
Abstract
Sexual health is a core component of overall well-being and depends on tightly coordinated signaling between the brain, endocrine organs, and peripheral autonomic pathways. This review synthesizes a neurochemical framework for understanding sexual desire, arousal, orgasm, and satisfaction, with a particular focus on how acute and chronic stress disrupt these processes. Dopamine-driven reward and motivation circuits support sexual interest and approach behavior, while serotonergic pathways often exert inhibitory control that can delay orgasm and reduce arousal effects commonly observed with serotonergic medications. Oxytocin contributes to intimacy, trust, and bonding, shaping relational closeness and post-sex “afterglow” experiences, whereas sustained activation of the stress response system and prolonged cortisol exposure can suppress libido and dysregulate downstream neuroendocrine balance. Orgasmic pleasure is further explained by the distinction between motivational “wanting” and hedonic “liking,” in which endogenous opioid signaling plays a central role in the subjective euphoria of orgasm and contributes to analgesia, satiety, and refractoriness. Clinically, this integrative model highlights why sexual dysfunction frequently co-occurs with anxiety, depression, chronic stress states, and medication effects, and it supports comprehensive management that combines psychosocial interventions, stress reduction strategies, and individualized pharmacologic review. The review also outlines translational directions, including scalable biomarker approaches to quantify chronic stress load and better stratify sexual dysfunction phenotypes in future research.
Introduction
Sexual health is a multifaceted aspect of human well-being, encompassing physical ability, psychological state, and interpersonal factors. Clinicians recognize that healthy sexual function depends on a delicate balance of neurochemical signals in the brain and body. 1 Key neurotransmitters and hormones, notably dopamine, serotonin, oxytocin, and cortisol, orchestrate the processes of sexual desire, arousal, and satisfaction. When these neurochemical systems are disrupted (e.g., by chronic stress or illness), sexual dysfunction can arise. This scoping review provides an overview of the neurochemical underpinnings of sexual health and dysfunction, with a focus on how chronic stress may act as a cause, a consequence, or a perpetuating factor in sexual disorders. We aim to present recent findings (including studies and meta-analyses) in an accessible way for a broad clinical audience, highlighting the roles of dopamine, serotonin, oxytocin, and cortisol in sexual function.
Dopamine: The Drive and Reward Behind Sexual Desire
Dopamine is often called the “reward” neurotransmitter and plays a pivotal role in sexual motivation and pleasure. Dopaminergic pathways in the brain reinforce the anticipation and reward of sex, making sexual activity desirable and satisfying. The mesolimbic and mesocortical dopamine systems, which include projections from the ventral tegmental area to the nucleus accumbens and cortex, are especially important for the preparatory phase of sexual behavior (libido, arousal, and motivational drive). 1 Early and recent studies consistently show that facilitating dopamine signaling tends to enhance sexual desire and performance, whereas blocking or depleting dopamine has the opposite effect. 1 For instance, in male subjects (preclinical and clinical), increased brain dopamine activity usually improves sexual activity, while lowered dopamine can worsen libido and erectile function. 1 Dopamine acts at specific receptor subtypes to exert these pro-sexual effects; research indicates that D₂ and D₄ dopamine receptors play major roles in promoting sexual arousal and erection. 1 These findings align with clinical observations: conditions characterized by low central dopamine (such as Parkinson’s disease) often feature reduced libido and erectile dysfunction (ED), whereas dopaminergic medications or agonists can sometimes restore sexual interest. In fact, a 2022 review noted that pharmacologically increasing central dopamine tends to facilitate male sexual behavior, and novel D₄ receptor agonists are being explored as treatments for ED. 1
Dopamine’s influence extends to multiple phases of sexual function. It not only heightens the desire and reward associated with sexual activity but also contributes to the motor and autonomic processes required for copulation. The brain’s nigrostriatal dopamine system helps coordinate the sensory-motor aspects of sexual activity (e.g., pelvic thrusting), while hypothalamic dopamine pathways trigger the reflexes for penile erection and orgasm. 1 Notably, there is a classic neurochemical interplay wherein dopamine facilitates sexual behavior, whereas serotonin tends to inhibit it. 1 This dopamine-serotonin balance is critical for normal sexual function. When dopamine signaling is dominant (relative to serotonin), individuals often experience increased sexual desire and arousal. Conversely, if dopamine activity is blunted, as can happen in depression or under chronic stress, patients may report apathy, anhedonia, and loss of libido. Recent neuroimaging studies support that dopamine release in reward pathways accompanies sexual arousal and orgasm, reinforcing the pleasurable aspects of sex. 1 Thus, healthy sexual function relies on robust dopaminergic tone, and dopamine dysregulation can manifest as hypoactive sexual desire or other dysfunctions.
Serotonin: Applying the Brakes on Sexual Excitation
Serotonin (5-HT) is a neurotransmitter widely known for stabilizing mood and modulating impulses. In the context of sexual function, serotonin generally has an inhibitory influence, particularly on sexual arousal and the timing of orgasm. 1 High levels of serotonin activity tend to “apply the brakes” to sexual processes, a phenomenon well exemplified by the side effects of selective serotonin reuptake inhibitors (SSRIs). Antidepressant arousal and serotonin (such as SSRIs) commonly cause sexual side effects in both men and women, including decreased libido, difficulty with arousal, and delayed or absent orgasm (anorgasmia). 2 In fact, increased serotonin can directly interfere with dopamine’s pro-sexual effects and even with peripheral sexual physiology. 3 One recent review summarized that excess serotonin may inhibit testosterone and dampen dopaminergic signaling, compounding its negative impact on sexual function. 4 Clinically, this is why some patients on SSRIs experience blunted sexual desire and pleasure.
On the other hand, serotonin’s inhibitory role can be therapeutically useful in certain scenarios. For example, premature ejaculation in men is often treated with low-dose SSRIs precisely because elevating serotonin delays ejaculation latency. 5 This illustrates that serotonin helps regulate the timing of orgasm: higher serotonin activity is associated with a prolonged time to climax, whereas lower serotonin (or blocking certain 5-HT receptors) can accelerate orgasm. 5 The balance between different serotonin receptor subtypes also matters. Activation of 5-HT_2C receptors, for instance, has been linked to reduced sexual arousal, while blockade or partial agonism of 5-HT_1A receptors (which can disinhibit dopamine) may alleviate SSRI-induced sexual dysfunction. Researchers have even identified post-SSRI sexual dysfunction (PSSD) as a condition where sexual side effects persist after discontinuing the medication, underscoring serotonin’s potent and lasting impact on sexual neurochemistry. 6
In summary, serotonergic tone must be optimally balanced: enough to maintain mood and impulse control, but not so excessive as to extinguish sexual desire. The classic dopamine-serotonin dichotomy in sexual function is well documented in animal studies: augmenting dopamine facilitates sexual activity while augmenting serotonin inhibits it. 7 For a healthy sexual response, there needs to be a coordinated dance where dopamine-driven excitation is not overly constrained by serotonin. Clinicians should be aware that medications and conditions affecting serotonin (such as antidepressants, chronic anxiety, or stress) can present with sexual side effects. Personalized strategies like switching antidepressant classes, dose adjustment, or add-on treatments (e.g., adding a dopaminergic agent or 5-HT_1A agent to counter SSRI side effects) are often employed to manage serotonin-related sexual dysfunction. 8
Oxytocin: Bonding Hormone and Facilitator of Intimacy
Oxytocin, often dubbed the “love hormone,” is a neuropeptide that plays a critical role in social bonding, affectionate touch, and sexual climax. It is released in bursts during physical intimacy plasma oxytocin levels rise during sexual activity, peaking at orgasm (ejaculation). 9 Oxytocin’s effects on sexual function are generally facilitatory. In the central nervous system, oxytocin acts on hypothalamic and limbic circuits to enhance sexual arousal and pair bonding, reinforcing the emotional connection between partners. Peripherally, oxytocin causes contraction of smooth muscles (e.g., uterine and pelvic muscle contractions during orgasm), and in males, it can promote aspects of erection and ejaculation. Animal research has provided striking evidence: administering oxytocin or agonists can stimulate sexual behavior and penile erection in laboratory animals, whereas oxytocin antagonists dampen sexual activity. 10 Certain hypothalamic neurons (in the paraventricular nucleus, PVN) that produce oxytocin are directly involved in erection initiation; interestingly, these oxytocinergic neurons can be activated by dopamine, linking the dopamine and oxytocin systems in a pro-sexual network. 11 In male rats, microinjection of dopamine agonists into the PVN triggers oxytocin release that induces erections, 12 highlighting an interaction where dopamine’s pro-erectile effect is partly mediated by oxytocin. This has led researchers to describe oxytocin as a central “facilitator” of sexual function in both sexes, supporting arousal, orgasm, and the sense of pleasure and satiety after sex.
Beyond its role in the mechanics of sexual response, oxytocin crucially influences the psychological dimensions of sexuality. It fosters trust, bonding, and intimacy between partners. The surge of oxytocin during orgasm is thought to contribute to the afterglow and emotional closeness post-sex. Elevated oxytocin also modulates stress responses, often producing calming, anti-stress effects. 13 This is particularly relevant in the context of chronic stress and sexual dysfunction: oxytocin can counteract some negative effects of cortisol and anxiety, potentially mitigating stress-related sexual problems. 14 Intriguingly, a 2022 study on men with compulsive sexual behavior (“hypersexual disorder”) found paradoxically high oxytocin levels in these individuals, which researchers interpreted as a compensatory mechanism to attenuate their concurrently hyperactive stress systems. 15 In other words, the body might be releasing more oxytocin to try to buffer the detrimental impact of chronic stress or anxiety in those with dysregulated sexual behavior. This finding underscores the complex bidirectional relationship between oxytocin and stress: while acute oxytocin release usually reduces stress, chronic stress can alter oxytocin signaling in unpredictable ways (sometimes leading to upregulation of oxytocin as the body attempts to restore equilibrium). 15
From a therapeutic standpoint, oxytocin is being explored as a treatment for certain sexual dysfunctions. Early pilot trials have examined intranasal oxytocin in women with arousal or orgasmic disorders, with some reports of improved sexual satisfaction (though often alongside placebo effects). 16 Given oxytocin’s role in arousal and its relative safety, it holds some promise as an adjunct for patients with low desire or difficulty achieving orgasm, especially when relationship intimacy issues or anxiety are contributing factors. However, more research is needed, and any use of oxytocin in this context should be approached cautiously. Overall, oxytocin represents the positive, bonding side of sexual neurochemistry, promoting not just the physical act of sex but also the emotional connectivity and relaxation that ideally accompany healthy sexual experiences.
Cortisol and Chronic Stress: The Sexual Function Antagonist
In stark contrast to the pleasurable neurochemicals above, cortisol is a hormone most associated with stress, and its impact on sexual health is largely negative. Cortisol is the end-product of the hypothalamic-pituitary-adrenal (HPA) axis, released by the adrenal glands during times of stress. Acute spikes in cortisol (as part of the “fight-or-flight” response) can interfere with sexual arousal. For example, sudden stress or anxiety can abort an erection or make arousal difficult. Under normal conditions, sexual arousal correlates with a reduction in cortisol: a study in healthy men showed that as sexual stimulation commenced and erection developed, cortisol levels decreased in the blood (both in systemic circulation and within the penile erectile tissue). 17 This drop in cortisol appears to be a prerequisite for a fully erectile response, essentially removing the inhibitory effects of stress hormones during intimacy. 17 The same study found that men with ED did not exhibit the normal decline in cortisol during arousal. 17 This suggests that excess or unchanging cortisol may act as an “antagonist” of the sexual response cycle, 17 preventing the body’s typical relaxation and vascular responses needed for sex.
Chronic elevation of cortisol, such as in individuals with long-term stress or certain medical conditions like Cushing’s syndrome, is strongly associated with sexual dysfunction. Hypercortisolism is linked to decreased libido and impaired sexual performance. 17 Clinically, patients under chronic stress often report loss of sexual desire, difficulty achieving arousal, or fatigue that dampens sexual interest. Biologically, prolonged stress and high cortisol can suppress the gonadal hormones (like testosterone) and neurotransmitters that support sexual function. 18 For instance, cortisol can inhibit gonadotropin-releasing hormone (GnRH) and subsequently lower testosterone levels in both men and women, contributing to low libido. 18 High cortisol is also associated with vasoconstriction and endothelial dysfunction, which may impair genital blood flow necessary for erection or lubrication. 19 A 2023 translational study in men provided direct evidence of cortisol’s inhibitory role: men with ED had a blunted cortisol decrease during arousal compared to healthy men, and the authors concluded that dysregulated cortisol secretion or clearance likely plays a role in ED pathophysiology. 17 In other words, if stress hormones remain high when they should be tapering off (during sexual activity), the sexual response is hampered.
It is important to recognize that not all evidence about cortisol is straightforward. Some animal studies paradoxically showed enhanced mating behavior when cortisol was experimentally increased, 17 suggesting a complex dose- and context-dependent effect. Nonetheless, the bulk of human evidence indicates that a state of chronic stress (high cortisol) is detrimental to sexual health, whereas stress reduction can be beneficial. In healthy males, cortisol naturally peaks early in the day and dips in the evening, aligning with typically higher sexual interest at night when cortisol is lower. This circadian pattern further supports cortisol’s inverse relationship with sexual readiness. For clinicians, managing patients with sexual dysfunction should include an assessment of stress levels and, if indicated, measuring cortisol (or other stress markers) like hair and nail cortisol and DHEA concentration, which are newer and novel approaches which need to be studied in sexual dysfunction cases. 20 Integrative interventions that lower chronic stress (counseling, mindfulness, exercise, improved sleep) may, in turn, lower cortisol levels and help restore more normal sexual function. One can conceptualize cortisol as a biochemical brake; when it is chronically engaged, it can block the neurovascular changes needed for sexual arousal and satisfaction. 17
Chronic Stress and Sexual Dysfunction: A Vicious Cycle
The relationship between stress and sexual dysfunction is bidirectional and often cyclical. On one side, chronic stress can cause or exacerbate sexual dysfunction; on the other, experiencing sexual dysfunction can itself become a significant source of stress and psychological distress. This two-way link can trap individuals in a self-perpetuating cycle. For example, a person under intense work stress may develop erectile issues or loss of libido due to neuroendocrine imbalances (high cortisol, low dopamine/testosterone). This new sexual problem can then lead to performance anxiety, reduced self-esteem, relationship conflicts, and further stress, which in turn makes the sexual dysfunction worse.
Stress activates the HPA axis and sympathetic nervous system, flooding the body with cortisol and adrenaline. These changes can acutely divert blood flow and attention away from sexual organs (the classic fight-or-flight response is the opposite of the “rest-and-digest” state that favors sexual arousal). Over time, stress may alter neurotransmitter levels; for instance, it is known to deplete dopamine and serotonin balance in the brain, potentially leading to depressive symptoms and sexual apathy. Epidemiological studies have found that people with high stress scores are more likely to report sexual dysfunction. In women, psychological stress has been significantly associated with female sexual dysfunction (FSD). A recent systematic review of reproductive-aged women noted that those with high stress (measured by validated scales) had markedly greater odds of FSD; in pooled analyses stress was associated with more than double the risk of sexual dysfunction (odds ratio ~2.3). 21 Similarly, in men, anxiety disorders and chronic work stress are recognized risk factors for ED. Meta-analyses indicate that men with anxiety (which often involves chronic stress arousal) have a higher incidence of ED compared to those without anxiety.22,23 The Heliyon 2024 review on stress and behavior succinctly stated that stress “alters sexual function via complex interactions of neuromodulator pathways,” 24 reinforcing that sustained stress can disrupt the biochemical pathways (dopamine, serotonin, oxytocin, testosterone, etc.) that normally support a healthy sex life.
Stress, therefore, Modern diagnostic definitions of sexual dysfunction (e.g., female sexual interest/arousal disorder, male hypoactive sexual desire disorder, erectile disorder) require that symptoms cause marked distress or interpersonal difficulty. Indeed, the presence of personal distress is often what differentiates a “dysfunction” from a mere variation in sexual function. 21 When individuals experience problems like inability to perform sexually, lack of desire, or inability to achieve orgasm, it commonly leads to frustration, anxiety, and lowered self-worth. This psychological distress can be substantial; for instance, men with ED often report symptoms of depression or performance anxiety and worry about their partner’s perception. Such stress can further elevate cortisol and adrenaline during subsequent sexual attempts, essentially creating performance anxiety that reinforces the dysfunction. In women, distress about sexual performance or lack of satisfaction can manifest as relationship stress, mood disturbances, and avoidance of intimacy, all of which feed back into heightened overall stress. Research has shown that marital and sexual dissatisfaction can significantly elevate stress and even correlate with mental health issues like depression. 21 In short, sexual dysfunction is rarely “all in the head,” but it invariably occupies the mind, the worries and emotional pain it causes are real stressors that deserve clinical attention alongside the physical aspects.
Given this bidirectional relationship, it is helpful to think of chronic stress and sexual dysfunction as both cause and consequence, often intertwined. A patient may initially be presented with stress-induced sexual problems, but over time, the presence of those problems generates new stress that compounds the issue. Breaking this cycle is a key therapeutic goal. Interventions may need to tackle both sides: stress reduction techniques to alleviate the physiological burden on sexual function, and sexual counseling or medical treatments to improve dysfunction and thus relieve the psychological strain. For example, cognitive-behavioral therapy or couples therapy can reduce the anxiety component and improve coping, while pharmacotherapy (like a PDE5 inhibitor for ED, or switching an SSRI to a less sexually side-effect-prone antidepressant) can restore confidence in one’s sexual capability, thereby reducing stress. Relaxation practices, exercise, and adequate sleep, all known to lower chronic cortisol levels, can be prescribed as part of a holistic approach to improve sexual health. 25
Cortisol Dysregulation and Sexual Function: The Stress Hormone Spectrum
Hypercortisolism
Endogenous hypercortisolism (e.g., Cushing’s disease) or exogenous steroid use (e.g., dexamethasone) impairs sexual function by suppressing GnRH and reducing circulating sex hormones. Dexamethasone suppression testing is used to diagnose Cushingoid states, which are often accompanied by low libido, ED, amenorrhea, and mood instability. 26
Hypocortisolism
Conversely, hypocortisol states, such as in Addison’s disease or chronic fatigue syndromes, may lead to sexual fatigue, low arousal, and reduced sexual initiative. In major depressive disorder, hypocortisolism due to HPA axis blunting can co-occur with anhedonia and sexual withdrawal. 27
Both ends of cortisol imbalance disturb the delicate neuroendocrine dance involving dopamine, testosterone, and oxytocin, underscoring the role of stress biology in sexual health.
Sex Hormones and HPA Axis Responsiveness: Key Findings from Rodent and Human Studies
Experimental studies in rodents have demonstrated that sex hormones significantly influence the HPA axis response to stress. In female rats, administration of testosterone (an androgen) induced a male-like pattern of corticosterone secretion, suggesting that androgens dampen HPA axis activity. Conversely, estradiol (a primary estrogen) was found to upregulate proopiomelanocortin (POMC) mRNA in the pituitary, promoting ACTH production and enhancing corticosterone response. Ovariectomy (OVX), which depletes endogenous estrogens, blunted stress-induced corticosterone release, whereas estradiol replacement restored and even amplified it. In male rats, castration led to increased stress-induced corticosteroid levels, while androgen replacement (testosterone or dihydrotestosterone) suppressed them. Overall, estrogens appear to enhance, while androgens suppress, HPA axis responsiveness. 26
These findings extend to humans, where sex hormone fluctuations during the menstrual cycle influence cortisol reactivity. Studies indicate that women exhibit stronger HPA responses during the low-estrogen follicular phase compared to the luteal phase. However, human data remain mixed: some studies report heightened ACTH responses in men, while others find higher cortisol reactivity in elderly women, depending on the nature of the stressor. These observations highlight that the influence of sex hormones on HPA axis activity is complex and context-dependent, shaped by hormone type, physiological state, and stressor characteristics.
Beyond Sex Hormones: Additional Modulators of HPA Axis Activity
While sex hormones clearly influence HPA axis responsiveness, several other physiological and metabolic factors also modulate glucocorticoid signaling. For instance, obesity and weight gain are associated with altered HPA activity, potentially through changes in glucocorticoid receptor (GR) isoform expression. Alhaddad et al. demonstrated that chronic ethanol consumption modifies GR isoforms in brain regions of alcohol-preferring rats, suggesting substance use and metabolic status may alter central stress regulation. 28
Inflammation and impaired insulin signaling are also known to suppress glucocorticoid feedback mechanisms, contributing to HPA axis dysregulation. Additionally, plasma proteins such as corticosteroid-binding globulin (CBG) and albumin influence the free circulating levels of cortisol and thus the bioavailability of intracellular glucocorticoids. 29
Future research is needed to explore how sex hormones affect the metabolism of glucocorticoids. Preliminary evidence suggests that they may regulate hepatic enzymes such as cytochrome P450S and UDP-glucuronosyltransferases (UGTs), which are responsible for glucocorticoid clearance. 30 This opens the possibility of sex-based differences in glucocorticoid elimination, though further data are required to substantiate this.
Asthma and Respiratory Drugs: The Overlooked Link to Sexual Side Effects
Bronchodilators, including β2-agonists like salbutamol and anticholinergics like ipratropium, may act as central nervous system stimulants in some users. These agents can indirectly influence arousal and mood, especially at higher doses, via their sympathomimetic effects. Though usually prescribed for pulmonary conditions, such drugs may trigger restlessness, insomnia, or hyperarousal in sensitive individuals, sometimes affecting libido or sexual performance. 31
Systemic corticosteroids used in asthma and COPD can suppress endogenous sex hormone production when used chronically, leading to reduced testosterone or estrogen levels and consequent sexual dysfunction. Additionally, corticosteroids may exacerbate mood lability, weight changes, and self-image issues, all of which can impact sexual confidence and partner interaction. 32
Recent studies also indicate that long-term inhaled corticosteroids may affect HPA axis function in a dose-dependent manner, although reversible. 33 This underscores the need for sexual health monitoring in patients on chronic pulmonary regimens.
Endorphins: The Brain’s Natural Pleasure Amplifiers
Endorphins are endogenous opioid neuropeptides released in response to stress, pain, and pleasurable activities, including sexual activity. These peptides bind to opioid receptors in the brain and spinal cord, reducing pain perception while enhancing a sense of euphoria and well-being. During sexual arousal and orgasm, elevated endorphin levels are associated with emotional bonding, reduced anxiety, and post-coital calm. 34
Endogenous opioids such as β-endorphins and enkephalins are released in key brain regions during sexual stimulation and orgasm, producing intense euphoria and analgesia through mass activation of μ-opioid receptors. Landmark studies by Komisaruk and Whipple demonstrated that orgasm-induced analgesia in both women and animals is mediated by this endogenous opioid system. 35 In chronic stress states, where cortisol is persistently elevated, endorphin production may become dysregulated, contributing to anhedonia and reduced libido.
Moreover, physical touch and affectionate behavior such as hugging, kissing, or prolonged skin contact stimulate endorphin release, which in turn may support emotional intimacy and relational bonding, particularly in long-term couples. 34
Opioid & Oxytocin Coupling and Partner Bonding
Beyond producing orgasmic pleasure, endogenous opioid “reward states” appear to train the brain to prefer specific partner cues by recruiting oxytocin-based bonding circuits. In animal models, orgasm-like opioid responses generate a conditioned partner preference that is reversible with naloxone, and this learning is accompanied by activation of hypothalamic oxytocin neurons along with mesolimbic/hypothalamic dopamine pathways; similarly, the long-acting opioid antagonist naltrexone blocks partner preference formation in monogamous prairie voles. This supports the broader view in our review that oxytocin strengthens intimacy, trust, and pair bonding, contributing to the post-sex “afterglow” and buffering stress response effects that may be amplified when oxytocin signaling is engaged during opioid-mediated sexual reward. 34
Wanting and Liking Neurochemicals
Sexual reward has two separable components: dopamine-driven incentive motivation (“wanting”) and endogenous opioid-mediated orgasmic euphoria (“liking”). During orgasm, widespread opioid activation is proposed to abruptly inhibit dopamine transmission (with prolactin rise as a marker), while serotonin contributes to satiety and refractoriness linking pleasure, afterglow, and post-orgasm sleepiness into a unified neurochemical model. 34
Testosterone, DHEA, and Prolactin: Hormonal Triad Shaping Sexual Health
Testosterone
Testosterone plays a crucial role in sexual desire and arousal in all genders, though it is more pronounced in men. It enhances dopaminergic activity in the hypothalamus and preoptic area, facilitating libido, genital sensitivity, and erectile function. Low testosterone levels are consistently associated with hypoactive sexual desire disorder and ED in men and, to a lesser extent, reduced sexual responsiveness in women. 36
DHEA (Dehydroepiandrosterone)
DHEA is often termed the “master hormone” because it serves as a precursor to both androgens (testosterone) and estrogens. It also exhibits independent neuroactive properties that enhance mood and resilience to stress. DHEA levels decline with age and chronic illness, often correlating with decreased libido, fatigue, and emotional blunting. Clinical trials using DHEA supplementation in both men and postmenopausal women have shown modest improvements in sexual satisfaction and arousal. 37
Prolactin
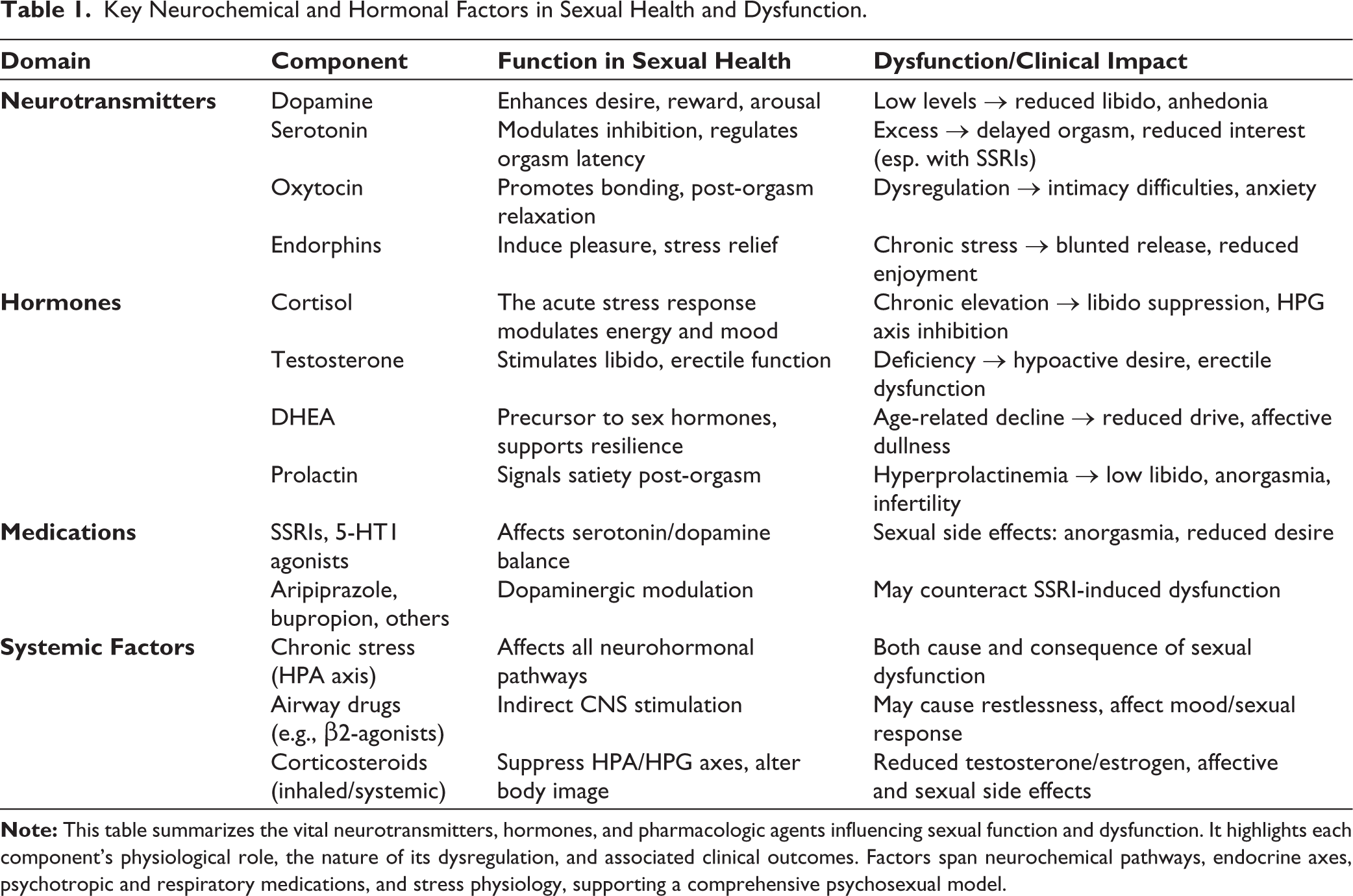
Prolactin is released in response to orgasm and contributes to sexual satiety and the refractory period. While acutely beneficial in ending sexual episodes, chronically elevated prolactin (e.g., due to prolactinoma, antipsychotic medications, or hypothyroidism) is associated with suppressed GnRH, hypogonadism, and sexual dysfunction. Symptoms can include low libido, erectile difficulty, and anorgasmia. 38 Key neurochemical and hormonal factors in sexual health and dysfunction are summarized in Table 1.
Key Neurochemical and Hormonal Factors in Sexual Health and Dysfunction.
Orgasmic Dysfunction in Clinical Practice Is Heterogeneous
Patients may report delayed orgasm/anorgasmia or a distinct “anhedonia orgasm” (PDOD), where climax occurs but orgasmic pleasure is absent. 34 Mechanistically, the recent review study highlights three common clinical pathways: (a) inadequate sympathetic arousal to activate the spinal LSt climax generator (e.g., insufficient stimulation, hyper inhibition of sympathetic outflow, interpersonal issues, boredom, age-/injury-related loss of Genito sensory signaling, or attempting arousal while still refractory, including in compulsive sexual behavior patterns); (b) drug/substance-induced anorgasmia, particularly with SSRIs, excess alcohol (blunted sensory input), or chronic opioid/opiate use; and (c) PDOD, which is reported in association with psychiatric disorders (depression/anxiety) and sometimes dopamine antagonists, and is also described alongside syndromes such as PSSD and post-orgasmic illness syndrome, where post-orgasm symptoms can blunt pleasure. 34
Psychotropic Medications and Sexual Health: SSRIs and Beyond
Selective Serotonin Reuptake Inhibitors
SSRIs are commonly associated with sexual side effects such as decreased libido, delayed ejaculation, anorgasmia, and ED. These adverse effects are linked to excessive serotonergic activity at 5-HT2 and 5-HT1A receptors, which suppress dopaminergic function in the mesolimbic system. 39
5-HT1A Agonists and Adjunctive Agents
Aripiprazole, a partial D2 and 5-HT1A agonist, is increasingly used as an adjunct to SSRIs for antidepressant-induced sexual dysfunction. It has been shown to restore dopaminergic tone in mesolimbic circuits and improve libido and orgasm latency in both sexes. 40
Balovaptan, a vasopressin V1a receptor antagonist under investigation for social cognition disorders, shows potential to modulate affiliative behavior and sexual responsiveness, though clinical applications remain under study. 41
Other newer antidepressants like bupropion, vilazodone, and vortioxetine, which have mixed serotonergic and dopaminergic activity, exhibit lower sexual side effect profiles and may be considered alternatives or adjuncts. 42
Conclusion and Clinical Implications
In summary, sexual health is deeply rooted in neurochemical balance, and chronic stress can tip that balance in unfavorable ways. Dopamine and oxytocin emerge as positive players that drive sexual desire, pleasure, and bonding, whereas serotonin (at high levels) and cortisol can impose brakes on sexual function. Chronic stress, often accompanied by persistently elevated cortisol and altered neurotransmitters, should be viewed as both a precipitant of sexual dysfunction and a perpetuating factor via the distress it causes. This neurochemical perspective is not merely academic; it has practical implications for clinical management of sexual problems. It suggests that effective treatment may require addressing biological, psychological, and social facets: for instance, using pharmacological agents to modulate neurotransmitters (dopamine agonists, oxytocin analogs, or adjusting SSRIs) and implementing stress reduction and psychotherapy techniques to break the stress-dysfunction cycle.
Importantly, ongoing research continues to shed light on these mechanisms. New studies and meta-analyses in the last few years have reinforced our understanding: a 2023 study confirmed cortisol’s inhibitory effect on male sexual arousal, 17 recent meta-analyses link psychological stress to sexual dysfunction prevalence, 21 and novel investigations into oxytocin’s role hint at future therapies. 25 For the broader clinical audience, the take-home message is clear: when evaluating and treating sexual dysfunction, consider the patient’s stress level and neurochemical milieu as integral components of the disorder. By viewing sexual dysfunction through a neurochemical lens, clinicians can better empathize with the physiological reality of their patients’ complaints (it is not “just in their mind”) and design comprehensive treatment plans. In the spirit of holistic care, attending to stress and neurochemical health will not only improve sexual outcomes but also enhance overall quality of life for our patients.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethical permission was not applicable to this article, as this is a review article drafted from various research articles and not from patients directly.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
All the authors contributed substantially to the work, participated in the writing, and have seen and approved the submitted.