
Abstract
Background:
Sexual attitudes among medical students play a crucial role in shaping their competence and comfort in addressing patients’ sexual health needs. Despite growing attention to sexual health education, cultural and social influences continue to shape students’ perspectives, particularly in India.
Aim:
To assess the sexual attitudes of final-year medical students using the Brief Sexual Attitudes Scale (BSAS) and to examine their associations with key sociodemographic and behavioral variables.
Methods:
A descriptive, cross-sectional study was conducted among final-year undergraduate medical students at a private medical college in Udaipur, India. Data were collected using a validated, self-administered online questionnaire incorporating the BSAS. Descriptive statistics, independent-samples t tests, and Pearson correlations were used for analysis.
Results:
The highest BSAS subscale mean was for permissiveness, followed by instrumentality, birth control, and communion. Permissiveness was significantly higher among males (P = .038), those spending ≥3 h on social media (P = .016), and those exposed to sexually explicit content (P = .004). Birth control was significantly higher among females (P = .028) and older students aged ≥24 years (P = .032). Communion was higher among females (P = .014) and students in relationships (P = .042). Instrumentality was significantly associated with independent living (P = .023), greater social media use (P = .010), viewing explicit material (P = .004), and following relationship content (P = .011).
Conclusion:
Final-year medical students demonstrated moderately liberal sexual attitudes, with permissiveness and instrumentality domains reflecting increasing openness influenced by gender and online exposure, with schooling type also associated with more permissive attitudes. However, emotional and contraceptive domains remained conservative. Integrating structured and culturally sensitive sexual health education into medical curricula is essential to promote professional competence and non-judgmental patient care.
Keywords
Introduction
Sexual health is an integral component of overall well-being and an important aspect of medical education. The attitudes of future physicians toward sexuality and sexual health can influence their comfort, competency, and sensitivity in addressing patients’ sexual concerns. 1 Despite its relevance, sexual health education often remains inconsistently integrated into medical curricula worldwide, leading to varied knowledge levels and attitudes among medical students.2,3
Studies have indicated that medical students’ sexual attitudes are shaped by multiple factors, including cultural norms, personal experiences, gender, religion, and exposure to formal sex education.4,5 In conservative societies, sexuality may still be regarded as taboo, creating barriers to open discussion and understanding of sexual diversity and health issues. 6 Consequently, medical students in such environments may demonstrate discomfort or moral conflict when addressing patients’ sexual concerns. 7
Previous surveys across different regions have shown a wide spectrum of sexual attitudes among medical students. International studies highlight relatively liberal views on premarital sex and sexual diversity,8,9 while studies from Middle Eastern and South Asian contexts reveal more conservative perspectives influenced by sociocultural and religious values.10,11 This diversity underscores the need for culturally sensitive, evidence-based sexual health education that balances professional competence with ethical and cultural awareness. 12
Several studies conducted in India have examined sexual attitudes among medical students, revealing a complex interplay between modern medical education and deeply rooted cultural values. Research from various regions shows that while many medical students display increasing openness toward discussing sexual health, significant gaps remain in knowledge and comfort regarding sexual diversity and contraception counseling.13–15 Sharma et al. reported that only half of final-year students felt confident addressing patients’ sexual issues despite acknowledging its clinical importance. 13 Similarly, a study from South India highlighted conservative views toward premarital sex and same-sex relationships, largely influenced by socioreligious norms. 14 Inadequate curricular exposure to sexual health topics has been identified as a consistent barrier to developing professional competency in sexual medicine.15,16
Final-year medical students are nearing the transition from training to clinical practice. Their beliefs and attitudes will directly affect how they address patients’ sexual health needs and provide non-judgmental care.17,18 Therefore, this study aims to assess the sexual attitudes among final-year undergraduate medical students and explore the influence of demographic and cultural factors on these attitudes.
Materials and Methods
Study Design and Setting
This study employed a descriptive, cross-sectional survey design conducted among final-year medical students. Before commencing the study, approval was obtained from the Institutional Ethics Committee. The study was carried out over a period of three months between January and March 2025. A cross-sectional approach was chosen as it allows for assessment of existing attitudes and perceptions toward sexuality within a defined academic cohort at a single point in time. 19
Participants and Sampling
The study population included all consenting final-year Bachelor of Medicine, Bachelor of Surgery (MBBS) students at a private medical college in Udaipur, Rajasthan, India. Students were eligible if they provided informed consent. Given the exploratory nature of this study and the focus on a defined academic cohort, a formal sample size calculation was not conducted. All eligible and consenting final-year undergraduate medical students at the institution during the data collection period were invited to participate. Students who had previously participated in similar studies and those with any responses that were deemed incomplete were excluded. A total of 183 students participated in the study.
Data Collection Procedure
Participants were approached during scheduled academic sessions and provided with a self-administered, anonymous online questionnaire. The purpose of the study was explained, emphasizing voluntary participation and confidentiality. The Brief Sexual Attitudes Scale (BSAS) tool was digitized and distributed via a secure Google Form. Participants completed the form privately through a secure link. No personally identifying information was collected. All responses were anonymized and securely stored. Participation was voluntary, with the right to withdraw at any time. Participants were asked whether they had previously participated in a similar survey on sexual attitudes, to identify potential duplicate responses and minimize response bias.
Tools
Data were collected using a self-administered online questionnaire incorporating the BSAS, a validated 23-item tool that assesses four domains of sexual attitudes: Permissiveness, birth control, communion, and instrumentality. It demonstrates strong internal consistency, with Cronbach’s alpha values of 0.93, 0.84, 0.71, and 0.77, respectively. Construct validity was established via factor analysis, confirming a four-factor structure, indicating its reliability and validity in measuring sexual attitudes. 20 Each item was rated on a 5-point Likert scale (1 = strongly disagree to 5 = strongly agree). The BSAS was originally developed and validated by Hendrick et al. 20 It has also been used in Indian settings, supporting its cultural relevance and interpretability among Indian college students.21,22
Statistical Analysis
The data were entered into a Microsoft Excel spreadsheet, and statistical analysis was carried out using the Statistical Package for the Social Sciences version 16. Descriptive statistics (mean, standard deviation, frequency, and percentage) were used to summarize sociodemographic variables and BSAS subscale scores. BSAS subscale scores were treated as continuous variables, and between-group differences according to sociodemographic and behavioral characteristics were examined using independent-samples t tests. Correlations between BSAS subscales were analyzed using Pearson’s correlation coefficients. All tests were two-tailed with α = 0.05, and a P value of <.05 was considered statistically significant; analyses were considered exploratory, and no formal correction for multiple comparisons was applied.
Results
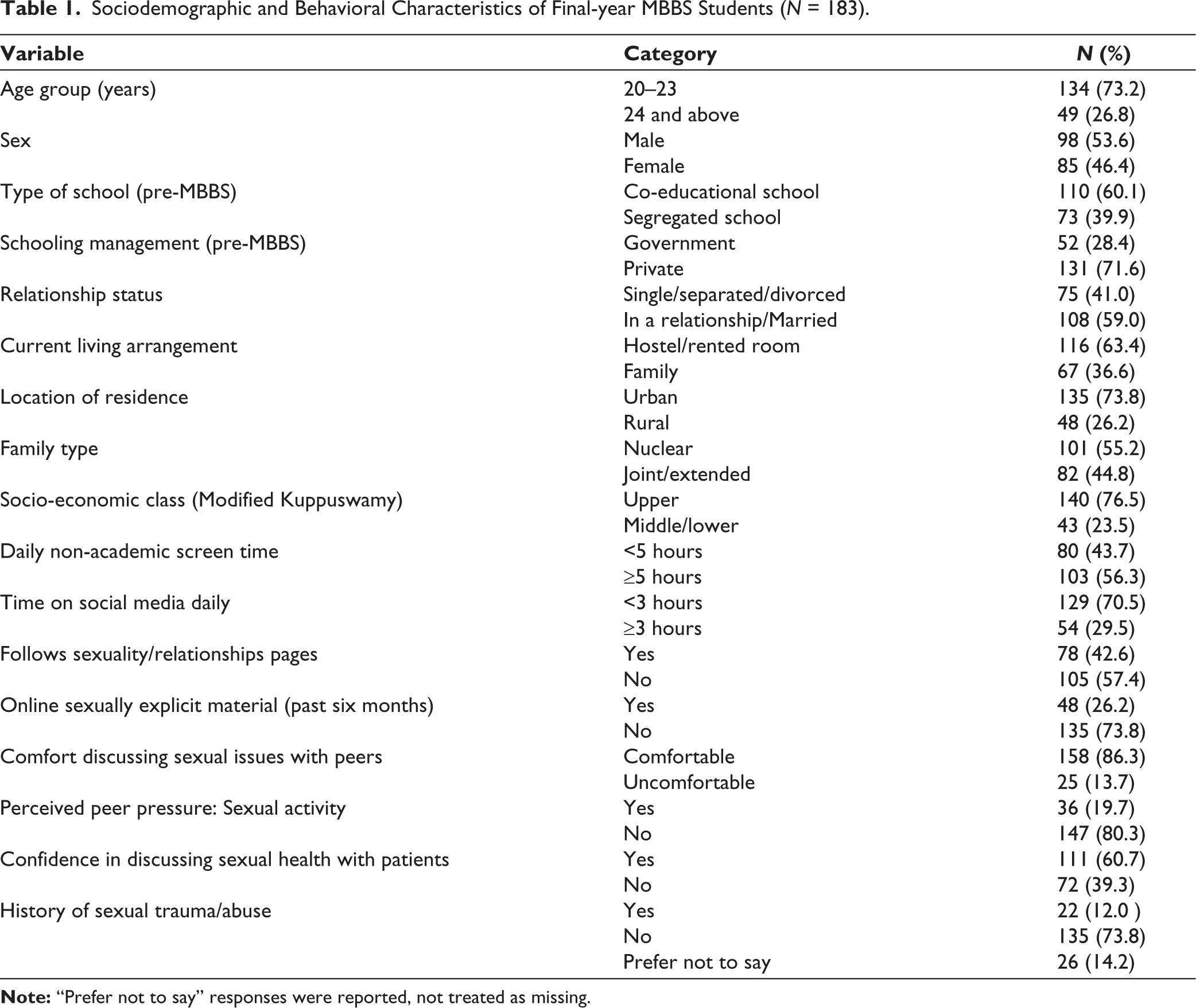
Table 1 shows that the majority of final-year medical students were aged 20–23 years (73.2%). A majority attended co-educational schools (60.1%). More than half of the participants (59.0%) were in a relationship or married. Most students resided in hostels or rented accommodations (63.4%). The majority were from urban areas (73.8%) and nuclear families (55.2%), with 76.5% belonging to the upper socioeconomic class. Additionally, 56.3% of students reported ≥5 hours of daily non-academic screen time, and 29.5% spent ≥3 hours daily on social media. About 42.6% followed sexuality or relationship-related content online, while 26.2% had viewed sexually explicit material in the past six months. A large majority (86.3%) felt comfortable discussing sexual issues with peers, 60.7% were confident discussing sexual health with patients, and 19.7% reported perceived peer pressure toward sexual activity.
Sociodemographic and Behavioral Characteristics of Final-year MBBS Students (N = 183).
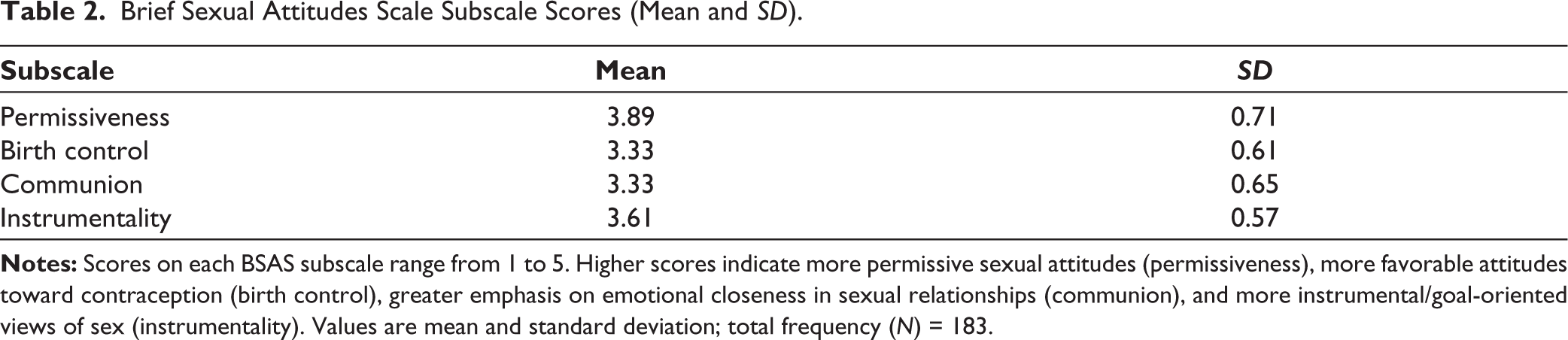
The highest BSAS subscale mean was observed for permissiveness (M = 3.89, SD = 0.71), followed by instrumentality (M = 3.61, SD = 0.57). Communion and birth control both recorded a mean of 3.33 (SD = 0.65 and 0.61, respectively) (Table 2).
Brief Sexual Attitudes Scale Subscale Scores (Mean and SD).
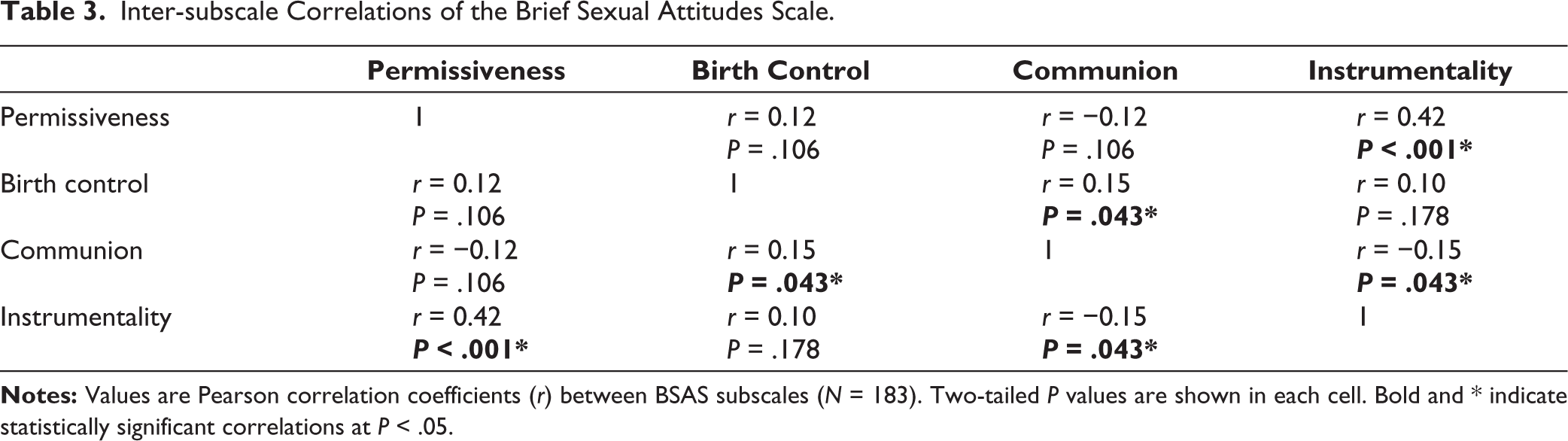
In Table 3, permissiveness showed a significant positive correlation with instrumentality (P < .001). Birth control was positively correlated with communion (P = .043), whereas communion was negatively correlated with instrumentality (P = .043).
Inter-subscale Correlations of the Brief Sexual Attitudes Scale.
For permissiveness, significantly higher scores were observed among students from co-educational schools compared to segregated schools (P = .021), those spending ≥3 hours on social media (P = .016), males (P = .038), and those who had viewed sexually explicit material (P = .004). Students who followed sexuality or relationship content online (P = .020) and those reporting peer pressure for sexual activity (P = .024) also exhibited greater permissiveness. For birth control, females and older age students scored significantly higher (P = .028 and P = .032, respectively). Regarding communion, higher scores were found among females (P = .014) and among those in relationships (P = .042). For instrumentality, students living independently scored higher (P = .023). Those who followed sexuality-related content online (P = .011), spent ≥3 hours daily on social media (P = .010), or had viewed sexually explicit content (P = .004) also reported significantly higher instrumental attitudes toward sex (Table 4).
Associations Between Sexual Attitudes (BSAS Subscales) and Key Sociodemographic and Behavioral Characteristics.
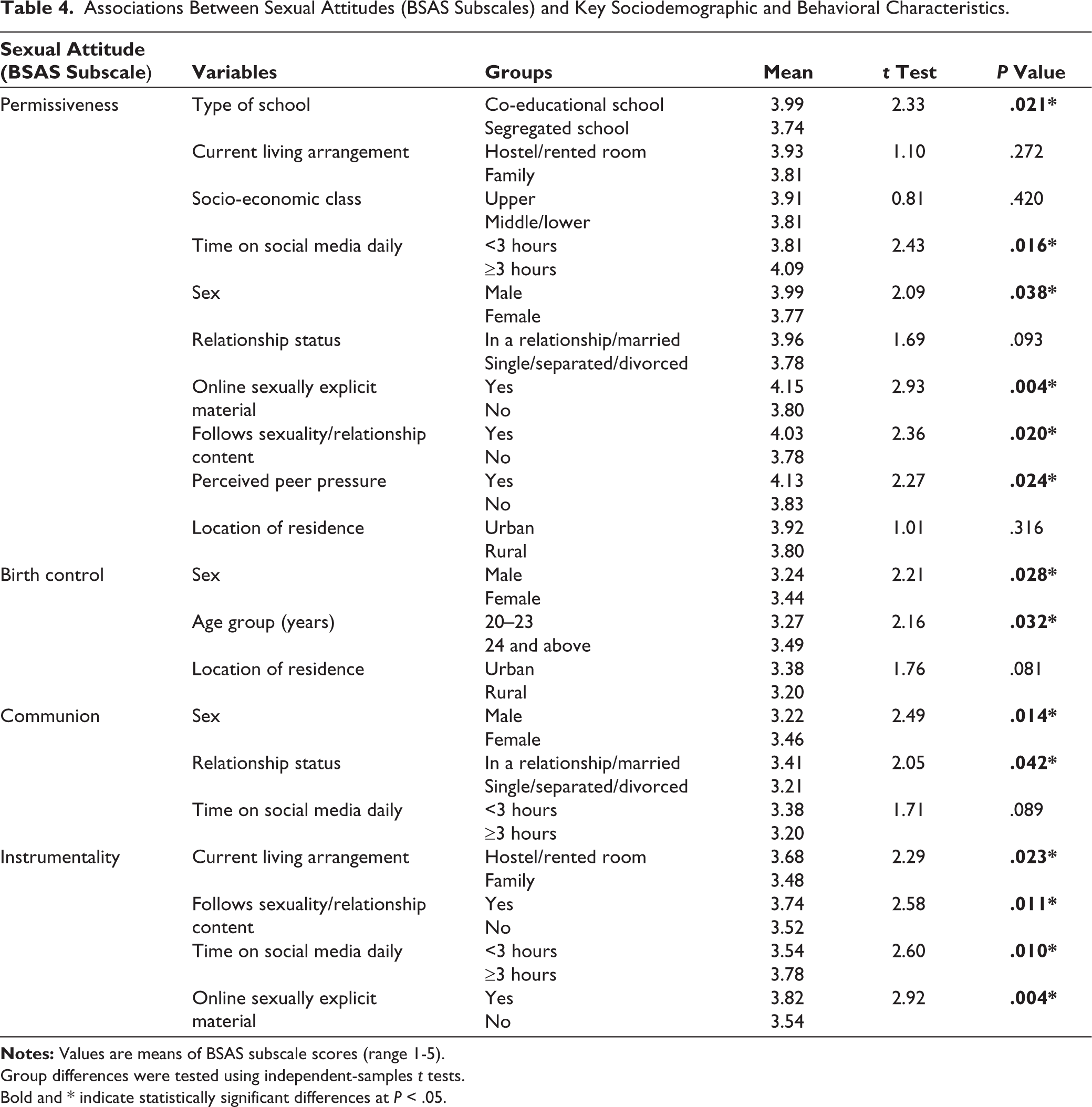
Group differences were tested using independent-samples t tests.
Bold and * indicate statistically significant differences at P < .05.
Discussion
In the present study, most students were younger adults with a male predominance, consistent with findings from Sharma et al. 13 A majority hailed from urban areas and nuclear families, similar to Nair et al. 16 who reported comparable trends among medical students. Most students were from co-educational and privately managed schools, similar to Shetty et al. 14 A majority resided away from their families, paralleling findings by Chhabra and Das, 15 indicating greater autonomy in living arrangements during clinical training. Regarding sexual openness, most participants felt comfortable discussing sexual issues with peers, yet fewer were confident discussing these with patients. This gap echoes Sharma et al. 13 who reported that only about half of final-year students felt professionally comfortable addressing sexual health concerns. Exposure to sexually explicit material was reported by fewer students than in other similar studies,10,11 likely reflecting sociocultural restraint in the Indian cohort.
Among the subdomains of the BSAS, permissiveness ranked highest, followed by instrumentality, indicating moderate liberal attitudes toward sexual freedom and self-oriented sexuality. These findings suggest slightly higher openness compared to previous cohorts studied by Sharma et al. 13 and Shetty et al. 14 pointing to gradual liberalization among newer generations of medical students. In contrast, birth control and communion domain scores were moderate, consistent with an Indian study 21 among Indian college students. These results also align with international literature on sexual and contraceptive attitudes.5,11 Instrumentality scores in this cohort were comparable with those found by a Mumbai-based study, 22 reflecting the emergence of pragmatic or self-focused sexual attitudes among medical students. Collectively, these patterns suggest that while sexual liberalization is increasing, emotional and relational dimensions remain moderated by prevailing sociocultural values.
Significant correlations in the present study were observed between permissiveness and instrumentality, consistent with Hendrick et al. 20 and Mansata et al. 21 who reported similar associations in both Western and Indian samples. The positive correlation between birth control and communion suggests that emotional intimacy aligns with responsible sexual behavior, paralleling findings by Reis et al. 5 Conversely, the negative correlation between communion and instrumentality supports the conceptual independence of emotional and pragmatic sexual domains, as also demonstrated by Hendrick et al. 20 These findings indicate that students displaying more liberal sexual attitudes also exhibit higher sexual autonomy and pragmatic orientation, yet emotional connection remains somewhat distinct from utilitarian sexual expression, a consistent pattern across diverse cultural contexts.
Higher permissiveness was observed among students from co-educational schools, males, those spending more time on social media, those exposed to sexually explicit content, and those following sexuality-related content online. Similar gender effects were reported by Sharma et al. 13 and AlQuaiz et al. 17 where male students exhibited more liberal attitudes. Increased permissiveness among those exposed to sexual media parallels findings by Zahedi et al. 10 who found exposure significantly associated with permissive views. Higher birth control scores were noted among females and older students, reflecting greater contraceptive awareness and responsibility. Comparable findings were observed in Reis et al. 5 and Nosheen et al. 11 where females consistently demonstrated stronger attitudes toward responsible sexual behavior. Females and students in relationships scored higher in communion, indicating stronger emotional and relational orientation. Similar trends were identified by Shetty et al. 14 and Nosheen et al. 11 suggesting that women and partnered individuals place greater emphasis on emotional intimacy within sexual relationships. Instrumentality was higher among students living independently, those following sexuality-related content, spending more time on social media, and those exposed to explicit material. Comparable trends were found in AlQuaiz et al. 17 and Zahedi et al. 10 where greater media exposure and independent living correlated with more pragmatic or exploratory sexual attitudes.
Overall, this study demonstrates that Indian final-year medical students exhibit a nuanced pattern of sexual attitudes, characterized by increasing liberalization in permissiveness and instrumentality, alongside moderate conservatism in birth control and communion. The significant gender and behavioral associations align with both Indian13-16,21,22 and global literature,5,10,11,17 reflecting a shift toward balanced sexual liberalism within professional student populations. Despite improved openness, gaps persist in emotional and communicative aspects of sexuality, emphasizing the need for structured, culturally sensitive sexual health education within medical curricula.
Strengths and Limitations
The strength of this study lies in its use of a validated and culturally adapted tool, the BSAS, to comprehensively assess multiple domains of sexual attitudes among final-year medical students, a group nearing professional practice. The inclusion of diverse sociodemographic and behavioral variables enabled multidimensional analysis, while adequate sample size and anonymized data collection reduced response and social desirability biases. However, being a cross-sectional study conducted at a single private medical institution, the findings may not be generalizable to all medical students across India. The reliance on self-reported data also introduces the potential for underreporting or overreporting of sensitive behaviors. Future multicentric studies incorporating qualitative insights could provide a deeper understanding of the cultural and educational determinants shaping sexual attitudes among medical trainees.
Conclusion
This study highlights that final-year medical students demonstrate a progressive yet contextually balanced approach to sexuality. The highest attitudes were observed in the permissiveness and instrumentality domains of the BSAS, reflecting a growing liberal orientation toward sexual openness and autonomy. However, relatively moderate scores in birth control and communion indicate persisting conservatism in emotional and relational aspects of sexuality. Sociodemographic and behavioral factors significantly shaped these attitudes. Males and students from co-educational schools exhibited more permissive attitudes, while students with greater social media exposure or engagement with sexually explicit material showed more permissive and more instrumental perspectives. Conversely, females and students in relationships scored higher on communion and birth control subscales, suggesting a stronger emphasis on responsibility and intimacy. These findings indicate that while modernization and digital influence are broadening sexual liberalism among medical students, underlying cultural and relational values continue to moderate these shifts. Overall, the results underscore the importance of incorporating structured, evidence-based, and culturally sensitive sexual health education into the medical curriculum. Such integration would not only improve students’ professional comfort in discussing sexual health with patients but also foster informed, non-judgmental, and ethically grounded medical practice.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Before conducting the study, approval from Human Research Ethics Commitee (HREC) was taken. (GU/HREC/EC/2025/2733).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
The participants provided their written informed consent to participate in this study.