
Abstract
This study aimed to investigate the association between impulsivity, craving and risky sexual behaviour in Brazilian substance users. Substance-use disorder, according to the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5), now features ‘craving’ as an essential criterion. Moreover, the intensity of craving and emotional dysregulation are factors considered pivotal to addressing risky sexual behaviour. Similarly, adverse childhood experiences, trauma, impulsivity and mental health conditions are considered to correlate to risky sexual behaviour. Research to date has focused on adolescent or student populations. A cross-sectional study design was utilised. The 135 participants were receiving treatment for substance-use disorder; the instruments used included the Barratt Impulsiveness Scale-11 (BIS-11), Sexual and Risk behaviour scale and the Behaviour Scale Crack Craving Questionnaire (CCQ-B) scale. Data was inputted into SPSS and analysed using the Pearson chi-squared test. The results included statistically significant correlations between craving and risky sexual behaviour, exposure to violence and risky sexual behaviour and perceptions of sexual addiction/ compulsion as being more of a problem than substance use. No statistical significance was found between socio-economic demographic data and risky sexual behaviour, or the primary substance and risky-sexual-behaviour. The limitations of the study were the small sample size, only male participants and language barriers. Implications for practice centre around synergising mental and physical health promotion via more proactive educational campaigns and accessible, equitable interventions. The study investigated the association between impulsivity, craving and risky sexual behaviour in Brazilian substance users receiving treatment. There were statistically significant correlations between craving and risky-sexual-behaviour, exposure to violence and risky sexual behaviour and a perception that sexual addiction/ compulsion is more of a problem than substance use.
This project explored the impact of impulsivity, craving, depression and risky sexual behaviour on Brazilian substance users. The working hypothesis was that substance users would be more likely to experience heightened levels of craving, be more impulsive and partake in ‘risky sexual behaviours’.
Craving is defined in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) as an ‘intense desire’ or ‘urge’ for a substance. Craving is a significant predictor of relapse. 1 Understanding craving may, therefore, be fundamental to helping inform implications for practice, for example, screening and treatment programmes. Craving is associated with the neurotransmitter dopamine and the prefrontal cortex region of the brain. 2 Substance use may increase levels of dopamine, yet damage prefrontal cortex functioning. 3 The prefrontal cortex helps regulate executive functioning, for example, attention, cognitive processing, working memory and inhibitory control. 4 Defects in this affect the ability to focus, retain information, think ahead, problem-solve and make rational decisions.
Risky decision-making among people with substance use disorders is commonplace. 5 Risky behaviours, including risky sexual behaviour, are dependent on the context and culture in which they are embedded. Nonetheless, sexual behaviour which is considered ‘high risk’ universally seems to constitute unprotected sex (sex without a condom), involvement with multiple partners and that which increases the likelihood of sexually transmitted infections (STIs). A strong correlation between substance use and unprotected sex is documented. 6
Aside from risky sexual behaviours being connected to substance use, with attendant physical and mental health concerns, crime and violence often were caused by substance use, 7 and there is a strong correlation between exposure to violence and substance use, as well as weapon carrying and aggressive behaviour. 8 Substance use may form a means of escapism, to counteract or distract an individual from dealing with negative emotions or experiences which they are finding difficult to accept 9 ; however, suppressing these emotions simply causes emotional dysregulation. There are greater levels of emotional dysregulation that were present in individuals with sexual addiction. 10
The consequences of not addressing issues with craving and substance use can lead to jeopardised decision-making and cause individuals to put themselves in risky situations, for example, unprotected sex. Developing a better understanding of this phenomenon may help identify priorities for future public health intervention.
Background
The World Health Organisation’s (WHO) Comprehensive Mental Health Action Plan 2013-2030 11 strives to promote more effective, community-based mental health and social care provision worldwide. The importance of positive mental health in enabling people to achieve their potential, actively participate, feel valued within their local community and develop the resilience to cope with challenging situations has been recognised as a global priority. However, stigma and discrimination are commonplace with individuals with mental health conditions, especially in the Americas. 12 Many face poverty and homelessness due to difficulties in securing or maintaining a job, so are vulnerable and often excluded within their local communities; high rates of substance use become comorbid with mental and physical health conditions. 13
The Pan American Health Organisation’s (PAHO) report, ‘A New Agenda for Mental Health in the Americas’ 12 acknowledged under-resourced, inequitable mental health provision, juxtaposed by significant increases in mental health and substance-use disorders (SUDs). Economic instability, fuelled by unemployment and poverty during the pandemic, resulted in the needs of many being unmet through the pandemic. PAHO 12 provided recognition that the transformation of mental health systems and services had to be prioritised as a matter of urgency. The process of improving and extending community-based mental health services began by integrating mental health within primary healthcare. Services aimed to be culturally relevant, with digitalised intervention emerging and holistic psychosocial support helping service users, as well as their families. Franca et al. 13 argued that delays in sourcing treatment can be burdensome not only for the individual and their family but also for wider society.
Brazil, the largest South American country, is sociocultural diverse. Each geographical region presents unique mental health needs and social issues. 14 Before the twentieth century, psychiatric asylums housed anyone considered socially ‘abnormal’; many with mental health issues were excluded from society. Therapeutic communities first emerged in the seventies, but it was only in 2001 that formal expansion of community-based services, aimed at reducing psychiatric hospital beds, became implemented. 15
In Brazil, the establishment of therapeutic communities has been controversial. 16 Whilst not a new phenomenon, originally the majority of these were linked to churches and were considered ‘recovery’ centres. These communities promoted abstinence, through health education, therapeutic activities and social support. 17 Brazilian community mental healthcare was further developed by the establishment of CAPS psychosocial care centres. Psychiatric treatment, psychosocial support and rehabilitation are central to the ethos of these centres. CAPS-AD provides outpatient community-based mental health support, whilst specialising in helping promote recovery from alcohol and other drugs (Centro de Atencao Psicossocial de Alcool e outras Drogas).
SUDs, including both alcohol and other drugs, are known to be complex and require multi-agency intervention. 18 Pierini et al. argued that community mental health provision for psychoactive substance users is typically less available, due to their unique needs; compared to those with other mental health disorders. 19 Regardless, 24-hour psychosocial care centres (Centros de Atencao Psicosocial) exist, including specialist substance-use centres (CAPS-AD III) for those in crisis. These are invariably located in the more impoverished areas ‘downtown’. Since the DSM-5 inclusion of ‘craving’ within the diagnostic criterion for SUD, 20 potential implications for more proactive intervention within the wider population might be worthy of consideration. 21 At present, there is a gap in the literature regarding the association between craving, impulsivity and risky sexual behaviour among service users with SUD.
The study aimed to investigate the association between impulsivity, craving and risky sexual behaviour in Brazilian substance users receiving treatment. The objectives of the study were to assess the type of substances used by participants, assess the links between substance use and risky sexual behaviour and explore the links between impulsivity, craving and risky sexual behaviour.
Method
The study used an analytical cross-sectional research design, 22 using a quantitative approach to identify correlations and associations between variables, providing a ‘snapshot’ 23 of a target population during a designated time. These variables were: impulsivity, craving and risky sexual behaviour.
Recruitment and Sampling
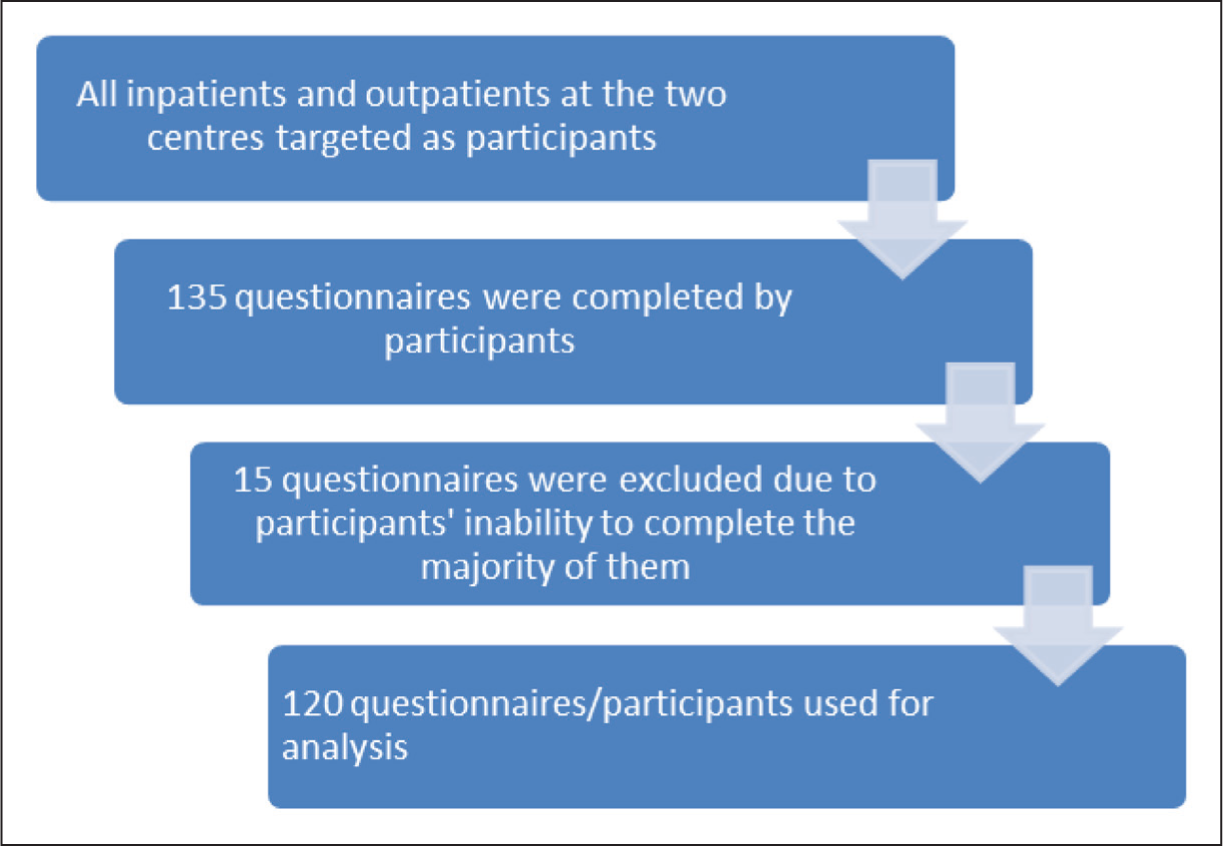
Data was gathered from 135 participants at two locations in Sao Paulo state, Brazil: CAPS-AD II (specialist drugs, alcohol community mental health centre) in Ribeirao Preto and Jaboticabal Therapeutic Community. One-hundred twenty sampled responses were relied upon for this study. Data collection occurred in two phases: Oct 2019-March 2021 and September-October 2023. Convenience sampling techniques were used; that is a convenience sample occurs when participants who fit a study’s criteria are enrolled in the study, sometimes by simply going to a location that is likely to have a large number of people who will fit the studies criteria, in this instance receiving treatment for substance use disorder. 24 No power calculation was done as convenience sampling used and all service users at the two sites were invited to participate.
The participants were all diagnosed with SUD, as defined by the DSM-5. All were 18 years old or older and without cognitive impairment, according to the Mini-Mental State Examination. 25 Exclusion criteria included anyone presenting as intoxicated, or experiencing severe substance-use withdrawal, for example, profuse perspiration, restlessness, extreme agitation, irritability, tremors, hallucinations, disorientated in time, place or person in line with the recommendations of WHO. 26
Data Collection
Participants adhering to the above criteria, at the two locations, were selected at random, according to their availability. Interview scheduling was determined by clinic management and the availability of a translation assistant. Each interview took approximately an hour and was conducted one on one. Confidentiality and privacy were maintained throughout.
The data collected was sociodemographic information (age, gender, marital status, sexual orientation, level of education, religion, occupation and income) and substance use (alcohol, cannabis, cocaine, crack, diazepam and others).
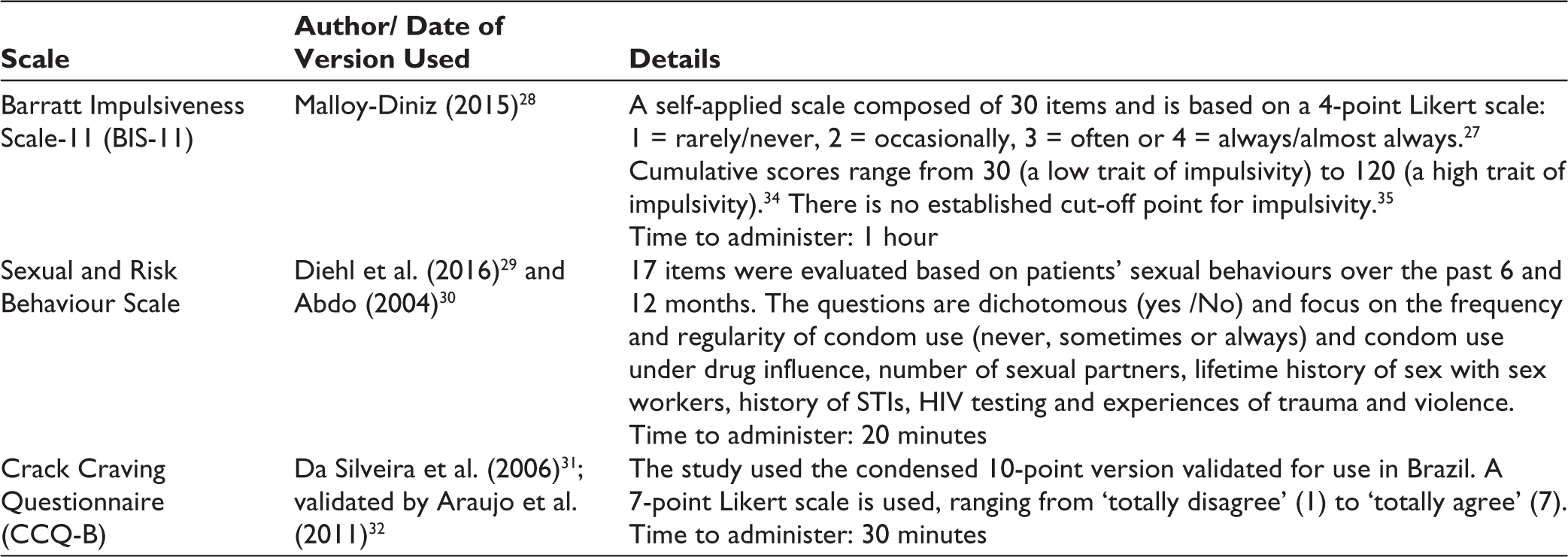
The scales used in the study were the Barratt Impulsiveness Scale-11 (BIS-11) 27 used to measure impulsivity using a version adapted to Brazilian-Portuguese 28 ; the sexual and risk behaviour scale 29 (based on Abdo’s work 30 ) was used to measure substance use and sexual behaviour and craving were measured using the CCQ-B,31,32 developed from the original CCQ-Now. 33
The standardised scales used in the study are shown in the table below:
Data Analysis
Data was inputted initially into an Excel spreadsheet and then coded in SPSS v.29. 36 Statistical analysis of the association between variables was then completed using the Pearson chi-squared tests of association and independence. 37
Ethics
Consent was sought at the start of each interview and each participant was made aware of their right to withdraw at any point. Whilst fulfilling ethical principles, the study also adhered to the Helsinki Declaration principles of 1964. Accordingly, approval was granted from the University of Birmingham Research Ethics Committee and the EERP- University of Sao Paulo Research Committee.
Results
There were 135 participants, but the study relied on n = 120 after excluding 15 woefully incomplete questionnaires. The dataset consisted of 120 people who were receiving treatment for substance use. However, only 113 responses were used because seven were incomplete (participants refused to answer certain questions).
While CAPS-AD provides treatment to both women and men, the participating therapeutic communities where the data was collected only offer treatment to men. So whilst the original intention was to gather data from both men and women, the data collection sites meant that only male participants were available.
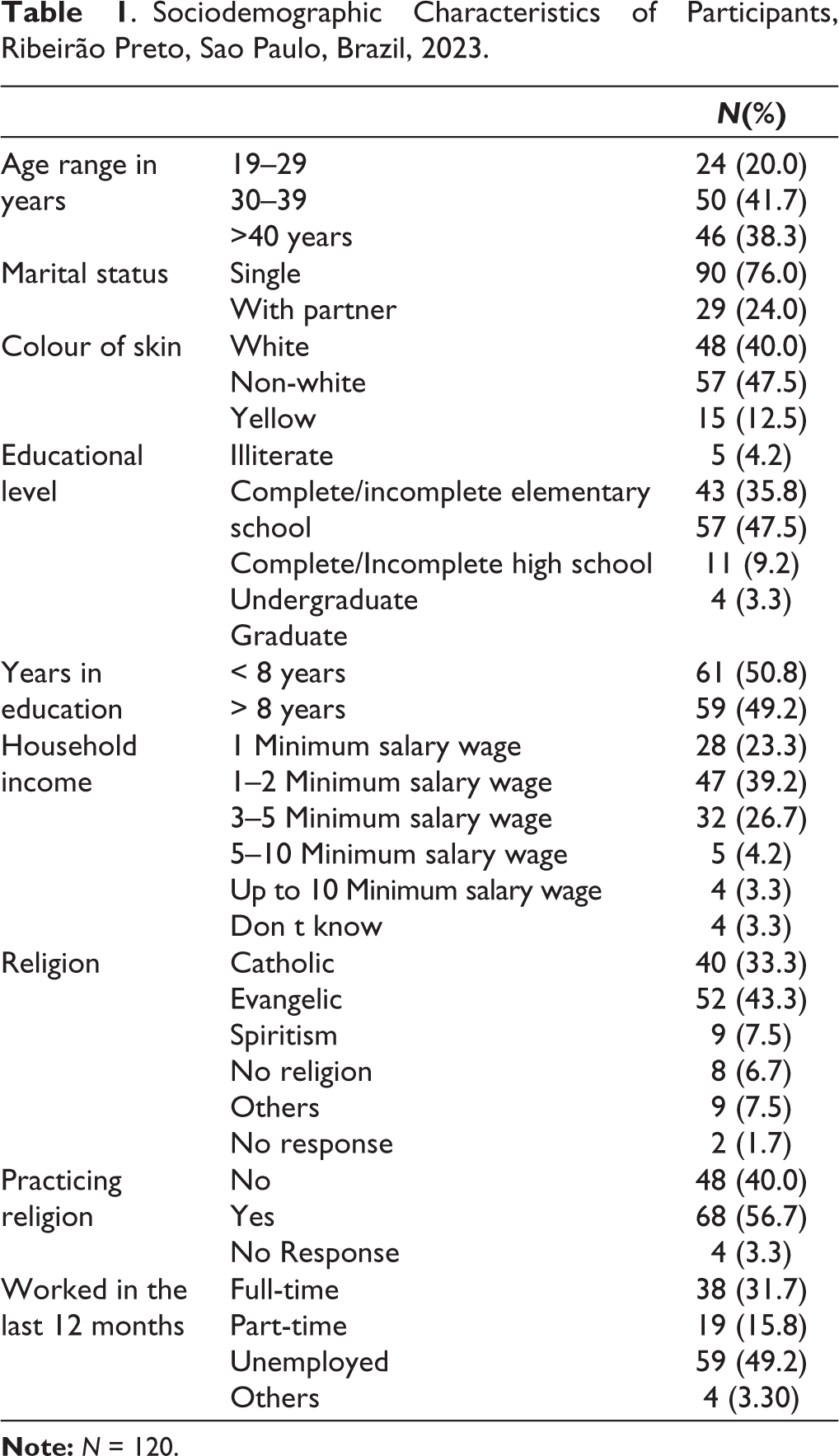
As can be seen in Table 1, 49 of these participants were 30–39 years old (43.3%). Most of these (68) were non-white (61.2%). The majority, 85, were single (75.2%). Fifty-five participants studied up to the end of high school (48.7%). Most, 52, considered themselves ‘evangelical’ (46.0%) in terms of faith, with 67 (59.3%) stating that they actively practice religion. Fifty-five participants (48.7%) stated that they were unemployed. Forty-four participants (38.9%) had a minimum salary wage of up to 2 MSW (R$ 2,640), per month (£414.37 – 1BRL = 0.1570 GBP 20/3/24 12:32).
Sociodemographic Characteristics of Participants, Ribeirão Preto, Sao Paulo, Brazil, 2023.
Participant Flow Diagram.
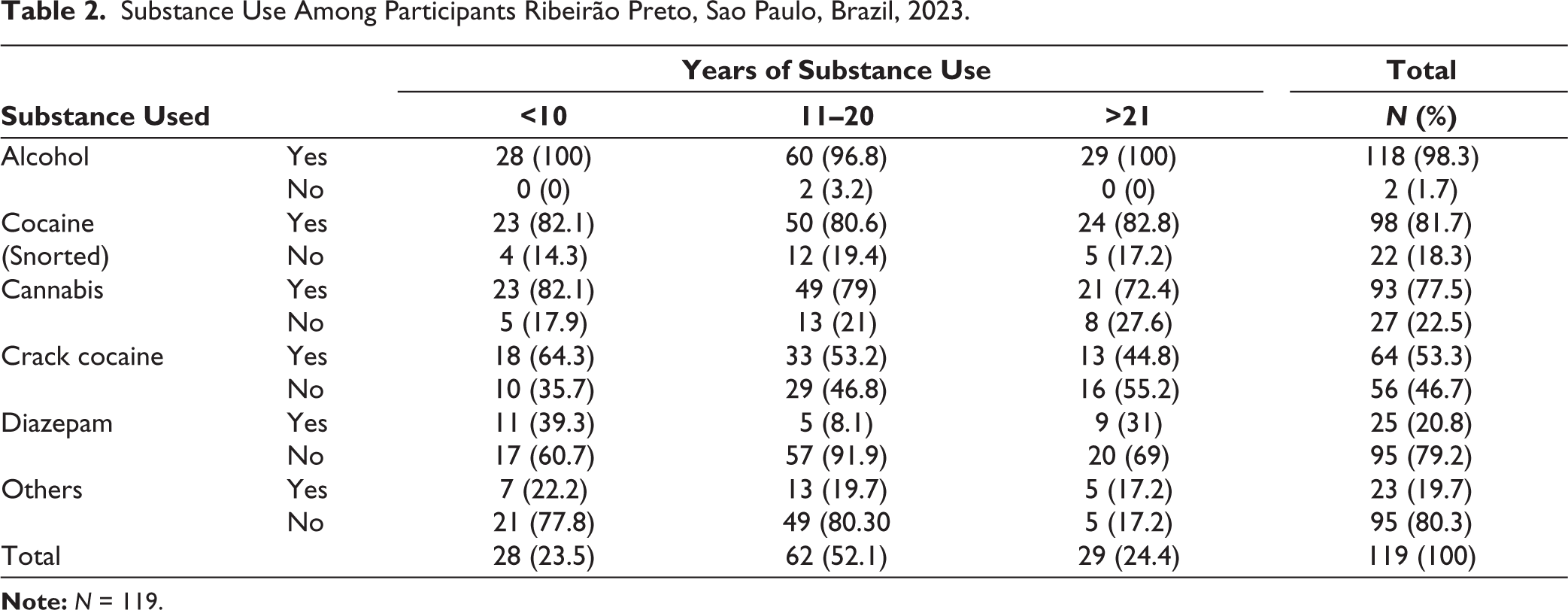
As regards substance use, Table 2, most of the participants (111) used alcohol (98.2%), followed by cocaine (96) with 84.9% and cannabis (90) with 79.6%. Participants who used crack were a much smaller percentage of the sample with 54.8%. Only 25 (22.1%) used benzodiazepines. Tobacco use was 100% among the participants. Most of the participants had been using substances for an extended period, using a substance/ substances for a mean time of 15.3 years (standard deviation (SD) = 7.4 years), ranging from 3 to 37 years.
Substance Use Among Participants Ribeirão Preto, Sao Paulo, Brazil, 2023.
The sample divided into two groups: those who considered themselves to engage in ‘high risk’ sexual behaviours—49 (40.8%) and those who considered themselves to engage in ‘low risk’ sexual behaviours—64 (53.3%). When making comparisons within the dataset, for ease of reference, these are presented as a homogeneous group.
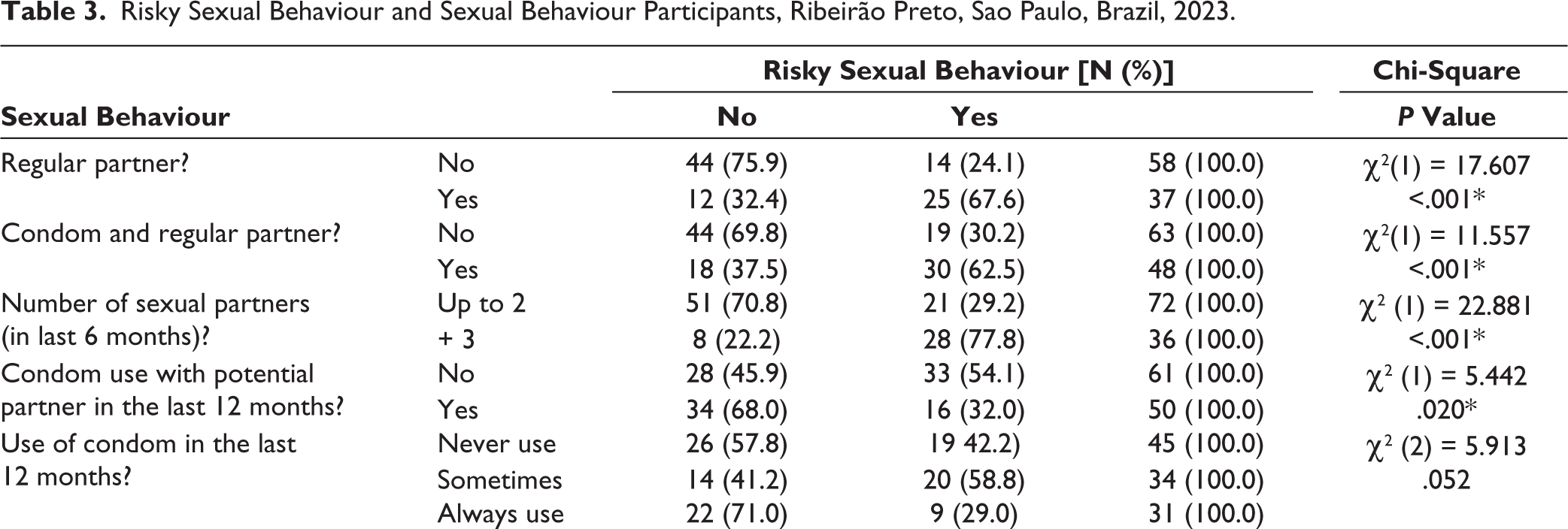
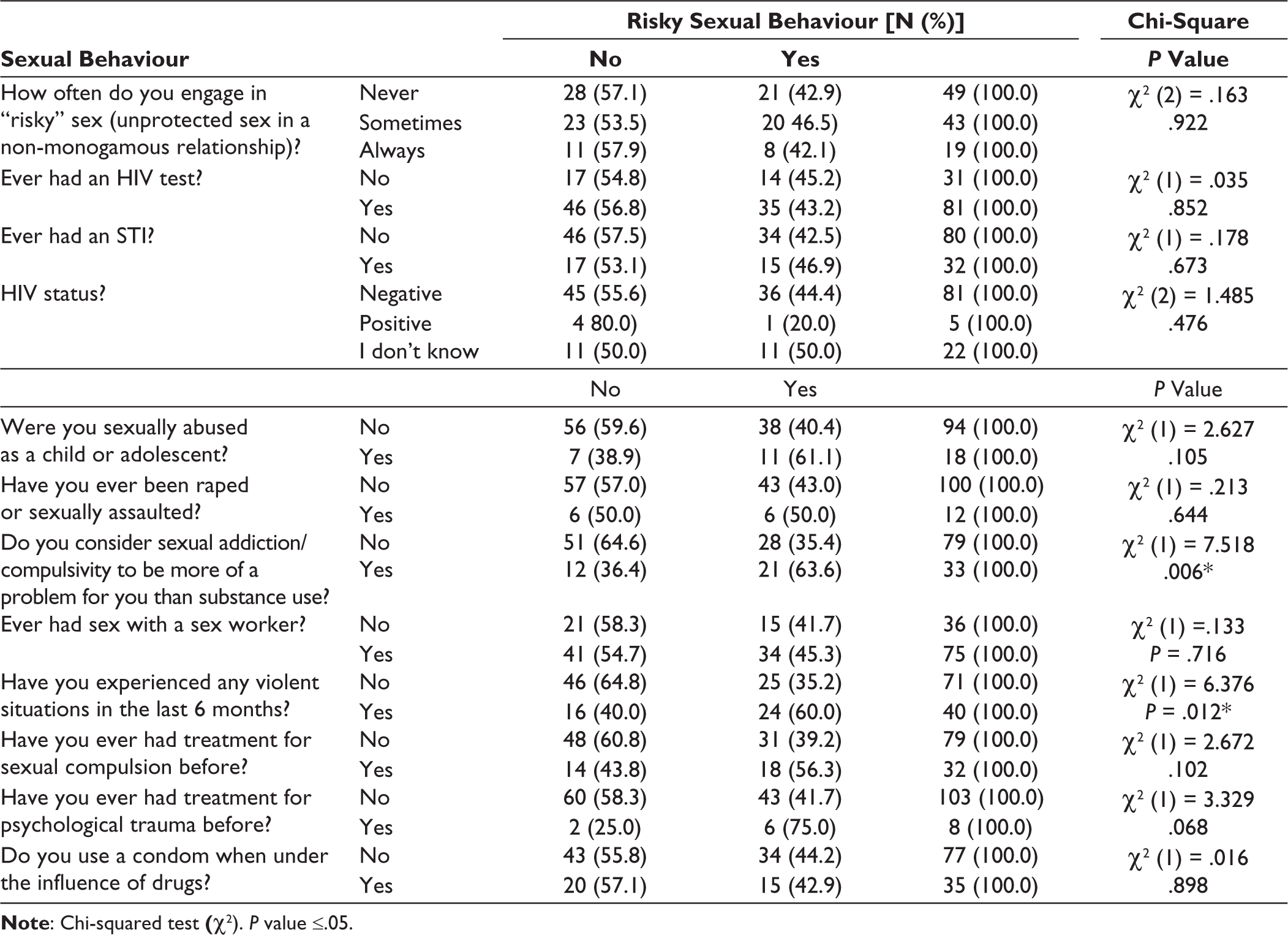
As can be seen in Table 3, a statistically significant P value (less than .05) is shown in terms of the following variables: regular partner, use of a condom with regular partner, number of sexual partners, condom use with eventual partner in the last 12 months, as well as frequency of condom use in the last 12 months. Also significant was that 21 (63.6%) considered their sexual addiction/ compulsivity to be more of a problem for them than their substance use; with a statistically significant P value of .006. Of importance too, was that 24 (60%) who had reported experiencing violent situations within the last 6 months, also had engaged with risky sexual behaviour; with a statistically significant P value of .012. Within the sexual and risk behaviours scale, violence was measured using Q23–Q25 and Q28.
Risky Sexual Behaviour and Sexual Behaviour Participants, Ribeirão Preto, Sao Paulo, Brazil, 2023.
Sociodemographic Factors and Risky Sexual Behaviour.
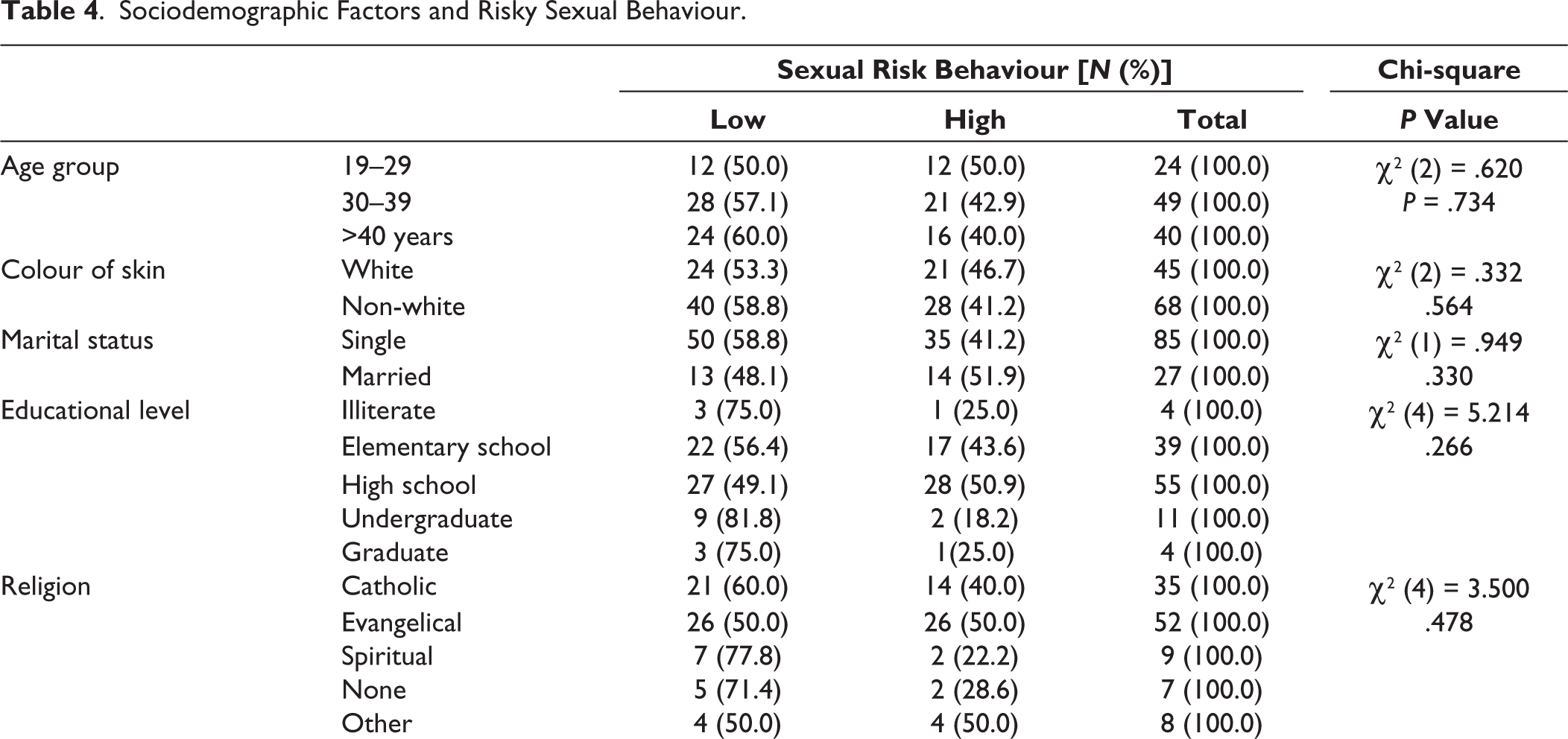
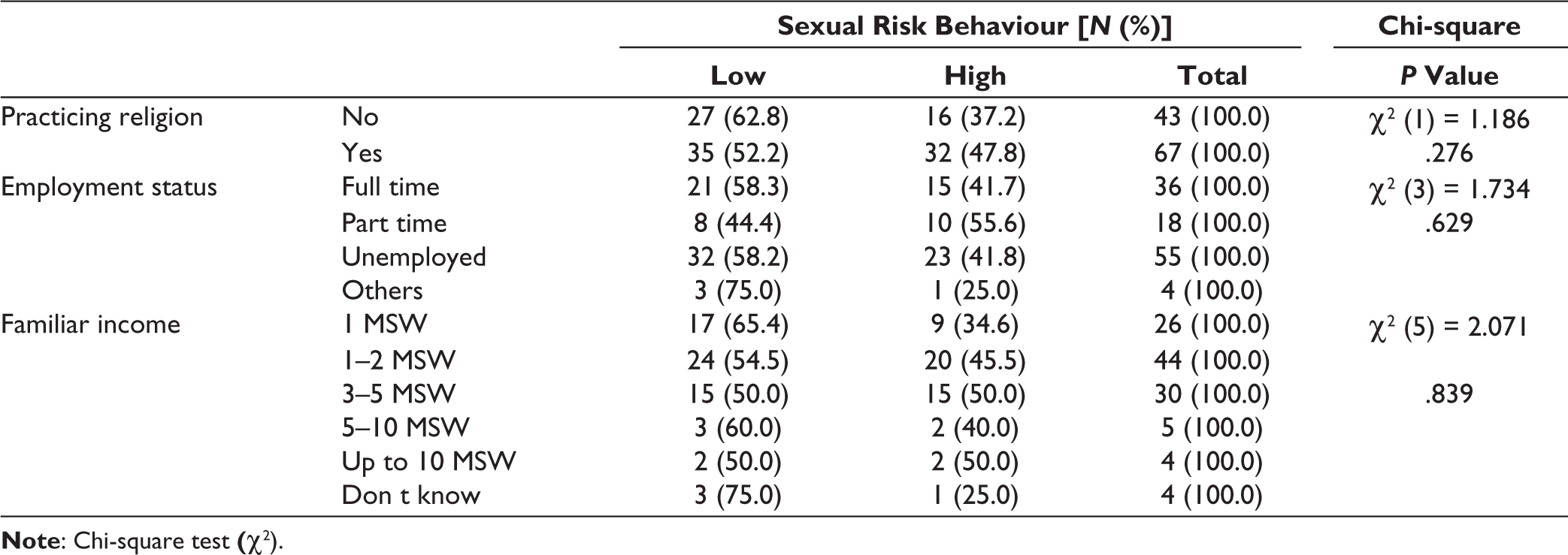
Those exhibiting high-risk sexual behaviours were younger (average 36.7 years and SD = 12.5 years), compared to those exhibiting low-risk sexual behaviours (average 38.5 years and SD = 11.7 years). However, this was not a statistically significant difference (P≥ .05). The results indicate that risky sexual behaviour is not determined by sociodemographic/ socioeconomic factors- the Chi-squared values for each element are not less than .05; that is, are not statistically significant.
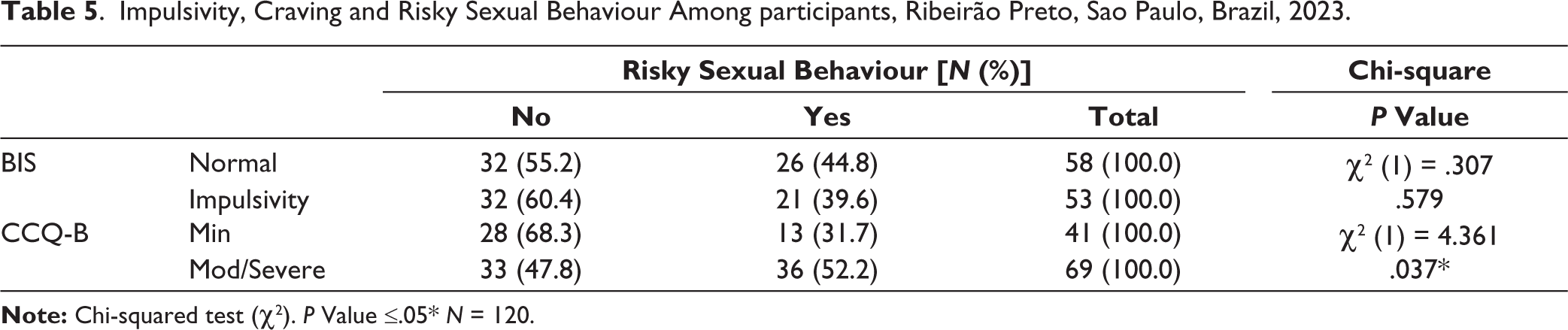
Table 5 highlights that there was no statistically strong association between levels of impulsivity and risky sexual behaviour. About 39.6% of people who considered themselves impulsive indicated that they engaged in risky sexual behaviour. About 44.8% of participants who considered themselves not to be impulsive, that is, in the ‘normal’ range of impulsivity, considered themselves to engage in risky sexual behaviour.
Impulsivity, Craving and Risky Sexual Behaviour Among participants, Ribeirão Preto, Sao Paulo, Brazil, 2023.
Risky Sexual Behaviour and Substance Use Among Participants, Ribeirão Preto, Sao Paulo, Brazil, 2023.

Nonetheless, in terms of craving, 52.2% of participants rated themselves as having moderate/ severe levels of craving and considered themselves to participate in risky sexual behaviour. This compares to 31.7% who rated themselves as having minimal craving levels (according to the CCQ-B). This indicates a P value of .037; which is statistically significant.
There were no statistically significant differences when comparing the type of primary substance used, in terms of risky sexual behaviours, with all P values being more than .05. It was observed that those with high-risk behaviours had been using a substance/ substances for less time (mean = 13.9 years, SD = 7.6 years) when compared to those with low risk (mean = 16.9 years, SD = 8.0 years), with statistically significant values (P = .024).
Aside from the formal research, it was evident that there was a sense of hope, acceptance and belonging in those attending the community centres. The research interview was motivating and felt culturally meaningful to the participants.
Discussion
This study aimed to investigate the association between impulsivity, craving and risky sexual behaviour in Brazilian substance users who attended CAPS-II and the Jaboticabal Therapeutic Community. Results indicated that there are statistically significant correlations between craving and risky sexual-behaviour, exposure to violence and risky sexual behaviour, and a perception that sexual addiction/compulsion is more of a problem than substance use.
The working hypothesis was that those with higher craving levels would be more likely to engage in risky sexual behaviour. All participants were male, the majority were 30–39 years old, non-white, single, high school educated, with a low income of up to 2 MSW (approximately £400) per month. Most participants reported engaging in risky sexual behaviour, but the socioeconomic and demographic factors were not statistically significantly correlated.
Individuals with substance use disorders are often unemployed, with financially limited recourse. 38 Formal employment can be difficult to secure, so many substance users rely on more accessible street-based work, such as informal recycling. 39 Others may turn to criminality. 29 Nonetheless, more affluent service users may simply pay for private substance-use treatment programmes; suggesting we interpret our sociodemographic data with caution. 40
Previous studies have focussed on the correlation between substance use and risky sexual behaviours of street children, adolescents and students/ young adults.41-43 However, when reviewing risky sexual behaviour within the context of substance use, definitions can be problematic due to differing expectations according to age, gender or culture. 44
As regards the primary substance used, alcohol was the preferred substance within the sample, closely followed by cocaine and then cannabis. Crack and benzodiazepines were the least preferred substances. Analysis showed no statistically significant connection between the specific type of primary substance used and risky sexual behaviour. However, this finding does not account for polysubstance use, which is commonplace among substance users. 5
While substance use and risky sexual behaviour are closely entwined 44 and there is a positive relationship between substance use and risky sexual behaviours, 45 there is no one specific substance that has been highlighted in the Brazilian population. However, alcohol (then crack cocaine) was the substance of choice in a Brazilian study into the characteristics of CAPS-AD service users, from where the study participants were recruited from. 40
A finding of statistical significance was that among the participants engaged in risky sexual behaviours had been using substances for less time. This was an unexpected finding, but perhaps the quantity of substance was higher when first taken, making risky sexual behaviour more likely. It is also possible that their responses were inaccurate or expressed what they assumed to be a suitable response. What is certain is that substance use tends to corroborate with risky/ irrational decision-making. 5 Brain imaging studies show increased abstinence from substance use results in increased volume in the prefrontal cortex, aiding cognitive functioning and regulating emotions, thoughts and behaviours. 38 Definitions of risky/irrational decision-making can be problematic due to differing expectations according to age, gender or culture. 46
Risk-taking behaviour may be perceived as normal for certain age groups, for example, adolescents. 47 However, the majority of our sample were aged over 30. Henceforth, it is fitting that those reporting high-risk sexual behaviours were younger; but in our sample, this was not to a statistically significant extent.
The majority of the participants who reported experiencing higher levels of craving (‘moderate/ severe’) also reported engaging in risky sexual behaviour, producing a statistically significant result. There is a lack of research investigating the relationship between craving levels and risky sex, or even risky behaviour in general. However, this finding addressed our working hypothesis about higher craving levels increasing the likelihood of participation in risky sexual behaviour. Whether levels of ‘craving’ are influenced by an individual’s personality/ natural disposition, or are simply a result of substance-use, warrants the question as whether ‘craving’ can be reduced to a manageable level, whereby it does not negatively impact upon decision-making and the ability to make rational, measured choices.
Recent research has suggested that sexual urges could be managed by regulating dopamine levels which are considered influential in addiction. Substance use can rapidly increase dopamine levels. 48 Additionally, executive function can be compromised by substance use. 49 Mestre-Bach and Potenza proposed that pharmacological treatment, for example, opioid receptor antagonists, SSRIs, or mood stabilisers, alongside psychological therapies, may be helpful in those with compulsive sexual behaviour disorder which corroborates the findings of this study. 48 The prevalence of compulsive sexual behaviour traits in patients with substance use disorders and highlighted the significance of addictive tendencies and emotional dysregulation. 50
Indeed, Morawetz et al. argued emotional regulation impacts the intensity of craving and the likelihood of relapse in those with SUDs, though they do not refer to risky sexual behaviours. 51 However, Wallace et al. evaluated the aetiologies of emotional dysregulation, personality and health-risk behaviours (including substance use and unprotected sex), in young adults. 51 They found emotional instability to be significant in health-risk behaviours, with personality traits, such as impulsivity, linking to compulsive substance use and risky sexual behaviour. 52
The importance of context in terms of risk-taking behaviour is emphasised by Wallace et al., 52 with factors such as trauma and social support being considered, as well as physical health conditions and medications being taken, to also be considered. Moreover, Chang et al. 53 suggested that targeting emotional regulation could help impulse control, giving individuals alternative coping strategies to cope with negative feelings and helping reduce alcohol cravings (which perhaps could be applied to other substances and risky behaviours, such as our focus here; risky-sexual-behaviour). Lew-Starowicz et al. 54 also argue emotional dysregulation is common in those engaging in compulsive sexual behaviour, which often is comorbid with substance use.
Ariesen et al. 55 examined ‘risky decision making’ in the context of alcohol-use disorder. Hereby, deficits in decision-making considered key to addiction may have detrimental consequences. A tendency to make ‘risky decision making’ could, of course, apply to risky sexual behaviour. ‘Risky decision-making’ may be linked to deficits in executive functioning. Understanding these connections, more importantly, could help prevent relapse in those with this- and possibly other forms of substance disorder. However, significant limitations of this study were acknowledged. Regarding the likelihood of participation in ‘risky sexual behaviour’, having a regular partner, three or more sexual partners in the last six months, and lack of condom use (never, or sometimes in the last 12 months) were amongst other statistically significant factors from analysis of our dataset. This finding did not present as particularly striking, or unusual; risky sexual behaviour via lack of condom use in people with a ‘regular’ partner seemingly contradicts the ‘finding’ that this is also attributable to those having multiple (3+) recent sexual partners.
A Brazilian population study found a lower prevalence of condom use in those in stable relationships and those aged over 35 years old, although these were not substance users, or not known to be. 56 Moreover, the same study noted markedly high STI rates, which they considered attributable to the fact that only a fifth of Brazilians used a condom. 56 Additionally, Reis et al. argued that substance use often precedes sexually risky behaviours, for example, instability and impulsivity; linking to compulsive substance use and risky sexual behaviour. 56
There were statistically significant associations between recent exposure to violent situations and participation in risky sexual behaviour. Research regarding the relationship between violence/ aggression and risky sexual behaviour in working-age adults is sparse, but the interrelation between risky behaviours, including exposure to violence, unsafe sex, alcohol, tobacco and illicit drugs, is well documented. 58 Both Monte et al. 58 and Reis et al. 57 studies were conducted on Brazilian adolescents. Increased drug trafficking, particularly of crack cocaine, was found to be another relevant factor in terms of exposure to violence. 59
Studies were examined substance use, domestic violence and unprotected sex, but different population groups (e.g., sex workers, teenagers, sexual orientation minority groups), or with other variables (e.g., during the coronavirus disease 2019 (COVID-19) pandemic, adverse childhood experiences) or locations (e.g., Mexico, Kazakhstan, Mozambique, Pretoria).60-63
In this study, a tangential statistically significant finding was that perceptions of sexual addiction/ compulsivity were more of an issue than substance use. A possible explanation for this might be regarding the stigma or sense of shame around sexual addiction/ compulsivity. Nayel et al. 64 found that there was a comorbidity between sexual addiction and SUD. Sexual addiction/ compulsivity may cause significant distress and disruption to an individual’s life, affecting relationships, career and social activities, consequently jeopardising quality of life (QoL). 64 Notwithstanding, substance users may already have compromised QoL, especially those who have experienced trauma, lack of social network support, or who are homeless. 65 .
Limitations
There were several limitations to the study. Our methodological cross-sectional design involved a relatively small sample, restricted to service users attending either CAPS-II AD, or the Jaboticabal Therapeutic Community. They were all male, mostly single and unemployed. There was no ‘control’ group; it would have been interesting to conduct the study with a more varied population, including women, substance users who were not accessing (and who had not previously accessed) treatment services, as well as those whose primary substance was not alcohol.
The sampling approach was simplistic, based on ‘convenience sampling’ 66 and only interviewing service users when available. The time when the research team had access to them was predominantly in the afternoons, which was when most of the service users were already scheduled to be in group therapeutic sessions. Thus, interviewing whoever happened to be available felt ‘ad-hoc’. ‘Purposive sampling’ might have been more efficient and beneficial. However, it has been argued that this form of sampling too presents challenges with generalisability to other populations. 67 Emerson 24 suggested this could be due to similarities in patients’ geographic socioeconomic and ethnic backgrounds; which could skew results.
The research team did not have access to details about any prescribed psychiatric or physical health medications, which might have included medication to help enhance sexual performance. Indeed, research has indicated that there is a connection between substance use, including prescribed psychiatric medication and sexual dysfunction. 62 Diehl et al. found that the relationship between substance use and sexual dysfunction may then catalyse low self-esteem, depression and poor physical health, symptoms which may perpetuate relapse. 29 A lack of identification of sexual dysfunction in substance users, perhaps due to healthcare professionals not necessarily taking an in-depth sexual history during consultations, only heightens dependence.
Additionally, without knowing service users’ likely complex backgrounds, possibly involving adverse childhood experiences and/ or trauma, we were unable to ascertain or explore individual triggers to craving and reasons for choosing risky sexual behaviour. Issues around financing substance use and economic vulnerability will likely accelerate risky- sexual-behaviours. Salazar et al. suggested economic hardship to be associated with increased risky sexual behaviour; propelled by substance use. 69 Nonetheless, their study participants were sex workers. Ekoh et al. found that substance use and risky sexual behaviour/ multiple partners provided trauma coping strategies. However, their sample comprised adolescents and young adults. 70
The study only collected quantitative data and qualitative data through focus groups, or semi-structured interviews, which would have allowed for a more in-depth exploration of certain responses. Such insight would have enhanced the results.
Nonetheless, the language barrier cannot be underestimated. At times, anecdotal information was overlooked, as the translation assistant’s time was limited, or they considered such information inconsequential.
Future Recommendations
Several statistically significant findings were made, of which the relevance of craving to risky-sexual behaviour, provides several implications for practice: In terms of harm reduction and relapse prevention, screening substance users for craving and emotional dysregulation at a much earlier stage may help minimise risky sexual behaviours. Ongoing health promotion in Brazil regarding substance use and safer sex within educational and community settings is needed. Training of a greater number of healthcare professionals to become confident with sexual health screening of substance users, integrated within regular physical health check-ups, also is necessary. Obtaining a thorough biopsychosocial history also appears salient to developing safer sexual behaviours and risk reduction on a public health scale. 71
The correlations between craving, substance use and risk-sexual behaviour are complex, whether dopamine levels, trauma, emotional dysregulation, poverty or other factors are considered instrumental. Further research is needed to unravel their complex aetiology. 72 Widespread stigma and discrimination surrounding substance use and mental health conditions remain in the Americas. 12 Holistic biopsychosocial assessments and proactive person-centred care are imperative. By developing healthier coping strategies, such as resilience, individuals are likely to be happier, more motivated, participate positively within their community, achieve their potential, economic stability and longevity; the goals of the achieving economic stability and longevity and achieving the goals of the Comprehensive Mental Health Action Plan 2013-2030. 11
As regards future research, the team will continue to investigate craving, impulsivity, substance use and sexual behaviour. As highlighted future studies with larger cohorts in different geographic locations would be beneficial, as well as looking at the needs of women and doing qualitative studies to develop a deeper understanding of the experiences of these vulnerable populations.
Conclusion
The study aimed to investigate the association between impulsivity, craving and risky sexual behaviour in Brazilian substance users who were in treatment. The results indicate that there are statistically significant correlations between craving and risky sexual behaviour, exposure to violence and risky sexual behaviour; and a perception that sexual addiction/ compulsion is more of a problem than substance use.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
The University of Sao Paulo and The University of Birmingham both provided Ethical Approval.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent
The participant has consented to the submission of the article to the journal.