
Abstract
Background:
Despite the fact that there have been significant advances in the prevention and treatment of sexual dysfunction in India, the majority of these have focused on male sexual dysfunction disorders and there is still a paucity of literature that adequately explains the relationship between sexual knowledge and attitudes and female sexual dysfunction (FSD). Furthermore, physiological events such as pregnancy, childbirth, breastfeeding, menopause, and ageing have a significant impact on sexual well-being, particularly when co-morbid psychiatric illnesses are present. The prevalence of these interactions and their relationship with FSD is expected to have consequences in the prevention and treatment of FSD.
Aim:
To assess sexual health knowledge and attitudes regarding sexual practices in women attending Obstetrics and Gynaecology OPD and assess presence and extent of sexual dysfunction in them.
Methods:
This was a hospital-based cross-sectional study with a sample size of 220 women in the category of pregnant, nulliparous and perimenopause/menopause/post menopause. The SKAQ-II (Sexual Knowledge and Attitude questionnaire) assessed their sexual knowledge and attitude, and Female Sexual Functioning Index scale (FSFI) evaluated sexual dysfunction.
Results:
Ninety-three percent of the women had an adequate amount of knowledge regarding sexual practice and 83.2% had a liberal attitude. Rural women had lower levels of sexual knowledge and a conservative attitude towards sexual practice. Level Sexual knowledge and attitude were positively correlated with the presence of sexual dysfunction, with the prevalence of later being 65.5%—with 63% of pregnant women having sexual dysfunction, and 77.8% of menopausal women having sexual dysfunction.
Conclusion:
Women with greater sexual knowledge and a liberal mindset towards sexual practices tend to have lower levels of sexual dysfunction. Rural women tended to have lower levels of sexual knowledge and a poor attitude towards sexual practice, there was no association found between religious attitudes. Most dysfunction was faced by the menopausal age group. Sexual issues were more common in the domains of desire, lubrication, orgasm and pain. A positive correlation was noted between sexual dysfunction and kind of housing, leading to a lack of intimacy being an important contributing factor.
Keywords
Introduction
Sexual functioning is a multifaceted process influenced by a variety of biological, psychological and social aspects. 1 Healthy sexual functioning and satisfactory marital intercourse have been viewed as one of the foundations of a lasting and intimate relationship, along with being important determinants in spouses’ physical and mental well-being. 2
Around the world, about 60%–80% of women have reported suffering from various forms of sexual dysfunction, which directly/indirectly has implications on several aspects of their lives. 3 In India, this can be even more complicated, as female sexuality has been, from time immemorial, considered taboo for many, and women often hesitate to talk about their sexual problems and needs with the healthcare worker. 4
Sexual Functioning in Pregnancy and Menopause
In addition, there are various physiological stages in a woman’s life in which sexual functioning can be affected due to a variety of hormonal changes as seen in pregnancy, postpartum and menopausal transitions. Abandoning sexual activity and feeling guilty about sexual relations during pregnancy, altered body image, reduced sense of attraction for the spouse, fear of injury to the foetus, fear of abortion and early childbirth are some of the factors that can affect a woman’s sexual response and, as a result, the couple’s relationship, leading to anxiety and lack of self-confidence in couples and, eventually, disrupting the family’s mental health. 5
Despite the fact that previous studies6,7 have confirmed that sexual intercourses among low-risk pregnant women are not associated with any complication (such as the risk of abortion, premature rupture of membranes or preterm labour), many women still have reservations about sexual activity, and this issue is one of the main causes of their concern, leading to low sexual desire. 8 These incorrect assumptions can have a substantial impact on a woman’s sexual response and put a pregnant woman’s sexual health in jeopardy. 9
Also, during the menopausal transition, a drop in oestrogen levels lead to genital atrophy—the uterus shrinks in size, and the vulva and vaginal tissues lose thickness and vascularity. 10 Cervical and Bartholin gland secretions also decrease, contributing to vaginal dryness and altered pH. 11 In addition, the most common misconception regarding menopause is that the end of a woman’s fertility is the end of her sexual life, due to which the percentage of women with sexual dysfunction increases twofold as they progress through the menopausal transition. 12
There has been a paucity in literature to correlate the knowledge and attitudes of Indian women towards sexual health with the presence of sexual dysfunction and assessing the other factors, such as religious beliefs, type of family, type of housing, educational levels and rural/urban background, which might further affect sexual health. This study is a modest attempt to highlight the prevalence of sexual dysfunction in these vulnerable populations—pregnancy, perimenopausal/menopausal women and their correlation with sexual knowledge and attitudes, as well as to evaluate for other contributing factors.
Methodology
Source of Data
Sample collection was carried out from the general population of women attending the Obstetrics and Gynaecology Outpatient department of a tertiary care urban hospital in Mysuru, Karnataka, which included antenatal and gynaecology clinics.
Sample Size
Two hundred twenty pregnant, premenopausal/menopausal/perimenopausal and nulliparous women were recruited above 18 years and below 65 years of age. This included 100 pregnant, 90 perimenopausal/menopausal/postmenopausal women and 30 nulliparous women who gave their consent and were willing to respond to the questionnaires.
Study Design and Timeline
Hospital-based cross-sectional study, conducted from October 2020 to February 2022.
Inclusion Criteria
Women aged between 18 and 65 years.
Women coming for treatment or follow-up to the OBG OPD.
Exclusion Criteria
Inability to provide required information.
High-risk pregnancies.
Women with gestational age around term (period of gestation beyond 36 weeks).
Tools for Assessment
Women qualifying for the study criteria were assessed with the following scales/questionnaires:
Socio-demographic proforma: Which includes details regarding name, age, marital status, obstetric/gynaecological status (pregnant, perimenopausal/menopausal/postmenopausal, nulliparous), domicile (rural/urban), education, occupation, religion, family structure, family size, housing conditions and religion. Sexual Knowledge and Attitude Questionnaire (SKAQ-II): For knowledge about sexual practices and attitudes towards sex. This is a 55-item questionnaire, one of the first self-rating Indian scales to be devised by Avasthi et al.
13
from the Department of Psychiatry, Post Graduate Institute of Medical Education and Research (PGIMER), Chandigarh, which was constructed and standardised to assess the sexual knowledge of the Hindi-speaking North Indian population. The basis of creating this standard questionnaire was that misconceptions and ignorance about sexual practices, along with poor sexual attitudes, were a perpetuating factor of sexual disorders.
14
The principal source of the items in the questionnaire was the 106-item Sex Knowledge and Attitude test (SKAT) questionnaire devised by Lief and Reed
15
which was modified to the Indian scenario. It is a two-part questionnaire containing 55 questions, wherein SKAQ-A is a 35-item knowledge section with dichotomous response options, and SKAQ-B is the 20-item attitude section that can be scored on a 3-point Likert scale. Total scores on the SKAQ-A and SKAQ-B are 35 and 60, respectively. Greater scores indicate higher knowledge and a more liberal mindset. Female Sexual Function Index (FSFI): A 19-item questionnaire was created as a quick, multidimensional self-report tool for assessing the essential elements of female sexual function. Devised by Rosen et al.
16
in 2000, this scale contained six domains, which include desire, subjective arousal, lubrication, orgasm, satisfaction and pain. Each question is scored from 0 (lowest) to 5 (highest) except questions 1, 2, 15 and 16, which are scored from 1 to 5. Each domain score has a maximum score of 6, making the total possible score 36. The presence of female sexual dysfunction (FSD) is taken when the total score falls below or equals 26.55.
Procedure for Conducting the Study
Before starting the study, Institutional Ethical Committee clearance was obtained. Women between the ages of 18 and 65 years attending the Obstetrics and Gynaecology OPD for treatment or follow-up who met the inclusion criteria were recruited and subjected to the study. Elaborate demographic details were taken along with obstetric status, family size and housing conditions, attitude to religion and rural/urban background.
The attitude and knowledge towards sexual practices were assessed with the two-part SKAQ-II questionnaire, presence and quantity of sexual dysfunction were assessed with FSFI. Since the SKAQ-II questionnaire was devised in the Hindi language, translators were used to explain the questions to patients in the vernacular language and their responses were recorded.
Statistical Analysis
The descriptive statistics, including quantitative variables like mean, standard deviation and range and qualitative variables like percentages and frequencies, were calculated. For comparing means of more than two groups, One-way Analysis of Variance (ANOVA) was used. Scheffe’s Post Hoc test was done to confirm the differences occurring between the groups. Frequency distributions of categorical variables across two or more groups were done using the chi-square test.
Data were analysed using the Statistical software named Statistical Package for Social Sciences (SPSS) 23.
Results
A total of 220 women attending the OBG OPD were taken and detailed history, including socio-demographic data, obstetric/gynaecologic status, urban/rural background, family structure and size, housing condition, religious attitude, were collected, and the above-mentioned scales were applied.
It was seen that uniform age distribution was present ranging from age 18 to 65 years of age with, 14.1% were from 18 to 25 years, 23.2% from 26 to 30 years, 18.2% from 31 to 40 years, 25.2% from 41 to 50 years and 19.1% between 51 and 65 years of age.
One hundred women, 45.5% of sample population, were chosen from the antenatal clinic, who had come for regular follow-ups and were from different trimesters of pregnancy. Of the total participants, 40.9% (n = 90) were from the gynaecology clinic and had come for various gynaecological issues such as menopausal hot flushes, gynaecological cancers, fibroids, pelvic floor prolapse, etc. Additionally, 13.6% (n = 30) of the women were nulliparous and had visited the clinic for concerns such as dysmenorrhea, PCOS/PCOD, infertility, menstrual disorders, vaginal white discharge etc.
There was an almost equal distribution regarding domicile of the patients, with 55% of them belonging to an urban background and 45% from a rural area.
Among the women, only 11.8% were illiterate, 15.5% mentioned having gone till primary school, 15.9% and 20% said they completed till middle and high schools, respectively, whereas 25.5% and 11.4% women had done higher studies till graduation and post-graduation, respectively. Most of the women were educated enough to answer most of the questionnaire on their own and did not require much translation.
Of the total women recruited, the majority of them, 36.4%, were homemakers, only 1.8% were pursuing their studies and were students, whereas 12.7% and 18.6% of them were involved in unskilled and semi-skilled jobs. 19.1% said they were doing jobs which took skilled abilities, and 11.4% mentioned they were involved in their own business.
The majority of the sample size, 55.5%, identified to be Hindu, 24.1% identified themselves as Muslims and 20% identified as Christians, whereas 0.5% identified with another religion. Out of these, 37.3% stated that they had a rigid outlook towards religion, 24.5% mentioned having a not very rigid religious attitude, and 38.2% mentioned their attitude was moderate.
44.1% of women were staying in nuclear families, 26.4% belonged to joint families, and 29.5% mentioned staying in extended nuclear families. 35.9% of women did not have any children, 36.8% mentioned having one to two children, 22.7% reported having three to four children and 4.5% mentioned having more than four children. Most of the women, 78.6% mentioned having individual houses/rooms, 15.9% and 5.5% reported sleeping with their children or having a common sleeping place, respectively.
Sexual Knowledge and Attitudes
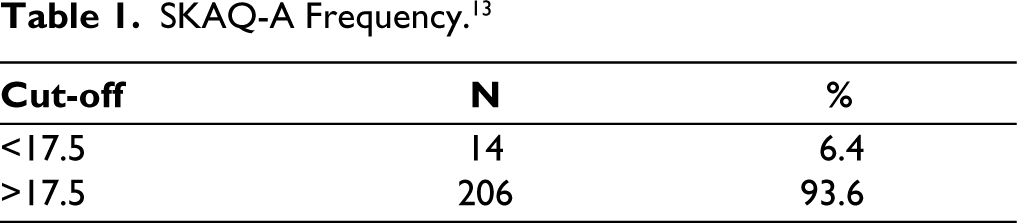
In the sexual knowledge section of the SKAQ questionnaire, majority of women 93.6% scored above the cut-off limit of 17.5 and only 6.4% had a score below 17.5, indicating that the overall sexual knowledge was adequate (Table 1). The questions were regarding whether sex education is an important aspect to be taught to children, their concept regarding masturbatory practices, safe sexual practices, menstrual hygiene, pre-marital sex and myths such as size of penis affecting sexual practice, absence of hymen indicating loss of virginity, loss of virility due to ageing, increased sexual desire being harmful for overall health, knowledge of sexual health making children promiscuous and whether having sexual knowledge promoted sexual activity. Most women had good awareness of sexual knowledge.
SKAQ-A Frequency. 13
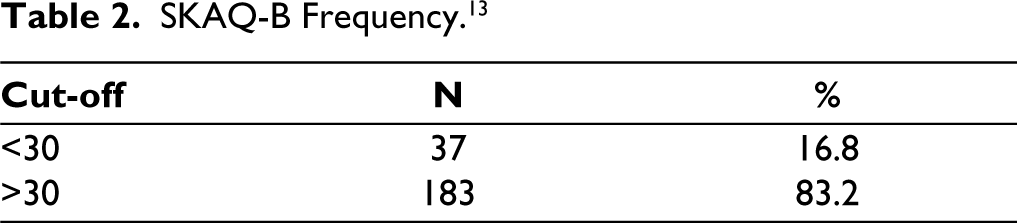
In the sexual attitudes part of SKAQ questionnaire, 83.2% of women scored higher than the mean value, and 16.8% fell below the average score (Table 2). These questions were about homosexuality, abortion, masturbatory practices, extra-marital sex and preservation of virginity before marriage, use of other forms of sexual practice apart from peno-vaginal intercourse for pleasure. Most women displayed a liberal attitude towards sexual behaviours.
SKAQ-B Frequency. 13
A positive association was found between the domicile of the women and the level of sexual knowledge as well as open-mindedness towards sexual practices. Women from a rural background were more likely to have lower levels of sexual knowledge—12.6% as compared to 1.6% of women who scored less on the SKAQ-A scale. Similarly, 30.6% of women from rural areas had a less liberal attitude about sexual practices as compared with 5.7% women from urban domicile.
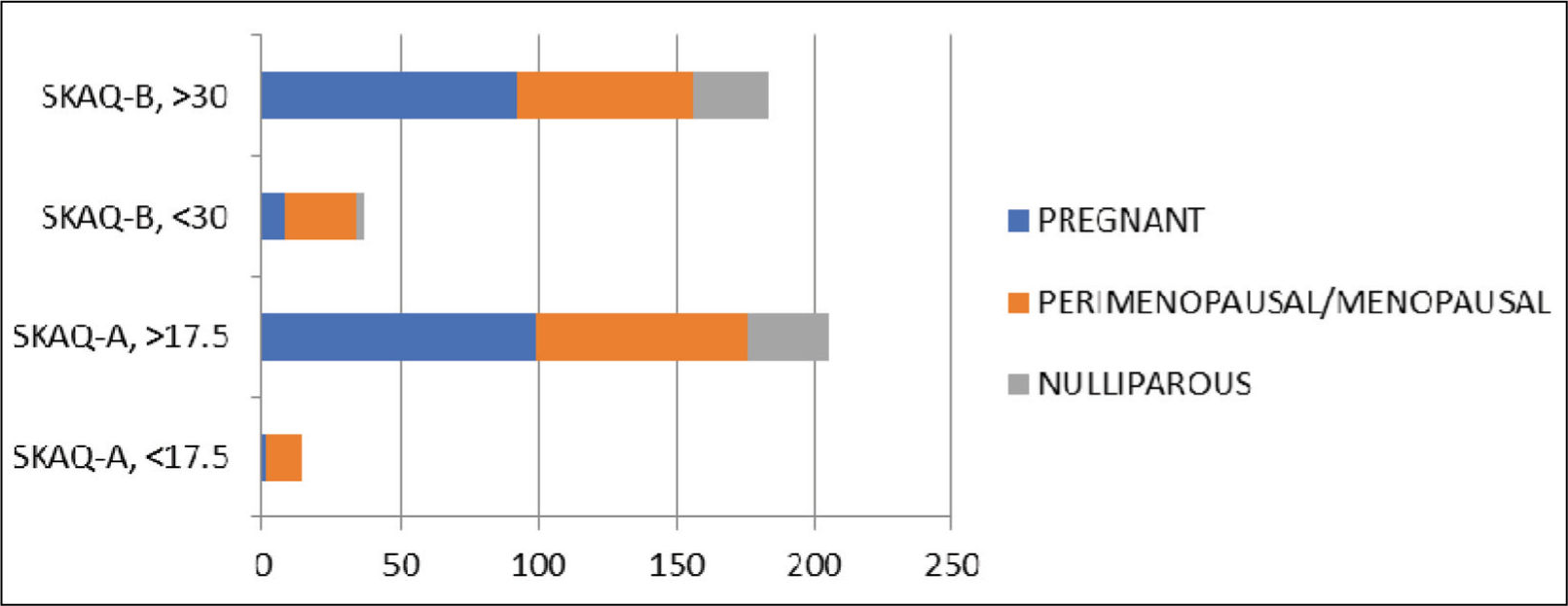
In the SKAQ-A part, pregnant women having good knowledge about sexual practices were 99% of the total 100 women; all of the nulliparous women scored >17.5, and 14.4% of the menopausal women had proper sexual knowledge. In the SKAQ-B section, 92% of pregnant women had liberal attitudes, whereas 92% of nulliparous and 71% menopausal/perimenopausal women had liberal views about sexual practices (Figure 1). Statistical correlation showed that sexual knowledge and attitudes did not have any association with the current obstetrical/gynaecological status.
Correlation Between SKAQ and Obstetrical Status. 13
Of the women having a rigid attitude towards religious practice, 17.07% scored below 17.5 on the SKAQ scale, whereas 82.9% of rigidly religious women had a higher score on sexual knowledge. 16.66% of women with moderate religiosity and 25.92% of women having not a rigid attitude towards religious practice had lower sexual knowledge, whereas 71.42% moderately religious women and 74.07% of not rigidly religious women had good scores on the sexual knowledge scale. 36.58% of rigidly religious women, 5.95% of moderately religious and 3.70% of not rigidly religious women had lower scores on the sexual attitudes (Table 3).
Correlation Between SKAQ and Religious Attitudes. 13

Sexual Dysfunction
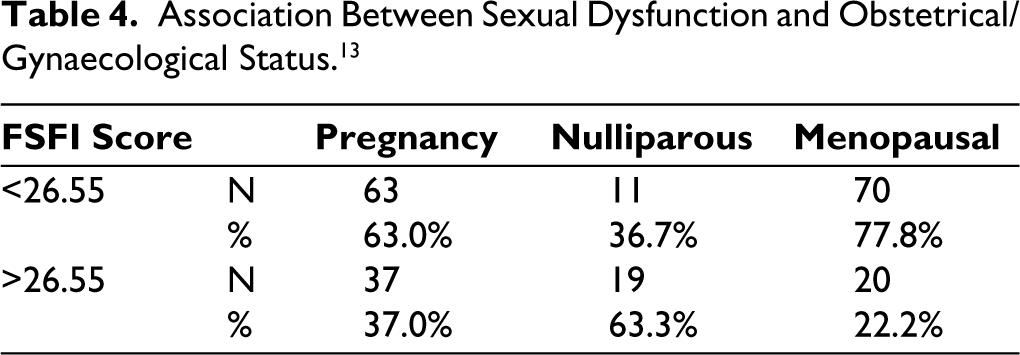
Out of 100 pregnant women, 63% reported facing sexual difficulties, whereas 77.8% of menopausal and 36.7% of nulliparous women reported sexual dysfunction as their scores were below 26.55 on the FSFI. However, sexual dysfunction did not show any statistically significant association with the obstetrical/gynaecological status (Figure 2) (Table 4).
Overall Prevalence of FSD. 13
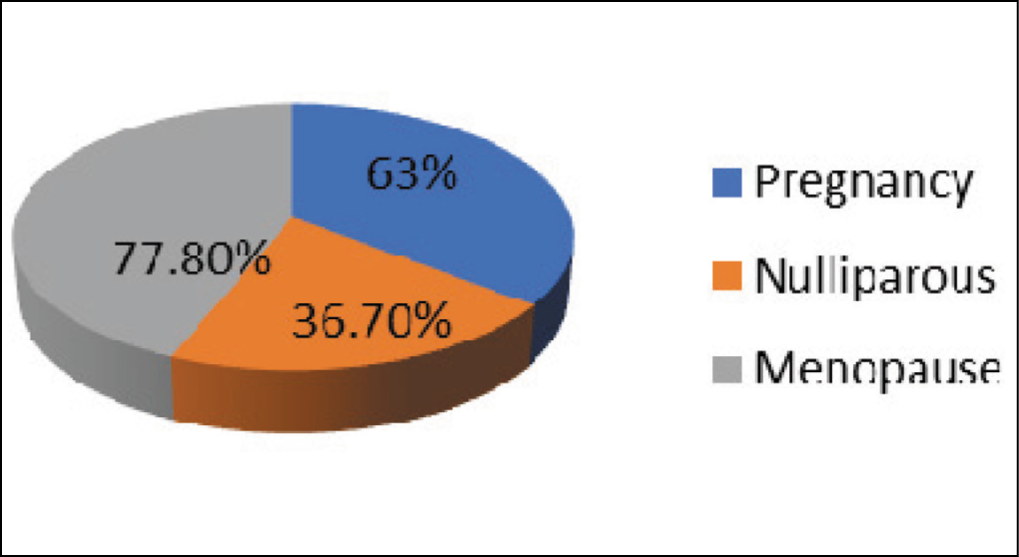
Association Between Sexual Dysfunction and Obstetrical/Gynaecological Status. 13
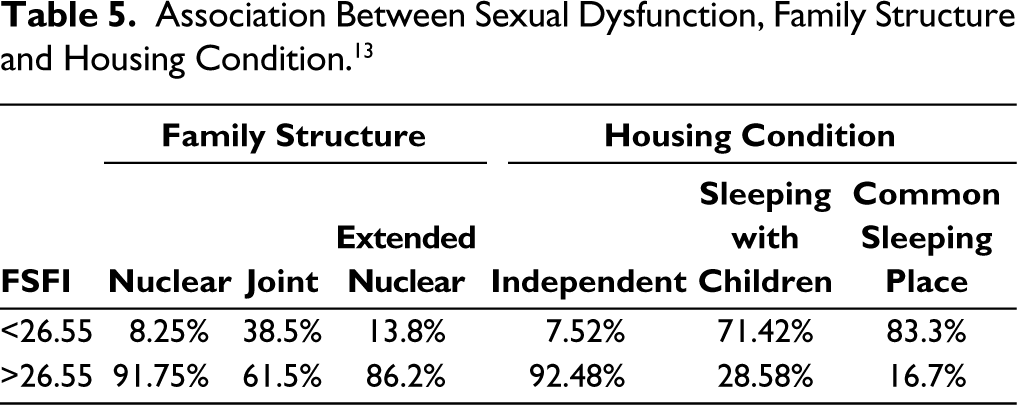
The study showed that out of the women who resided in nuclear families (n = 97), proportion of women who reported sexual dysfunction was only 8.25% as compared to 38.5% and 13.8% of women residing in joint (n = 58) and extended nuclear families (n = 65), respectively.
Out of 220 women, of those staying in independent housing conditions, only 7.52% reported having sexual difficulties as compared to 71.42% women having sexual dysfunction who were sleeping with children, and 83.3% women having a common sleeping place mentioned having sexual problems. Housing conditions showed a statistically significant relationship with the presence of sexual dysfunction (Table 5).
Association Between Sexual Dysfunction, Family Structure and Housing Condition. 13
Sexual Knowledge and Attitude Related to Sexual Dysfunction
It was seen that 9% of women having sexual dysfunction also had a low level of sexual knowledge, as compared to 1.3% of women having sexual dysfunction but with better sexual knowledge. 98.7% of women had a good level of sexual knowledge as well as adequate sexual functioning. Also, 22.2% of women reported having a less liberal attitude towards sexual practices along with the presence of sexual dysfunction, as compared to 77.8% of women who had a liberal attitude but faced sexual problems. Only 6.6% women having a conservative sexual attitude had satisfactory sexual functioning.
Of the 100 pregnant women who participated, the mean scores on the different domains of FSFI were 3.97 ± 1.14 for desire, 2.72 ± 1.50 for arousal, 3.47 ± 1.38 for lubrication, 2.58 ± 1.51 for orgasm, 4.11 ± 1.43 for satisfaction and 4.40 ± 1.71 for pain. The mean scores for the total 30 nulliparous women, on the other hand, for the six domains respectively were 4.24 ± 1, 4.22 ± 1.14, 4.23 ± 1.04, 4.08 ± 1.44, 4.78 ± 0.91, 4.86 ± 1.33. For the recruited 90 menopausal/perimenopausal women, the average scores on the domains of desire, arousal, lubrication, orgasm, satisfaction and pain were 3.40 ± 1.15, 3.18 ± 1.58, 2.64 ± 1.40, 2.21 ± 1.54, 3.00 ± 1.18 and 2.95 ± 1.92.
Pregnant women scored lesser on the domains of arousal and orgasm; whereas menopausal women had lesser average scores in the domains of lubrication, orgasm, overall satisfaction and pain.
Discussion
In this era of diverse and ever-expanding sexuality, the findings of this study are pertinent and surprisingly corroborate with those carried out by Avasthi et al. 17 in the 90s, who had initially devised and used SKAQ for assessing sexual health knowledge and attitude in North Indian Hindi-speaking women. In our country, where some religions do not even have a word to describe genitalia, and where the erotic aspect of even marital life is looked upon with a disapproving gaze, 18 it is presumed that knowledge and attitude towards sexuality would be looked from a sceptical lens. However, we found the majority of women to rather have accurate information about sexual health issues and an overall liberal mindset towards sexuality and sexual behaviours.
However, rural Indian women are likely to have a range of beliefs or misinformation about reproductive health, as well as insufficient knowledge, unscientific notions, and blind confidence in cultural taboos, myths, and social practices19,20; all of which can have a negative impact on sexual health, as seen in the study where hailing from a rural background was found to have a direct relationship with the prevalence of sexual dysfunction. A focused approach to educate these women and debunk their myths without being inconsiderate towards cultural beliefs must be tried by every healthcare professional.
Although in this study there seemed to be no significant association between religiosity and attitude towards sexual behaviour, previous Western studies21,22 established that the most significant predictor of women’s opinions about masturbation, abortion, homosexuality, pornography and sexual coercion was religiosity, particularly attendance at religious services or sermons. This finding was not present in our study, and this discrepancy could be explained by the difference in the type of religious preachings, religious practices and the varied religious culture found in India, which are more tolerant towards sexual practices.
The overall prevalence of sexual dysfunction was found to be 65.5%, of which pregnant women reported having 63% of sexual dysfunction. This study is in line with the one conducted by Singh et al. 23 where FSD was estimated to be around 66% and most likely to be encountered by obstetricians and gynaecologists rather than psychiatrists. Indian women are less likely to seek help from the latter for sexual dysfunction, and it is only when they go through a period of bodily change, such as pregnancy, that they meet a gynaecologist. This is mainly because for a large number of women, sexual issues are only considered a part of reproduction and many fail to understand their impact on mental health. McCool-Myers et al. 24 have conducted a systematic review and qualitative analysis and discovered that FSD has a significant impact not only on women’s sexual lives but also reproductive health, and that a variety of social, psychological and biological factors influence the prevalence of sexual dysfunction.
The prevalence of sexual dysfunction in the perimenopausal/menopausal age group was found to be even higher (77.8%), far more than sexual dysfunction encountered by men of the same age group. 25
According to the ground-breaking sexual response cycle that was created by Masters and Johnson 26 in pregnancy, for each trimester, difficulties in arousal, desire and satisfaction vary and are related to the body image concerns, fear of harm to the foetus and changes in sleep quality, leading to an overall decrease in pleasure and satisfaction.27,28
However, the domains affected in perimenopausal/menopausal women are consistently present for difficulties in lubrication primarily, followed by difficulty in orgasm, satisfaction and pain during intercourse. This can be prima facie due to a drop in oestradiol and age-related decline in circulating androgens, but more importantly, psychosocial determinants such as lack of self-confidence as a sexual partner, feeling ‘aged’ and presence of psychiatric co-morbidities should be taken into consideration.29,30 The prevailing thought in Indian society that menopause leads to the end of sexual life must be questioned by the healthcare professional, and sexual activity or interest must be normalised for the empowerment of these women.
It was concluded that one of the factors affecting sexual dysfunction was a lack of intimacy and poor communication with the partner, leading to a decline in interest in initiating sexual contact. This was also found by studies by Eryilmaz et al. 31 and Abouzari-Gazafroodi et al. 32 who established that the lack of personal space is an important contributing factor to the development of FSD.
This study also establishes that knowledge about sexual practices and a liberal sexual attitude might serve as a protective factor for FSD. Furthermore, having a good outlook and increasing one’s understanding of sexual matters can also have an impact on improving or growing sexual behaviours, regularity of sex, coping skills, and awareness of one’s spouse’s needs—all of which can contribute to couples experiencing sexual satisfaction. 33 In traditional Indian society, discussions about sex are often discouraged, leading to a range of problems, including ignorance, misconceptions and biased attitudes. This lack of openness can result in psychological conflicts, low self-esteem and distress, as well as high-risk behaviours. Individuals may also be more susceptible to physical or sexual abuse, unethical treatment and unsatisfactory interpersonal relationships. Despite its importance for overall health and well-being, sexual health is frequently overlooked at both the individual and public health levels. 34
Although this study highlights the importance of FSD with sexual knowledge and attitudes, it also has a few limitations. First, the use of self-reporting questionnaires and local translators may have led to bias, as there may have been underreporting or over-reporting of a few issues, or poor comprehension of the questionnaire. Second, being a hospital-based study, there may be a difference in the community prevalence as estimated and third, due to the ongoing COVID-19 pandemic, a larger sample size could not be taken. Fourthly, social desirability could also be a key factor for the underreporting of sexual issues.
The implication of our study would be to aid in public health interventions and sexual education programmes by focusing on women who are going through vulnerable transitions of life such as pregnancy and menopause so as to improve the sexual quality by enhancing sexual knowledge and enquire about their attitudes towards sex during their antenatal check-ups or during gynaecology consultations. Establishment of ‘Sexual health’ clinic along with Obstetrics and Gynaecology OPDs may serve the purpose of educating women on sexual practices during pregnancy, post-partum and menopause.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval obtained by Institutional Ethical Committee on 14.11.2019 prior to starting study at JSS Medical College, JSSAHER; Certificate number JSS/MC/PG/5189/19-20.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Informed consent was taken from the patients willing to participate in the study after explaining what the study is about and the extent of their participation.