in this direction. However, to our knowledge, this is one of the few Indian studies that investigated the relationship between sexual cognition, sexual anxiety, and mental health.
Conclusion
In conclusion, sexual anxiety and negative sexual cognition have been found as the potential predictors of mental health among youth. Individuals with more negative sexual cognition and sexual anxiety display comparatively more poor mental health. There exists a significant gender differences in sexual behavior patterns, sexual needs, and sexual desires. Male participants had more positive sexual cognition than females. Also, married individuals experience comparatively more positive sexual cognition than married participants. Better knowledge of such dissimilarities can help in designing gender appropriate intervention techniques. 41 Also, better sex education will help youth to deal with their sexual anxieties and cognitions.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The ethical approval was obtained from Institutional Ethics Committee, Institute of Medical Sciences, B.H.U.
Funding
The authors received no financial support for the research, author-ship, and/or publication of this article.
Informed Consent
Informed consent participation in the study was completely voluntary. All the participants provided written informed consent to participate.