
Abstract
BACKGROUND:
Sexual health is a taboo issue in some societies. Limited assessments were conducted during nursing care in mental health services. It is unknown whether psychiatric nurses’ competencies would be enhanced through short training courses.
AIMS:
The present study employed a quasi-experimental design to evaluate the effectiveness of an 8-hour sexual health care training for psychiatric nurses to improve sexual health knowledge, attitude, and self-efficacy in a teaching psychiatric hospital in southern Taiwan.
METHOD:
Volunteered psychiatric nurses were randomly assigned to the experimental or control group. The 8-hour training program contained sexual health knowledge and attitudes, case discussion, role play, and sexual identity or harassment issues. Each nurse received a pretest and a posttest in the 1-month period between August and September 2019. Descriptive and multivariate statistical analyses were used to evaluate the effects.
RESULTS:
Among the 75 psychiatric nurses, 43 were in the control group and 32 were in the experimental group. The two groups were not significantly different in the working year, gender, education, marriage, and other psychosocial variables. After the training, the overall performance of sexual health care knowledge, attitudes, and self-efficacy of the experimental group improved significantly than the controls.
CONCLUSIONS:
The sexual health care training program enhanced psychiatric nurses’ confidence and generally improved their sexual knowledge and attitudes. It is suggested that sexual health care needs to be highlighted during in-job training to augment the well-being and life quality of psychiatric patients.
Introduction
Sexual health is an essential part of human development and personal rights. It is fundamental to physical and mental well-being as well as interpersonal relationships. Due to its complicated and sensitive features, sexual health issues require positive and respectful attitudes to achieve a pleasurable and safe experience (Hendry et al., 2018; World Health Organization [WHO], 2015). To promote sexual wellness, health care providers should make efforts to gain sexual health and well-being from the acquisition of sexual information and knowledge (WHO, 2015). Nurses are in a unique position and firm foundation to offer holistic care, which facilitates interactive discussions on sexuality and sexual health–related issues as a part of their daily practice (Quinn et al., 2013).
Severe mental illness and psychotropic medications could cause sexual dysfunction and dissatisfaction about sexual life (Montejo et al., 2018). The literature revealed that patients with mental disorders were more likely to become involved in high-risk sexual behaviors (e.g., infrequent condom use, trading sex for material gain, sex with the high-risk group), more vulnerable to sexual exploitation, and comorbid drug and alcohol abuse (Quinn & Browne, 2009). Although psychiatric patients find communication barriers in expressing sexual concerns, these issues tend to be underreported and underrecognized by mental health professionals in clinical settings (Bossini et al., 2014; Montejo et al., 2018). Health care providers may hold the belief that patients with disabilities should not have a sexual or reproductive life or need sexual health services (WHO, 2015). In contrast to such belief, a balanced sexual life could improve overall well-being, restore confidence and dignity, and further help overcome psychiatric patients’ stigma and integrate social activities (Montejo et al., 2018). A qualitative study showed that mental health nurses acknowledged the importance of sexuality in clinical practice, yet the majority avoided or ignored to mention these issues actively during their assessment or referred them to the psychiatrists (Quinn et al., 2011). However, two thirds of patients who experienced sexual dysfunction have never been asked about sexual functioning by their psychiatrists (Ucok et al., 2008).
Moreover, several reasons related to the infrequent practice of sexual health assessment in mental health nursing care were identified, such as lacking sexual knowledge, insufficient time, not considering it as the nursing role to discuss sexuality, difficulty opening the conversation, or anxious feelings between the nurses and patients during a discussion (Aaberg, 2016; Hendry et al., 2018; Quinn et al., 2018). Although integrated sexual health care is part of the nursing process, standardized sexual health training is lacking. In addition, there is taboo about sex-related issues in certain cultures such as the Taiwanese society, in which the majority avoid talking about it openly (Huang et al., 2020; T. Y. Tsai et al., 2011). Despite the importance of sexual health needs among psychiatric patients, evidence reveals that nurses are not providing adequate sexual information to them. Previous studies in Taiwan have shown that while most nurses and nursing students acknowledged their roles in providing sexual health care, they were unwilling to open the conversation in practice (L. Y. Tsai et al., 2013). Moreover, nurses identified the knowledge and gaps required to discomfiture when confronting patients’ sexual concerns and preventing them from performing sexuality assessments in clinical practice (Sung et al., 2016). These factors may interfere with the ability to offer proper nursing assessment and interventions toward patients in need of maintaining sexual health.
Therefore, to support psychiatric patients achieve equitable and quality lives, promoting the nurses’ competencies of sexual health care through training is of ultimate importance yet a challenge to many nursing educators (Ciydem et al., 2020). Researchers have indicated that the development of knowledge, competence, and self-confidence through sexual health care education can lead to improvement of self-efficacy and would have a positive effect on the attitudes toward sexuality discussions by the nursing students (Sung & Lin, 2013). A recent review from 1997 to 2017 showed only seven studies related to research examining the sexual health training program given to mental health nurses, of which six were conducted by the same authors in Australia and one in Ireland (Hendry et al., 2018). The findings showed a lack of robust evidence to inform the current gap of knowledge. Therefore, more research will be needed to explore the outcomes of sexual health training programs to help mental health nurses equip with better skills in consulting sexual health issues, especially in Asian societies. This quasi-experimental study aimed to evaluate the effectiveness of a sexual health care training program for psychiatric nurses in a teaching hospital in southern Taiwan. We hypothesized that psychiatric nurses who received an 8-hour sexual health training in this study would report significantly higher levels of knowledge, attitude, and self-efficacy in sexual health care.
Method
The Design and Study Population
The research was designed as a quasi-experimental, pre- and posttest study to evaluate the effectiveness of a sexual health care training program for psychiatric nurses in terms of their knowledge, attitude, and confidence in assessing and discussing these issues with patients. The study was conducted in the largest psychiatric teaching hospital in southern Taiwan from August to September 2019. The research sample consisted of psychiatric nurses who volunteered to participate in the research and be able to share experience in the group. The nurses who volunteered were allocated to the control (n = 43) or experimental group (n = 32) according to time differences during the study period; thus, the sample size was slightly different. The experimental group received an 8-hour sexual health care training program, and the control group did not undertake any course.
The first two authors explained the research purpose and procedure to the participants in both groups during recruitment. The two groups’ baseline data were collected through a standardized questionnaire. Each participant took around 20 to 30 minutes to complete the pretest tests using the questionnaire. Then the participants in the experimental group completed the 8-hour training course. The posttest was collected right after the training course for both groups.
Sexual Health Care Training
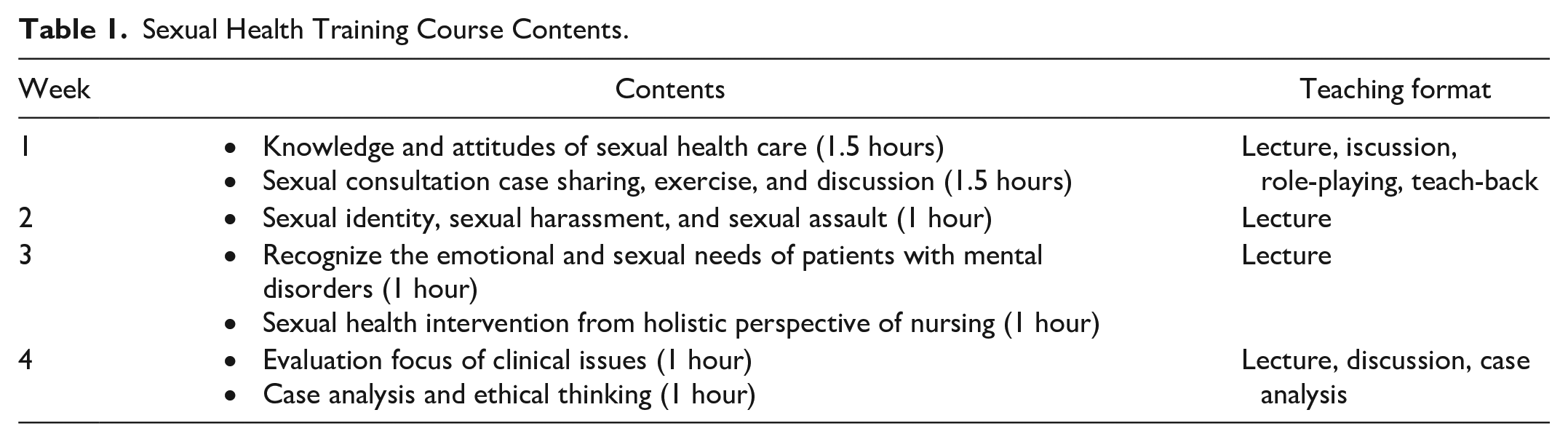
The 8-hour sexual health care training program was conceptually derived from the theoretical basis developed by Sung et al. (2016). The total time for the training course was 8 hours within 4 consecutive weeks. Each week contained one to two sessions, with each session lasting for 60 to 90 minutes (Table 1). The course included three themes. The first theme was to develop the concepts of sexual health care. The second theme focused on sexual consultation, case analysis, role-playing exercises, and discussion. The last theme was to emphasize sexual identity, sexual harassment, and sexual assault related to mental health clinical practices. The teaching formats included lectures, clinical role-playing scenarios, teach-back method, in-depth case analysis, and interactive discussion in large or small groups.
Sexual Health Training Course Contents.
Instruments
The questionnaire was composed of demographic information and three parts of sexual health–related questions, including sexual health care knowledge, sexual health care attitude, and self-efficacy scales in assessing and discussing sexual health issues (Sung & Lin, 2013). The original scale was approved to adopt in this study (Sung & Lin, 2013).
Demographic information: This part of the assessment includes gender, age, education level, religious beliefs, years of work, marital status, family type, relationship with parents, previous experience of taking related courses about sexual health, and experience of being sexually harassed in clinical care.
Sexual Health Care Knowledge Scale: The scale entails three parts of questions, including sexual health care, sexual health care evaluation, and sexual harassment or assault, with a total of 31 items. Each item was rated as “yes,” “no,” or “do not know.” The correct answer was rated 1 point, while 0 points for the wrong answer or don’t know. The higher the score, the higher the levels of knowledge related to sexual health care. The content validity index (CVI) score was .83, and the test–retest reliability was satisfactory (Cronbach’s α = .73; Sung & Lin, 2013). In this study, the Cronbach’s alpha score was .91.
Sexual Health Care Attitudes Scale: The scale covers three aspects of assessment, including “independence,” “professional roles,” and “professional response,” with a total of 18 questions. Each question was rated on the 5-point Likert-type scale and divided into 5 = strongly agree, 4 = agree, 3 = neutral opinions, 2 = disagree, and 1 = strongly disagree. The score ranges from 18 to 90. The higher the score, the more positive attitudes the nurses possess in dealing with sexual health care issues or holding a more positive attitude toward professional roles and professional response. The test–retest reliability was high (Cronbach’s α = .91), with the CVI score of .96 (Sung & Lin, 2013). The Cronbach’s alpha in this study was .96.
Sexual Health Care Self-Efficacy Scale: The 22 items in the scale were divided into three dimensions—that is, “communicative issues related to self-efficacy,” “self-efficacy toward professional response,” and “responsive issues of self-efficacy.” Each question was measured with the 5-point Likert-type scale, reflecting the degree of self-efficacy—that is, 5 = >90%, 4 = 70% to 80%, 3 = 50% to 60%, 2 = 30% to 40%, and 1 > 20%. The total score ranges from 22 to 110 points, with a higher score indicating a higher level of confidence in dealing with sexual health care. The CVI and test–retest reliability were both high (Cronbach’s α = .94, CVI = .92; Sung & Lin, 2013). The Cronbach’s alpha in this study was .98.
Ethical Considerations
The ethical approval was received from the hospital’s institutional ethics committee where the study was conducted (reference number: KSPH-2019-10). The psychiatric nurses were informed about the research, and their written informed consent was obtained. Participation was voluntary, and the participants were able to withdraw from the research at any time, which would be kept confidential during and after the research.
Data Analysis
The Statistical Package for Social Sciences (SPSS) Version 21.0 (SPSS Inc., Chicago, IL, USA) for Windows was used. To analyze the psychiatric nurses’ descriptive characteristics, numbers, percentages, and arithmetic means were used. Itemized responses of the knowledge, attitudes, and self-efficacy in the scales were analyzed to provide evidence-based results to inform clinical training course development. The independent-sample t test (t table value) and chi-square were used to compare two independent normally distributed groups and access the association between categorical variables. The paired-samples t test (t table value) was used to compare the two dependent groups. The statistical power was set at .05.
Results
Seventy-five psychiatric nurses voluntarily participated in this study, with 32 nurses in the experimental group and 43 nurses in the control group. No significant differences were found in most demographic variables between the two groups except the mean age (p < .001). More than half of the nurses had more than 5 years of working experience in both groups, and about 81% of nurses had taken a basic course about sexual health before the study. Concerning sexual harassment issues, prior experience in sexual harassment in general and sexual harassment in the hospital by the patients were assessed. The number of nurses in the experimental group who reported having experienced sexual harassment in general was slightly less than those who did in the control group (43.8% and 53.5%, respectively); however, the two groups had the same prevalence of having experienced sexual harassment in the hospital by the patients (53%). While half of the nurses in the experimental group reported their feeling of trouble during taking care of the patients with sexual health issues, only one third of the control revealed that feeling (Table 2).
Participant Characteristics of the Two Groups at Baseline.

Table 3 illustrates the mean score of perceived knowledge, attitude, and self-efficacy before and after the training and also shows the mean differences (MD) of pre- and postscores among the two groups. At baseline, all participants exhibited a similar level of sexual health care knowledge (experimental group = 23.21 ± 3.64, control group = 22.49 ± 4.29, score range = 0-31). Psychiatric nurses who completed the sexual health care training program had significantly higher scores on knowledge (MD = −1.53, 95% confidence interval [CI; −1.96, −1.10], p < .001), attitude (MD = 0.37, 95% CI [0.08, 0.66], p = .02), and self-efficacy (MD = 0.71, 95% CI [0.22, 1.16], p < .001). Nevertheless, there was a significant slight decrease in the control group’s knowledge mean score from 22.49 (SD = 4.29) to 21.58 (SD = 6.74) (MD = 0.91, 95% CI [0.04, 1.77], p = .04), and no difference was recorded in the domain of attitude and self-efficacy within this group.
Perceived Knowledge, Attitude, and Self-Efficacy Pre- and Posttraining.
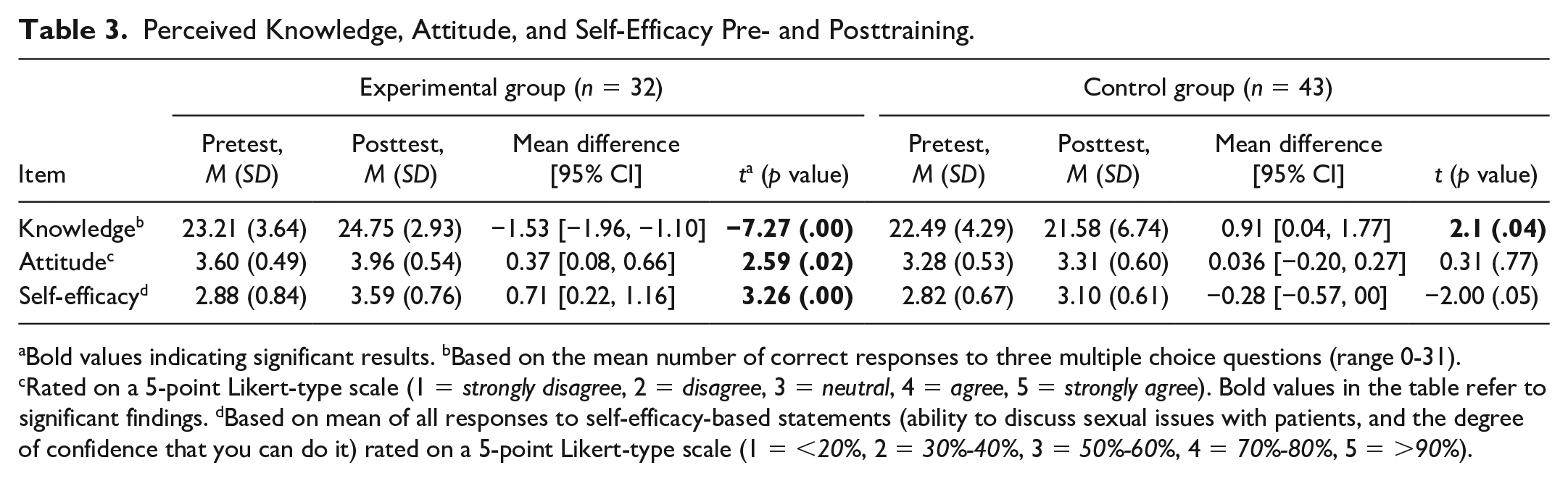
Bold values indicating significant results. bBased on the mean number of correct responses to three multiple choice questions (range 0-31). cRated on a 5-point Likert-type scale (1 = strongly disagree, 2 = disagree, 3 = neutral, 4 = agree, 5 = strongly agree). Bold values in the table refer to significant findings. dBased on mean of all responses to self-efficacy-based statements (ability to discuss sexual issues with patients, and the degree of confidence that you can do it) rated on a 5-point Likert-type scale (1 = <20%, 2 = 30%-40%, 3 = 50%-60%, 4 = 70%-80%, 5 = >90%).
According to the knowledge domain, all participants exhibited high overall correct responses on the knowledge related to sexual health care at baseline. The significant differences were recorded between the experimental group and the control group (p < .05) related to early ejaculation in men, urethral reflux complication in sex reassignment surgery from female to male, avoidant terms in discussing sexual issues, describing the sexual problem with a generalized or normalized manner, and religious/cultural taboos’ effect on patient’s sexuality expression. After the sexual health care training program, participants in the experimental group significantly increased their correct response items (p < .05) concerning vaginal dryness, myocardial infarction, the manner of describing the sexual problem, low libido after childbirth, religious and cultural taboos’ effect in sexuality expression, and verbal sexual harassment identification (Table 4).
Percentage of Correct Responses on the Knowledge Related to Sexual Health Care Pre- and Posttraining Among the Two Groups.
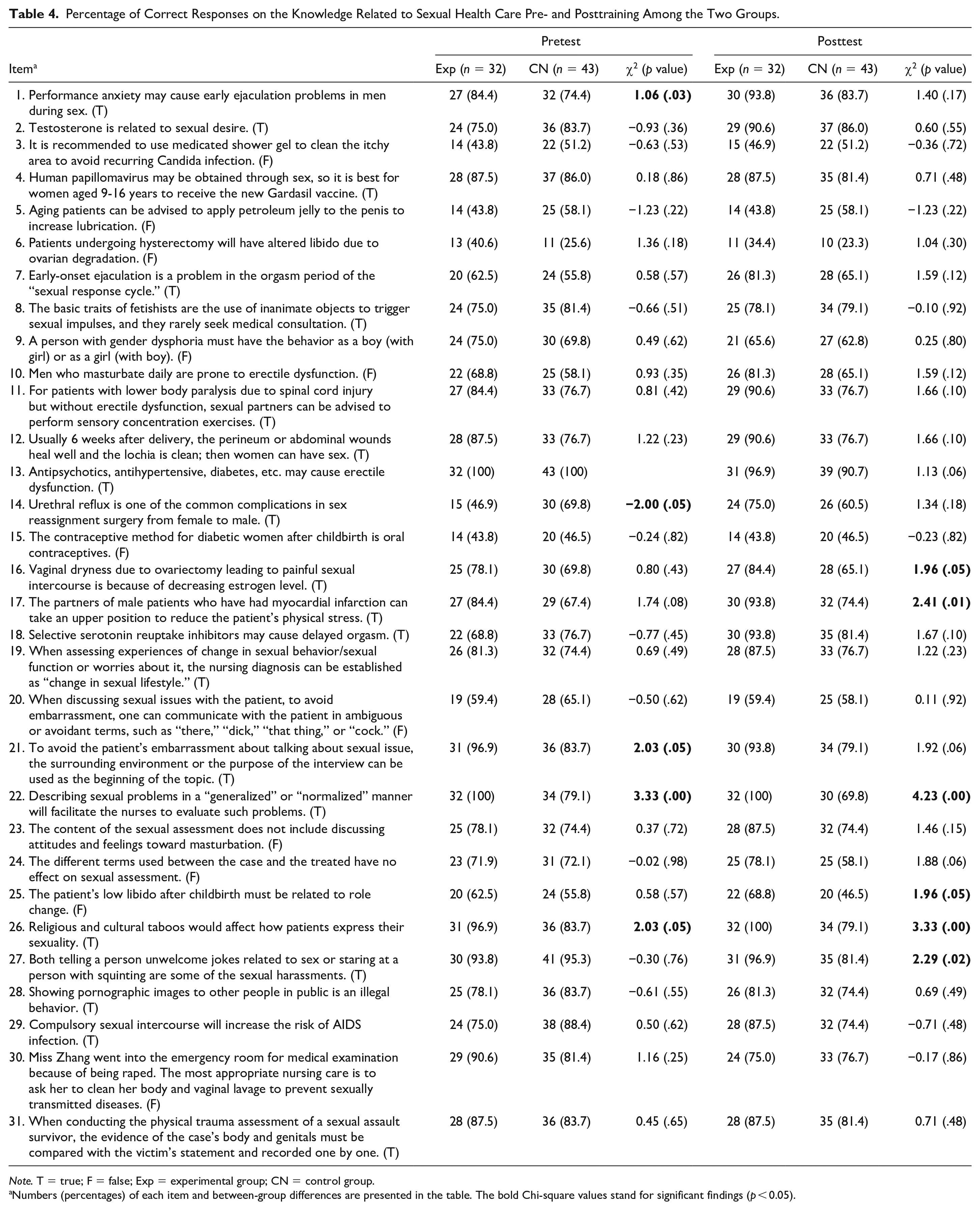
Note. T = true; F = false; Exp = experimental group; CN = control group.
Numbers (percentages) of each item and between-group differences are presented in the table. The bold Chi-square values stand for significant findings (p < 0.05).
Table 5 shows the agreeableness level on the attitude related to sexual health care pre- and posttraining among the two groups. The number of participants who answered “strongly agree” or “agree” would be categorized as agreeableness level to perform in Table 5. The attitude related to the sexual health care domain included three subscales related to feeling comfortable, feeling responsible, and feeling suitable in providing care for patients with sexual health problems. Notably, all psychiatric nurses in the experimental group reported significant improvement in nearly all items assessing sexual health care attitude. In contrast, the control group still kept a negative attitude pre- and posttraining. Psychiatric nurses in the control group reported the lowest agreeableness attitude scores related to feeling comfortable if the patient asks about their sexual problems (n = 10, 23.3%), assess (n = 11, 25.6%), or discuss (n = 12, 27.9%) sexual problems with the patient; feeling responsible to actively assess patient sexual health problems (n = 12, 27.9%); feeling suitable to be the first line to discuss with the patient about their sexual issues (n = 11, 25.6%).
The Agreeableness Levels on the Attitude Related to Sexual Health Care Pre- and Posttraining Among the Two Groups.
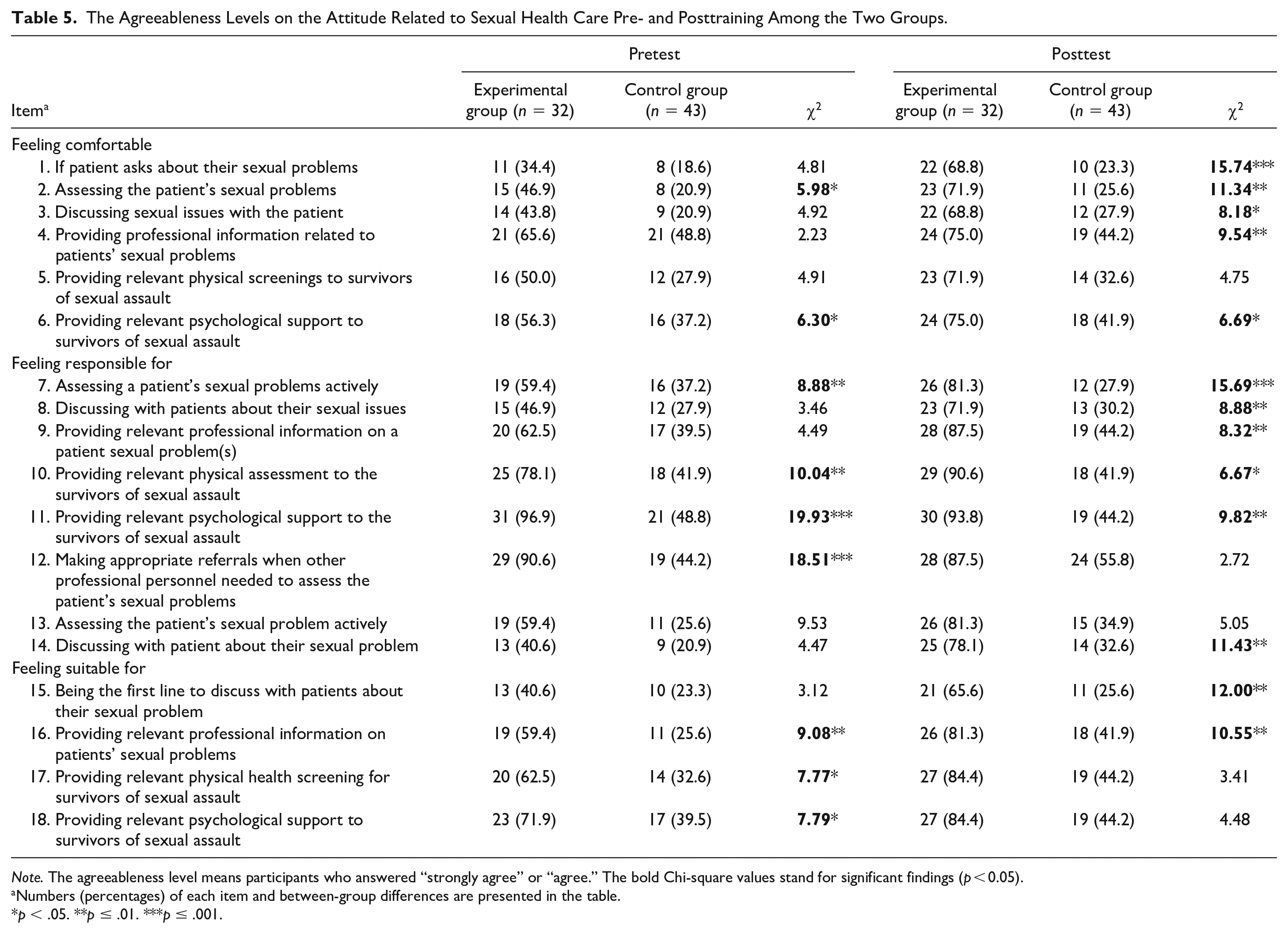
Note. The agreeableness level means participants who answered “strongly agree” or “agree.” The bold Chi-square values stand for significant findings (p < 0.05).
Numbers (percentages) of each item and between-group differences are presented in the table.
p < .05. **p ≤ .01. ***p ≤ .001.
At baseline, all psychiatric nurses reported low confidence in providing sexual health care. The lowest confidence scores related to encouraging others to discuss sexual problems (experimental group: 2.47 ± 0.98; control group: 2.72 ± 0.83), assessing the patients’ sexual and physical problems (experimental group: 2.50 ± 0.95; control group: 2.65 ± 0.75), and discussing sexual relevant physical issues (experimental group: 2.50 ± 0.98; control group: 2.67 ± 0.81). The psychiatric nurses report the most confidence in adapting and seeking help for their psychological discomfort caused by sexual harassment (experimental group: 3.25 ± 0.98; control group: 2.93 ± 0.86). After completing the training, psychiatric nurses in the experimental group significantly improved self-efficacy in providing care, performing assessments, and discussing sexual health issues for all categories compared with the control group with a mean score from 3.22 ± 0.98 to 3.84 ± 0.81. In contrast, the control group still felt less confident in providing sexual health care for the patient with the lowest score concerning provide relevant professional sexuality information based on the physical problems (2.86 ± 0.71), and assess the patients’ sexual and psychological problems (2.88 ± 0.73; Table 6).
The Self-Efficacy of Discussing Sexual Health Issues With Patients Pre- and Posttraining Among the Two Groups.
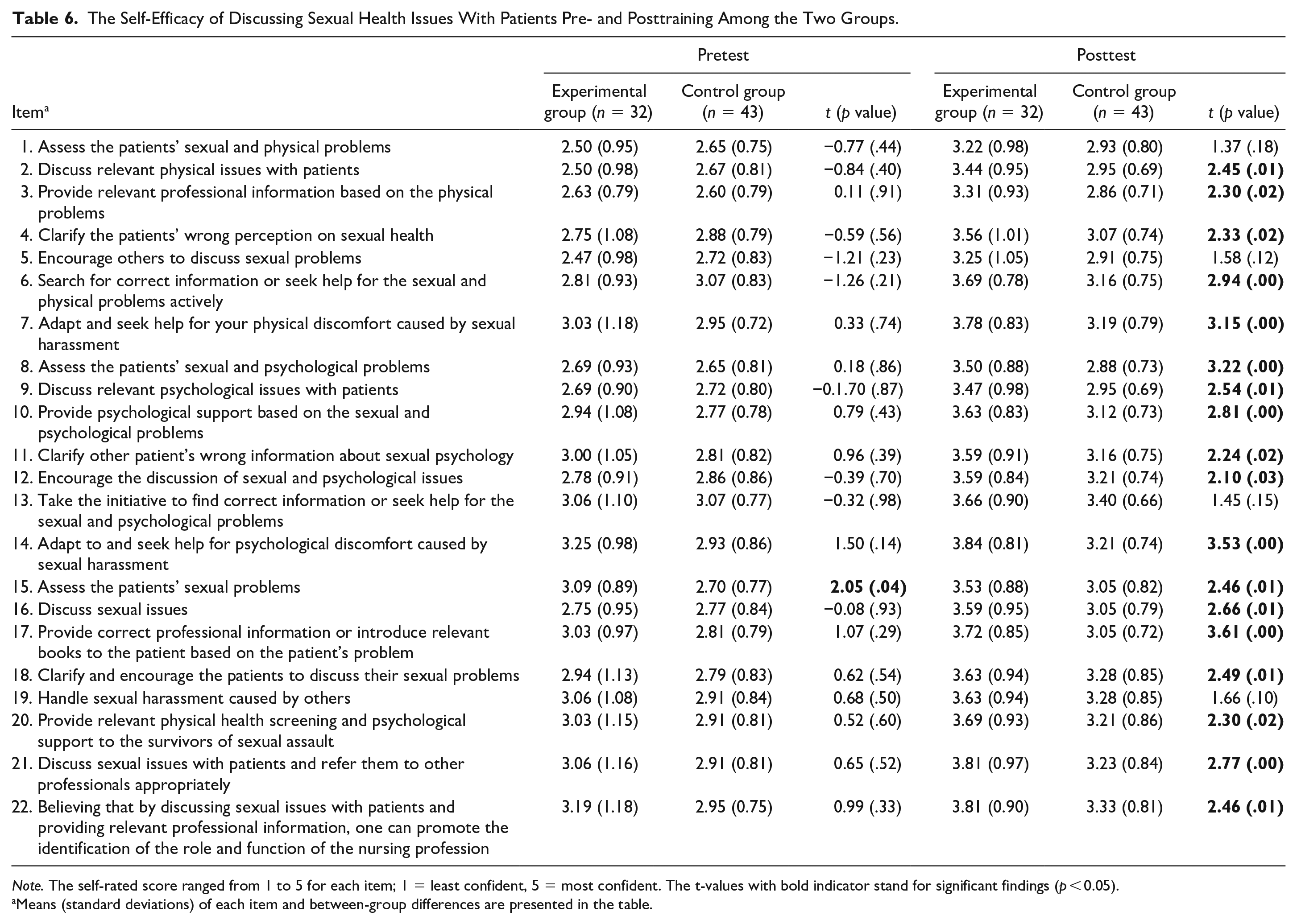
Note. The self-rated score ranged from 1 to 5 for each item; 1 = least confident, 5 = most confident. The t-values with bold indicator stand for significant findings (p < 0.05).
Means (standard deviations) of each item and between-group differences are presented in the table.
Discussion
Both the experimental and control groups had high overall knowledge scores at baseline, suggesting that the participating psychiatric nurses have received similarly appropriate background knowledge in sexual health care. The findings suggested that psychiatric nurses who completed the 8-hour sexual health training program had significant improvement in their knowledge, attitude, and self-efficacy compared with the control group. These results deserved more attention in nursing education and in-job training for mental health nurses because they require not only knowledge but also positive attitudes and competence to provide sexual health care.
The underlying study detected similar levels of knowledge on sexual health care in both groups before the training program except for a few areas of questions, indicating comparable background knowledge levels for the participating nurses. While the experimental group showed significant improvement in knowledge scores, the control group reported a decline after the training program. This result showed the effectiveness of a concise sexual health care program in the clinical setting for psychiatric nurses. Thus, psychiatric nurse educators should be mindful to include a diverse range of topics in sexual health curricula (including sexual health–related specific clinical problems, the manner of describing sexual health, religious and cultural taboos, and sexual harassment identification).
A previous study supported the fact that discomfort feelings experienced by the psychiatric nurses in responding to the patients’ sexual concerns and discussing sexual problems may derive from inadequate knowledge about sexuality (Tugut & Golbasi, 2017). Psychiatric nurses in the experimental group of this study reported significantly more improvement in the agreeableness levels on the attitude (i.e., feeling comfortable, feeling responsible, and feeling suitable) of providing care for psychiatric patients with sexual health problems. Of note, almost all items assessing the attitude of psychiatric nurses in the experimental group improved significantly following their attendance of the program. Evidence showed the consistency that demonstrated the increasingly positive attitude toward sexual health care by providing education (Haesler et al., 2016; Sung et al., 2016). In contrast, the control group reported the most negative attitude scores in the following four items: feeling comfortable facing patients’ sexual health concerns, assessing and discussing sexual problems with the patient, responsibility in assessing patient sexual health problems, and suitability in discussing as the first line to the patient about their sexual issues. Similarly, another study pointed out the reason why nurses hesitate to talk about sexual health issues (Saunamäki & Engström, 2014). While most nurses felt responsible, the sexual health topic triggered embarrassing feelings, which put an end to a conversation about sexuality. Also, attitudes about patients’ sexuality concerns are dominated by personal values rather than professional values in the psychiatric clinical care context (Ruane & Hayter, 2008). Therefore, to identify patients’ sexual problems, the psychiatric nurses should use their knowledge and go beyond the comfort zone to address sexuality (Saunamäki & Engström, 2014).
On completing the sexual health care training, the experimental group reported significant improvements in self-efficacy scores in sexual health care for all categories compared with the control group. These results were consistent with recent studies conducted in Taiwan (Sung & Lin, 2013), Turkey (Tugut & Golbasi, 2017), and America (White et al., 2020), which showed improvements in self-efficacy after sexual health care training in nursing students and registered nurses. Another study suggested that sexual issues in clinical practice presented nurses with considerably difficult ethical, legal, judgmental, and professional challenges while affecting their self-efficacy of actual care (Sung et al., 2016). Therefore, helping to improve the self-efficacy of the nurses is an important task in the mental health field. In addition to increasing the nurses’ self-efficacy in dealing with sexual health problems and emphasizing the importance of maintaining professional knowledge in in-job training, nursing educators can offer actual cases to discuss and assist the nurses to have a better conversation to support the patients’ well-being and recovery (Quinn & Browne, 2009), and this evidence was supported by the underlying study.
Overall, on completion of the training program, psychiatric nurses in the experimental group reported significantly higher levels of knowledge, attitude, and self-efficacy in providing comprehensive sexual health care for patients with mental illness. Our result was inconsistent with another local study, in which the sexual health care training was provided to nurses (70% psychiatric nurses and 30% general nurses) and showed a nonsignificant result in their self-efficacy (Sung et al., 2016). However, our results were similar to studies of nursing students that led to significant improvement in sexual health care knowledge, attitude, and self-efficacy (Sung & Lin, 2013; Tugut & Golbasi, 2017). This discrepancy could have occurred because individuals’ self-efficacy may change within relatively short periods and clinical practice environments (Bandura, 1997; Sung & Lin, 2013). On the other hand, research on social cognitive theory showed that intraindividual changes in self-efficacy related to the study engagement and task performance over time (Ouweneel et al., 2013). Therefore, to improve psychiatric nurse’s confidence more effectively, sufficient training time and proper instructions should be directed for clinical nurses in future sexual health care programs (Hendry et al., 2018; Sung et al., 2016).
Current research about such training for psychiatric nurses had been scarce and underrecognized, which could lead to underestimation of the patients’ need for sexual health. A previous study suggested that psychiatric nurses recognize the necessity of sexual health assessment, but the majority of nurses do not properly offer such care or receive appropriate education, support, or consultation about management or treatment for the patients’ sexual problems (Higgins et al., 2006a, 2006b). On the contrary, if the nurses understand their attitudes concerning human sexuality, biases may reduce with motivation to communicate sexual health issues enhanced (McCann, 2003; Quinn & Browne, 2009). Our course contents were designed to recognize the emotional and sexual needs of psychiatric patients, especially the holistic nursing care perspective. Compared with other diseases, severe mental disorders and psychotic medications impair sexual function and reduce the sexual satisfaction of psychiatric patients. As a result, patients with mental illness are needed to be screened not only for potential sexual dysfunction but also for sexual needs (Montejo et al., 2018). The findings align with previous reports of psychiatric nurses’ needs to actively develop and perform sexual health assessment in daily practice for a better quality of life among psychiatric patients (Ding et al., 2016; Montejo et al., 2018; Quinn & Browne, 2009; Quinn et al., 2018). Last but not the least, about a half of our respondents reported having previous experience of sexual harassment both in general and in the hospital by the patients. This situation may lead to effects on nurses’ psychological distress and attitude toward psychiatric care, which directly affect on providing holistic care to the best of their ability (Yada et al., 2014). In the current study, a 1-hour course was designed in the training course to assist the psychiatric nurses to identify sexual harassment and sexual assault to reduce the occurrence of sexual harassment. Through enhancing psychiatric nurses’ attitude and self-efficacy in delivering sexual health care using a guideline or supportive program, the importance and effectiveness of sexual harassment identification and management were evident and need to be valued in psychiatric clinical practice.
Our study presents a unique evidence into the sexual health care training program for Taiwanese psychiatric nurses and further supports finding from a rare study field that the sexual health care training enhanced psychiatric nurses’ confidence and improved their sexual knowledge and attitudes (Hendry et al., 2018). Moreover, the concise program was constructed within 8 hours that applied to reasonable numbers of participants in the clinical setting. We presented detailed findings of each item in the scale to understand the impact of the 8-hour training program, which will inform future training development to enhance the nurses’ knowledge, attitude, and self-efficacy in sexual health care. We believe that these specific findings will bring much attention to the nursing leaders who want to create and tailor an appropriate program for their needs in a different context. Moreover, the itemized contents will help psychiatric nurses to learn, thus we presented these results in detail. However, several limitations should be acknowledged. First, our study was conducted in only one hospital with female dominance. It is not possible to generalize these findings to a broader population or represent the views of mental health nurses elsewhere. Furthermore, to avoid information contamination and to broaden sample size, multisite training can be conducted across hospitals to increase power. Second, the sexual health care training program leads to permissive knowledge, attitudes, and self-efficacy immediately posteducation, but the sustainability of change over time was not explored. Therefore, further research is needed to investigate this important issue. Finally, although the mean age difference between groups resulted from the volunteering process of participation, it may potentially affect the outcomes. The senior psychiatric nurses might have more experiences and knowledge that would lead to a better attitude and self-efficacy of sexual health. Future studies are suggested to apply age-matched randomizing method with more sample size and observe longer-term effectiveness for further evidence.
Conclusion
The study found that the underlying sexual health care training had a positive effect on the knowledge, attitude, and self-confidence of a group of psychiatric nurses in a major psychiatric hospital in southern Taiwan. The in-job training program in terms of sexual health care assessment and skills could provide psychiatric nurses a guideline for discussing related issues with the patients. Without appropriate attention to the sexual health needs of these patients, illness recovery might be prolonged, resulting in mental health comorbidities or suicide risks. Thus, psychiatric nurses must break out of their comfort zone and open the discussion about sexuality as a part of the holistic care process.
Footnotes
Acknowledgements
We would like to thank all the participating nurses who contributed their opinions to this study.
Author Roles
All authors contributed to the conception or design of the study or to the acquisition, analysis, or interpretation of the data. All authors drafted the manuscript, or critically revised the manuscript, and gave final approval of the version that was submitted for publication. All authors agree to be accountable for all aspects of the work, ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Kaohsiung Municipal Kai-Syuan Psychiatric Hospital.