
Abstract
Unsafe sexual behaviour among psychiatric patients is a critical intersection of mental health and sexual well-being. Risky sexual behaviours, defined as practices like unprotected sex or impulsive relationships under the influence of mental disorders or substances, pose significant health risks. Studies reveal a high prevalence (up to 80%) of such practices among individuals with severe mental disorders compared to the general population. Factors including impaired judgement, impulsivity and low self-esteem cause relationship challenges. Consequences range from sexually transmitted infections (STIs) and unintended pregnancies to social and relational conflicts. Prevention and intervention strategies such as cognitive-behavioural therapy (CBT), Dialectical behaviour therapy (DBT), routine sexual health screenings and integrated care approaches are essential. Addressing stigma, resource limitations, and cultural taboos are crucial for safer practices, ensuring patient autonomy and improving quality of life through multidisciplinary collaboration and patient-centred policies.
Sexual health is defined by the World Health Organization (WHO) as a state of physical, emotional, mental and social well-being in relation to sexuality; it is not merely the absence of disease, dysfunction or infirmity. 1 It requires a positive and respectful approach to sexuality and sexual relationships. Sexual experiences should be free of coercion, discrimination and violence and sexual rights must be respected, protected and fulfilled. 2 Sexual health is integral to individual, familial and societal well-being, contributing significantly to overall health and the socio-economic development of communities. 3
Risky sexual behaviour is inconsistent condom use with multiple sexual partners or having sex under the influence. 4 Risky sexual behaviour also known as unsafe sexual practices, high-risk sexual behaviour, unprotected sex, promiscuous behaviour, casual sex with multiple partners, condomless sex, sexual risk-taking and hazardous sexual practices.
Prevalence of risky sexual behaviour among severe mental disorders is very high, almost up to 80% compared with the general population. 5 The global age-standardised mortality rate (ASMR) and age-standardised DALY rate (ASDR) attributable to unsafe sex are 11.98 (10.97–13.52) per 100,000 people and 570.78 (510.24–658.10) per 100,000 people, respectively. The burden of unsafe sex in women has an even more serious impact. 6
The public health expenditure related to unsafe sexual behaviours primarily includes the costs associated with managing the health consequences of risky sexual activity, such as sexually transmitted infections (STIs) like HIV, unintended pregnancies, unsafe abortions and related healthcare services. The cost spent on the problematic sexual behaviour in the USA is on average $2,900–$3,500 per month per youth. 7
Despite its importance, the budget for managing unsafe sexual practices is not enough to address the problem.
The relationship between psychiatric disorders and unsafe sexual behaviour:
Certain psychiatric disorders are associated with heightened sexual drive, often referred to as ‘hypersexuality’, which can lead to unsafe sexual practices. Such as, individuals with bipolar disorder may show risky sexual behaviours during manic phases by impulsive decision-making and unprotected sex with multiple partners or strangers. 8 Some personality disorders (like antisocial or borderline), schizophrenia and substance use disorders can show increased sexual risk-taking. 9
The high-risk behaviour is often driven by impulsivity, impaired judgement caused by distorted thinking, and inflated self-esteem. The potential consequences of unsafe sex include increased risk of contracting STIs, unintended pregnancies, strained relationships and social conflict.
Psychological factors like low self-esteem, body image issues, and relationship difficulties complicate the challenges of sexual health in psychiatric patients. Synergistic effects of mental disorder (Depression, Anxiety and Substance Use) on unsafe sex have to be explored. 10
Risky sexual behaviour and substance abuse:
Studies in Portugal show risky sexual behaviour is present in drug-dependent patients. 11 In Nigeria, inconsistent condom use and multiple partners sex was reported under the influence of substance use. 12 Individuals with SUD are susceptible to contracting and spreading STDs, including HIV/AIDS 12 as they have a low health care utilisation rate and may miss opportunities for early diagnosis. 13
Chinese college students with mental disorders were found to have risky sexual behaviour. 14 Unsafe sexual behaviour was documented among psychiatric inpatients in the USA, Belmont Centre and Ethiopia.11,15 Unprotected anal sex was higher among Australian homosexuals identified with depressive disorders. 16 Unprotected Sex has been documented among adolescents with autism. 17
Existing Guidelines for Addressing Unsafe Sexual Behaviour Among Psychiatric Patients
Expression of Sexual needs is a basic human right. A systematic review highlights existing guidelines in certain European countries for training staff to impart sex education and provide contraceptives to institutionalised psychiatric patients. 18 However, guidelines are needed to address unsafe sexual behaviour among psychiatric patients, not just in psychiatric institutions but in Outpatient Departments in nations other than European countries, especially lower-middle-income group countries.
Opportunities and Challenges
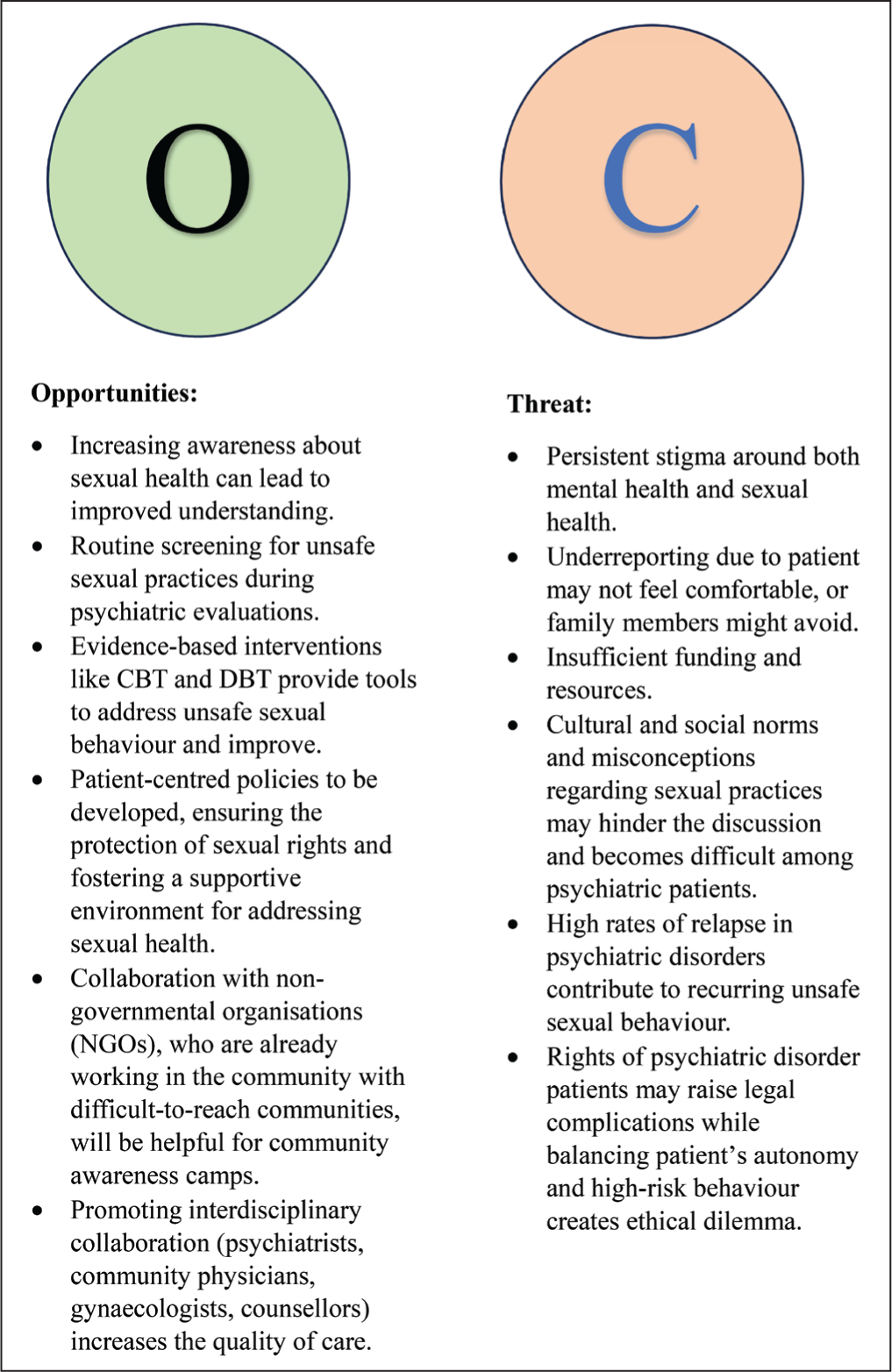
The intersection of sexual and mental health offers both opportunities and challenges. Addressing sexual health among psychiatric patients presents opportunities for integration of services, therapeutic advancements, and healthcare provider training. Enhanced awareness and multidisciplinary approaches can be taken to empower patients.
Key challenges include stigma, underreporting, cultural taboos, ethical dilemmas and legal issues. High relapse rates in psychiatric and substance use disorders exacerbate risky sexual behaviour.
Comprehensive strategies, including education, integration of services and new policies, can enhance care. Overcoming barriers like stigma, system constraints, and cultural taboos requires a coordinated, multidisciplinary effort. Opportunities and challenges have been shown in Figure 1.
Opportunity and Challenges Analysis.
Prevention and Intervention Strategies
The following strategies can be taken for combating sexual health among psychiatric disorder patients. 19
Sexual health education.
Routine screening of sexual health-related problems.
Addressing underlying psychiatric issues and building self-awareness.
Addressing medication side effects through consultation with psychiatrists.
Integrating sexual health counselling with mental health.
Psychotherapeutic interventions can be done in the form of cognitive behavioural therapy (CBT), motivational interviewing and dialectical behaviour therapy (DBT). CBT helps to identify and modify negative thoughts and behaviours related to sexual decision-making, while DBT develops skills for managing emotions and improving interpersonal experience.
Periodic training for health care workers.
Clear policies to be developed.
Individualised approach to be taken with sensitivity and collaboration with different specialists.
Conclusion
Sexual health is a fundamental aspect of overall well-being, and its intersection with mental health deserves significant attention. This article addresses unsafe sexual behaviours among psychiatric patients, which requires a multidisciplinary approach. Adopting a holistic approach is highly recommended for safer practices, protection of the rights of individuals and for the betterment of their quality of life.
Footnotes
Authors’ Contribution
All authors have a role in drafting and revising the viewpoint.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
Not applicable.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent
Not applicable.