
Abstract
The term compulsive sexual behaviour disorder (CSBD) involves a person’s excessive and recurring obsession with sexual fantasies, impulses and behaviours that are unpleasant for them and/or cause psychosocial harm. Due to the paucity of research on the topic, no specific guidelines are available for the treatment of CSBD, however, preliminary studies suggest a few options. This case report aims to discuss the management of a clinical case of CSBD that presented the increased number of sexual encounters with commercial sex workers leading to high-risk behaviours. After a detailed history and, physical and mental state examination, a diagnosis was established and management was done with a combination of pharmacotherapy and psychotherapy. A progressive improvement was noted over six months. The case report highlights the need for timely diagnosis and effective treatment, which can improve distress, dysfunction and overall quality of life.
Introduction
A continuous pattern of being unable to control strong, recurring sexual impulses or drives that result in recurrent sexual conduct accompanied by distress or severe impairment is known as compulsive sexual behaviour disorder (CSBD). It might entail fantasies and desires in addition to or instead of sexual behaviour. 1 The International Classification of Diseases 11th Revision (ICD-11) has developed new, precise guidelines for CSBD that make it easier to distinguish the condition from normal variations of sexual behaviour and differential diagnoses like increased libido in manic episodes or hypersexuality in frontal brain syndrome. 2 Since there are no epidemiological studies evaluating CSBD in populations, it is still uncertain how prevalent CSBD is among adults worldwide. A large percentage of those affected—at least 80%, according to a study, are men. 3 Even if they are unable to regulate their sexual behaviour, people with CSBD frequently identify that it is excessive. They may behave compulsively (plagued by intrusive, obsessive thoughts and driven behaviours) or impulsively (doing something without considering consequences and lacking control). Similar behaviours can have different meanings, motives and psychological functions for various individuals. Excessive sexual behaviour can stem from early attachment issues, unresolved trauma and inner conflicts. It can serve as a coping mechanism for emotional distress, reinforcing cycles of dependency and dysfunction.
Numerous detrimental outcomes, including STDs, unintended pregnancies, social isolation, low self-esteem, financial troubles and legal infractions, have been linked to CSBD. Furthermore, comorbid illnesses, including mood disorders, anxiety disorders, drug addiction, personality disorders and obsessive-compulsive disorders, are frequently present in people with CSBD. 4
Similar to substance use disorders, affective disorders or impulse control disorders, compulsive sexual behaviours can manifest in several ways and to varying degrees of severity. Quite frequently, the symptoms are not disclosed until they are specifically questioned about, and it might not be the main reason for seeking therapy.
The pharmacological management of CSBD has been explored; however, the majority of these findings are the product of case series, limited open-label trials or retrospective analysis. Selective serotonin reuptake inhibitors (SSRIs) are among the treatment options for CSB that have been studied the most extensively; citalopram, sertraline and fluoxetine in particular have strong evidence bases. 5 Naltrexone, an opioid antagonist, with doses ranging from 50 mg/day to 150 mg/day has earned some backing from existing evidence as have some mood-stabilising and anti-convulsant drugs like Topiramate. 6
Early research also suggests that psychotherapeutic techniques like cognitive behavioural therapy (CBT), acceptance, and commitment therapy, and marital therapy may help minimise the negative consequences of CSB. Motivational interviewing and conventional CBT have been used successfully in several cases, and the results have shown a considerable reduction in sexual behaviours as in the index case, including the frequency of sexual partners and the amount of time spent online during work hours. 7
Case Report
A 25-year-old unmarried male, diploma holder in mechanical engineering, working as a cab driver presented alone to outpatient services of a tertiary care hospital with illness of two years duration of acute onset and continuous fluctuating course. The disease was characterised by sudden irresistible urges for sexual gratification for which the patient started visiting commercial sex workers. As per him, there was a gradual increase in the time and money spent to acquire pleasure through such sexual encounters. Due to this, he neglected all other activities which were pleasurable to him earlier. He reported not being in any romantic relationship at the time of presentation. Apart from encounters with commercial sex workers, he also watched pornographic content available online for about one to two hours at night followed by masturbation when he was not able to visit commercial sex workers. Though he reported an urge to watch pornographic content as well the act did not give him as much sexual gratification as visiting commercial sex workers. His frequency of visits increased from three to four times per month initially to three to four times per week over five to six months. He would not use a condom or any protection during intercourse. Gradually he felt that his desire for sexual gratification was excessive and beyond his control as he was unable to focus on his academic and professional goals due to preoccupation with thoughts of acquiring sexual pleasure. Significant socio-occupational and inter-personal impairment was seen which led to intermittent low mood. He continued to experience an initial excitement during the anticipation of sexual intercourse which would perpetuate the cycle but soon to be followed by feelings of guilt and worthlessness following the encounters. He reported feeling trapped.
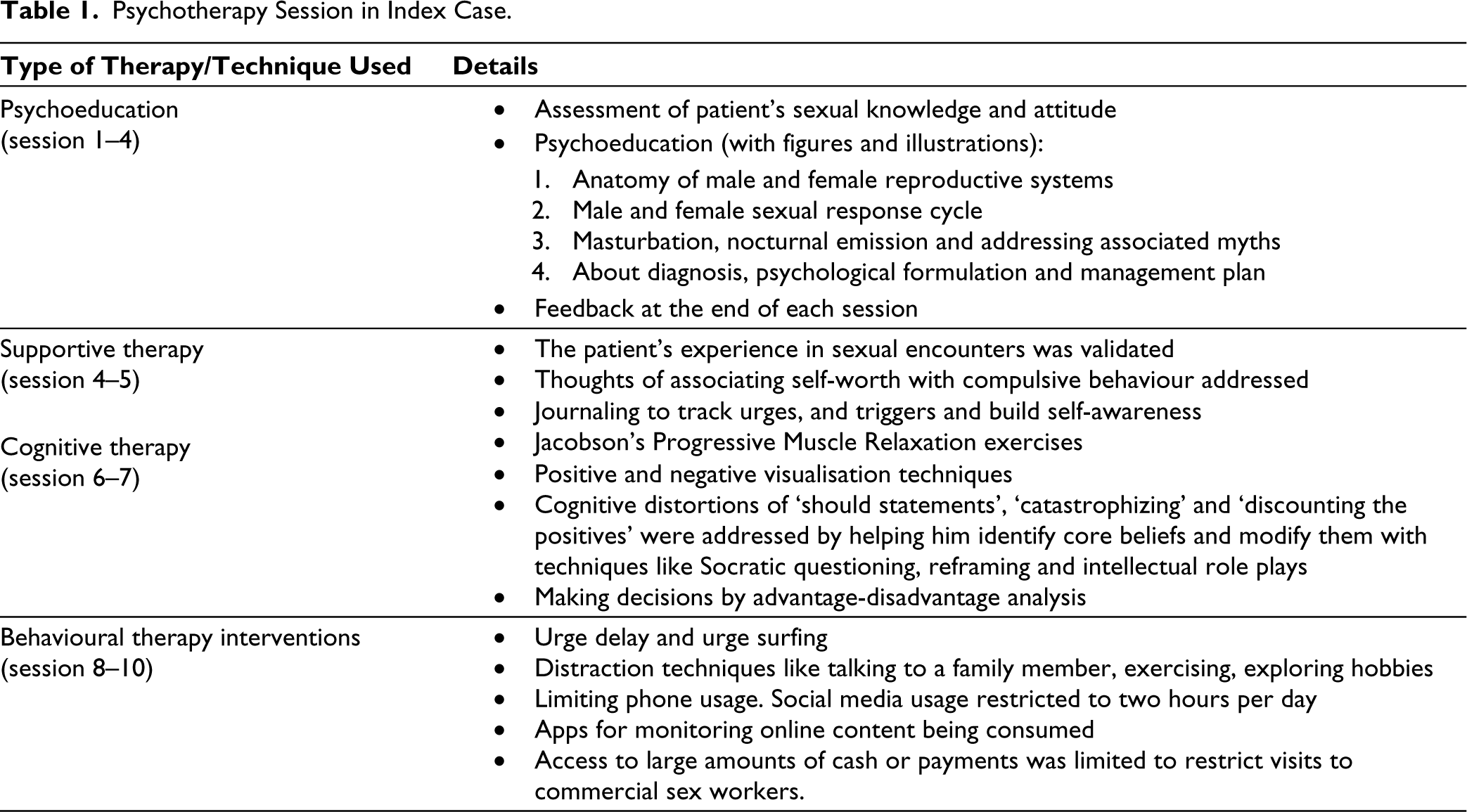
Other comorbid psychiatric disorders including substance use were ruled out and he denied having any family history of psychiatric disorders. As per him, he had never faced any legal issues. He fulfilled the ICD-11 criteria of CSBD which included engaging in repetitive sexual behaviour despite numerous unsuccessful efforts to control the same and adverse consequences. He also continued to engage in the same behaviour even when there was little satisfaction from it, thus, a diagnosis of CSBD was made and the patient was started on Tab. Fluoxetine 20 mg once daily and Tab. Clonazepam 0.25 mg on need basis. He was enrolled in supportive therapy sessions initially which later proceeded to behavioural therapy. Liaison was also sought from the Department of Dermatology given the complaint of lesions on genitalia which were diagnosed to be due to molluscum contagiosum. Adequate management was done for the same as advised by the Department of Dermatology. In psychotherapy sessions, initial focus was kept on psychoeducation regarding his diagnosis, and relaxation exercises were explained. Within two weeks of treatment initiation, he reported 20%–30% improvement. His urge for immediate sexual gratification had decreased and the patient was also able to include distraction techniques in his routine as explained to him in therapy sessions. He still engaged in excessive viewing of pornographic content followed by masturbation. Tab. Fluoxetine was increased to 40 mg/day and after another three weeks, the patient subjectively reported an overall 60%–70% improvement. His masturbation practice also decreased significantly and he was able to focus on his professional goals which led to improvement in self-esteem. He was then maintained on the same pharmacological treatment with regular therapy sessions as mentioned in Table 1, for identifying triggers and teaching behavioural strategies for impulse control and emotional regulation. Adding a cognitive element to therapy the focus was shifted on identifying underlying beliefs. In subsequent sessions, he was able to identify that the lack of a romantic partner made him feel inadequate and unworthy, and visiting CSWs had become a sort of reassurance seeking. Based on the clinical interview and therapy sessions, the index case had poor exposure to individuals of the opposite sex during his adulthood, including the absence of peer circles and adult females in his adolescence, which could have further led to communication deficits and anxiety in initiating conversations with females. He reported improvement evident by a decrease in his score on the compulsive sexual behaviour inventory—Baseline: 59/110; which reduced to 31/110 after six months of treatment and the Sexual Compulsivity scale—Baseline: 36/40; which reduced to 13/40 after six months of treatment. He also reported a decrease in obsessive preoccupation which was evident in the decrease in masturbatory practices, improvement in his ability to concentrate on his studies, and increased confidence in his ability to pursue a monogamous romantic relationship. The patient is regular in follow-ups and adhering to treatment for the last six months.
Psychotherapy Session in Index Case.
Discussion
Excessive sexual behaviour is a common clinical manifestation of several mental health issues, and it is critical to distinguish it from CSBD. Drug use, especially stimulants like cocaine, amphetamines as well as gamma hydroxyl butyrate (GHB), can also lead to excessive sexual behaviour. 8
CSB can be subdivided into three clinical elements: repeated sexual fantasies, repeated sexual urges and repeated sexual behaviours. 9 While many report feeling satisfied after engaging in compulsive sexual activity, shame or regret frequently accompanies these actions. 5 Subtypes of compulsive sexual behaviour can also be classified as paraphilic or non-paraphilic. Activities that are seen as being outside of the typical spectrum of sexual behaviour are referred to as paraphilic behaviours. Non-paraphilic behaviours as evident in the index case, include engaging in widely accepted sexual activities but with excessive frequency, such as masturbation, sex with commercial sex workers, browsing pornographic content or indulging in extramarital relationships. 10
The index case responded well to the first agent used, that is, fluoxetine, which in combination with psychotherapy possibly worked by reducing intrusive thoughts, making resisting compulsions easier, improving secondary depressive symptoms and underlying self-esteem issues
However, in the absence of solid guidelines and expert consensus, it is prudent to rely judiciously on pharmacotherapy, as the target is not to get rid of healthy libido, which could be a common side effect.
Current research on the treatment of CSB shows the need for more thorough controlled studies, even though it offers an informative place to start. When treating CSBD, the role of controlled and randomised approaches in conjunction with clinical case reports will be crucial as CSB research advances.
In the Indian context where open conversations about sex itself are generally taboo, it is imperative to explore reasons for distress and encourage healthy discussions regarding sexual disorders, so that people can seek help and not just continue to live in shame and guilt thinking that there is something inherently wrong with them and there is no solution to their problems.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
Not applicable.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent
Consent for research was taken from the index case as per the department protocol and anonymity was ensured.