
Abstract
Background:
This study was designed to assess the levels of and associations between gay-related stressful events, social support, emotional distress and the number of unprotected anal intercourse partners among Chinese men who have sex with men.
Methods:
Using a respondent-driven sampling method, 807 men who have sex with men were recruited in urban areas of northeast China and data were collected via face-to-face interviews. Gay-related stressful events were measured using the Gay-Related Stressful Life Events Scale; levels of depression, anxiety symptoms and social support were measured using the Self-Rating Depression Scale, the Self-Rating Anxiety Scale and the Social Support Rating Scale, respectively.
Results:
Over a quarter of study participants experienced gay-related stressful events during the preceding 3 months. Their average Self-Rating Depression Scale, Self-Rating Anxiety Scale and Social Support scores differed significantly from the national norm. Gay-related stressful events significantly correlated with anxiety (r = 0.167, p < 0.001), depression (r = 0.165, p < 0.001), social support (r = −0.107, p = 0.002) and number of unprotected anal intercourse partners (r = 0.13, p < 0.001), showing a clear dose–response relationship.
Conclusion:
Gay-related stressful events are common and are significantly associated with emotional distress, lack of social support and high-risk sexual behaviors among Chinese men who have sex with men. Multifaceted approaches are warranted to increase social support and reduce intolerance toward homosexual behaviors and to reduce risky sexual behaviors related to the rapid HIV epidemic among men who have sex with men population in China.
Keywords
Introduction
Many studies have documented that men who have sex with men (MSM) experience significantly higher levels of gay-related stressful events (GRSEs), such as discrimination, victimization, rejection and prejudice because of their sexual orientation, compared to heterosexual men (Huebner et al., 2004; Meyer, 2003). The accumulation of these stressors and a lack of social support have been found to lead to the development of psychosocial health problems (Mays and Cochran, 2001; Meyer, 2003; Rosario et al., 2002). These problems co-occur at high rates and interact synergistically, increasing the likelihood of behaviors associated with a risk of HIV, such as unprotected anal intercourse (UAI) (Mustanski et al., 2007; Semple et al., 2010; Wong et al., 2010). Advocates recommend the expansion of behavioral prevention methods to address the mental health context of at-risk MSM and to increase the efficacy and effectiveness of these programs (Crepaz et al., 2006; Herbst et al., 2005; Koblin et al., 2006; O’Cleirigh and Safren, 2007).
In China, despite relatively successful and cost-effective interventions to prevent HIV in at-risk MSM, the HIV infection rate increased rapidly, from 0.3% before 2005 to 13.7% by 2011, among 18 million Chinese MSM (Shang et al., 2012). This alarming spread may have been fueled, at least in part, by a strong stigma toward homosexuality in China, which may cause Chinese MSM to self-marginalize and conceal their sexual encounters, providing them with fewer social resources. The hidden MSM are afraid to seek out HIV information resources and testing or counseling centers and are unaware of their HIV status. When an individual who is hiding his sexual activity becomes infected and engages in high-risk sexual behaviors, HIV can spread among his partners in an ongoing cycle (Shang et al., 2012).
To our knowledge, no study has assessed the status of GRSEs and the associations between such events and emotional distress, social support and sexual risk behaviors among Chinese MSM population. The principal objectives of this study were (1) to assess the levels and characteristics of recent GSREs, social support, emotional distress and UAI behaviors among the Chinese MSM, and (2) to analyze the effects of GRSEs on sexual behaviors.
Subjects and methods
Site selection and subject recruitment
The locations of study areas and the selection of MSM have been described in detail previously (Yu et al., 2013). In brief, 807 MSM residing, working or living in four cities of Liaoning province, northeast China (Anshan, Benxi, Dandong and Shenyang), were recruited using a standardized respondent-driven sampling (RDS) procedure. Respondents were included if they had oral or anal sexual intercourse with another man during the previous 12 months and were aged between 18 and 65 years. Each subject was interviewed face to face by trained interviewers. Age, socio-demographic characteristics, sexual identity and disclosure of homosexual identity were noted using a structured questionnaire. No name or other personal information, such as an identification number, was recorded. The study protocol was reviewed and approved by the Institutional Review Board of the Liaoning Provincial Center for Disease Control and Prevention (LNCDCP).
Definition of variables
Gay-related stressful life events
GRSEs were measured using the Gay-Related Stressful Life Events Scale (Rosario et al., 2002), a 12-item scale that measures the occurrence of arguments with friends and relatives; parental, social and work conflicts; loss of friends; and victimization – all specific to sexual orientation – over the past 3 months. A total score was calculated by summing the number of items checked so that higher scores represented greater stress. Because the responses were skewed, we computed a response scale of 0, 1, 2 and 3 or more stressful events.
Anxiety and depressive symptoms
Subjective feelings of depression and anxiety during the previous week were quantified using the Self-Rating Depression Scale (SDS) (Shu, 1993) and the Self-Rating Anxiety Scale (SAS) (Wu, 1993), respectively. Each test consists of 20 items, each scored on a scale from 1 to 4 (never or occasionally, sometimes, often and most of the time). The item scores were multiplied by 1.25 to obtain a standard scale of 4–100, with scores ⩽53 on the SDS (Wang et al., 1999a) and ⩽50 on the SAS (Wang et al., 1999b) considered normal. The internal consistency (alpha) of SDS is 0.92. The correlation coefficient between SAS and Hamilton Anxiety Scale is 0.365.
Social support
Social support was measured by the Social Support Rating Scale (SSRS) (Xiao, 1999), which contains 10 items, measuring three dimensions of social support: subjective support (4 items), objective support (3 items) and support-seeking behavior (3 items). Item scores of the SSRS were simply added together, generating a total support score of 0–50, with higher scores indicating stronger social support. The SSRS has been used with a wide range of Chinese populations due to its high reliability and validity, with 2-month test–retest reliability of 0.92.
Number of unprotected anal intercourse partners
Respondents were asked about their sexual activity during the previous 6 months. Questions included the number of all male partners, whether they had engaged in anal insertive and/or receptive sex and the extent to which they had used a condom (never, sometimes, always, unknown) during the period, including casual partners and paid sex encounters. UAI was defined as ‘never’ or ‘sometimes’ using a condom during the previous 6 months. The number of unprotected anal intercourse partners (NUAIP) during the period was determined because it represents the level of high-risk homosexual activities related to HIV infection; there are other measures that can represent HIV risk behavior (e.g., serodiscordant condomless anal sex).
Statistical methods
Data analysis was conducted in SPSS, version 17.0. Analysis of variance (ANOVA) and Kruskal–Wallis test were used to compare mean values of SAS, SDS, SSRS and NUAIP by frequency of GRSEs. A standardized partial correlation coefficient was calculated to assess bivariate relationships between the number of GRSEs, SAS score, SDS score, SS score and the NUAIP, after adjusting for potential confounding variables (age, education, income, sexual orientation and HIV infection status [1/0]).
Results
A total of 807 MSM were recruited (Table 1). Their mean age was 27.2 ± 0.3 years, with 71.25% <30 years of age. Of these, 24.78% were married or cohabited with men, 40.27% were bisexual, 47.21% were gay and 12.52% were of heterosexual or unconfirmed sexual identity. We found that 22.92% had revealed their identity to their parents and wives as homosexuals, and 38.41% had engaged in UAI behaviors during the past 6 months, having an average of 2.19 ± 8.50 sexual partners. Their average SDS, SAS and SSRS scores were 47.29 ± 11.39, 40.66 ± 9.19 and 33.98 ± 7.46, respectively, differing from the national norms of 41.85 ± 10.57, 37.23 ± 12.59 and 40.12 ± 5.11, respectively (Wang et al., 1999a; 1999b; Xiao, 1999).
Characteristics of the 807 MSM sampled.
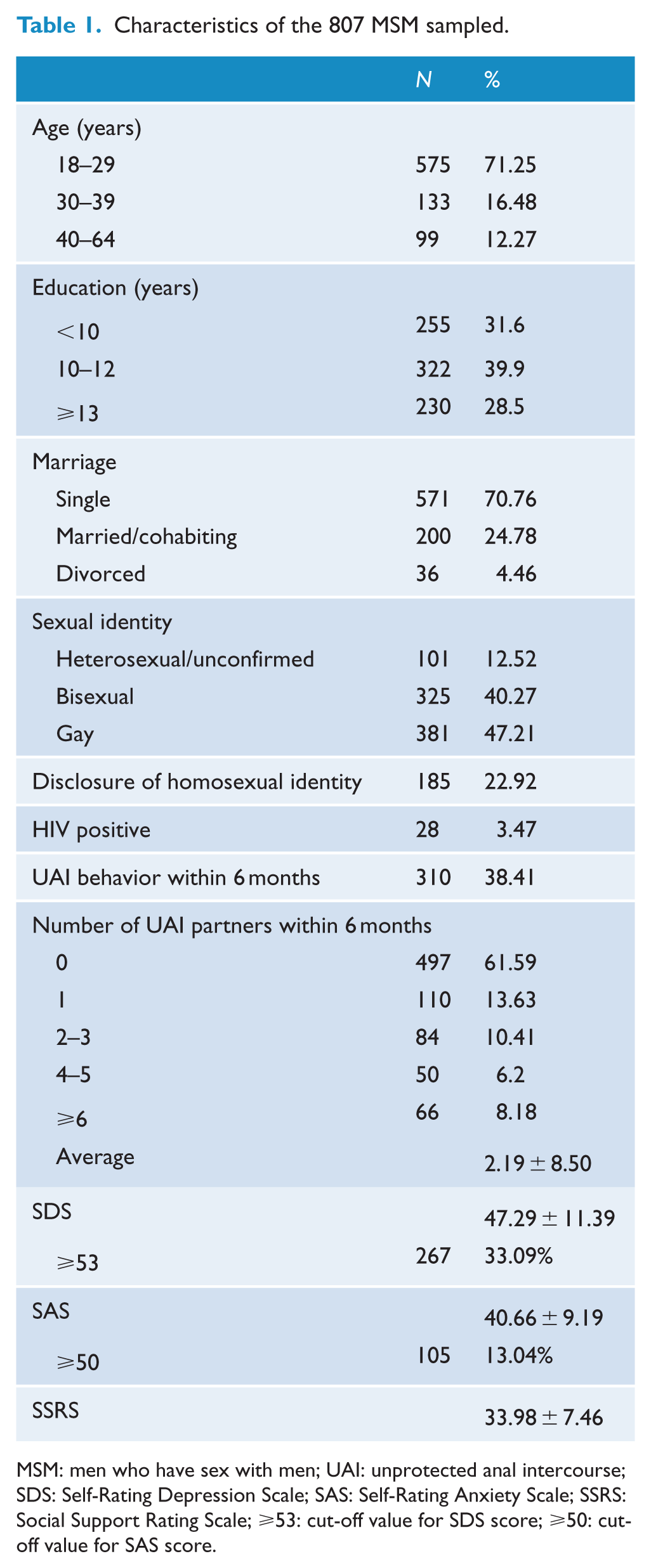
MSM: men who have sex with men; UAI: unprotected anal intercourse; SDS: Self-Rating Depression Scale; SAS: Self-Rating Anxiety Scale; SSRS: Social Support Rating Scale; ⩾53: cut-off value for SDS score; ⩾50: cut-off value for SAS score.
Table 2 shows that 26.02% of Chinese MSM experienced GRSEs during the previous 3 months, with 5.70% having two and 4.09% having three or more events. The top five events were arguments with close friends (11.28%), losing close friends (6.82%), arguments with parents (6.44%), arguments between parents (3.59%) and being physically assaulted (3.47%). The means of GRSEs were significantly higher in those who have disclosed their homosexual identity than those of non-disclosers.
Frequency of gay-related stressful events in the past 3 months among 807 Chinese MSM by status of disclosure of homosexual identity.
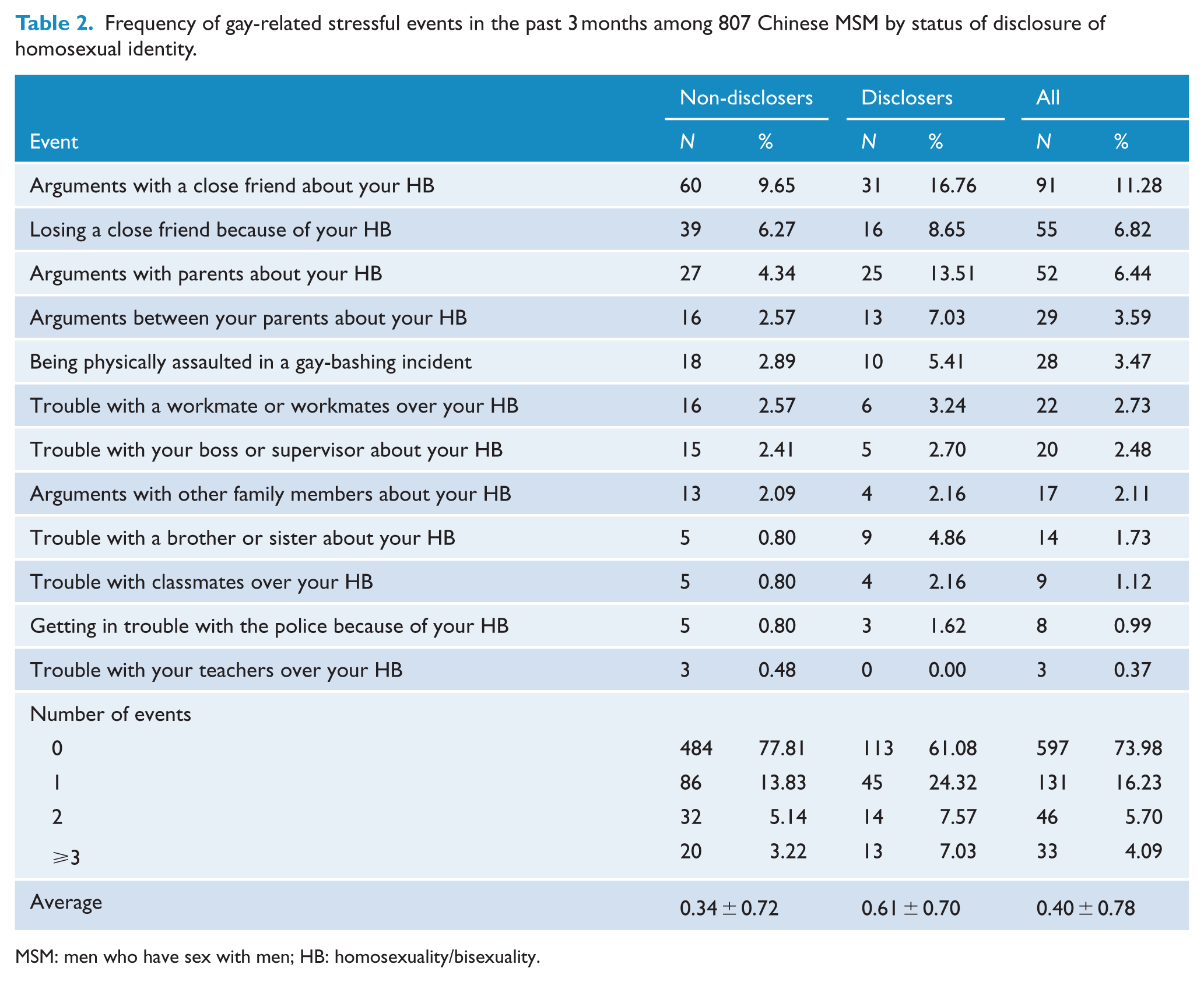
MSM: men who have sex with men; HB: homosexuality/bisexuality.
Table 3 shows that as the number of GRSEs increased, the NUAIP and the levels of anxiety and depression significantly increased while social support significantly decreased.
Average levels of anxiety, depression, social support and unprotected anal sexual behaviors relative to number of gay-related stressful events.
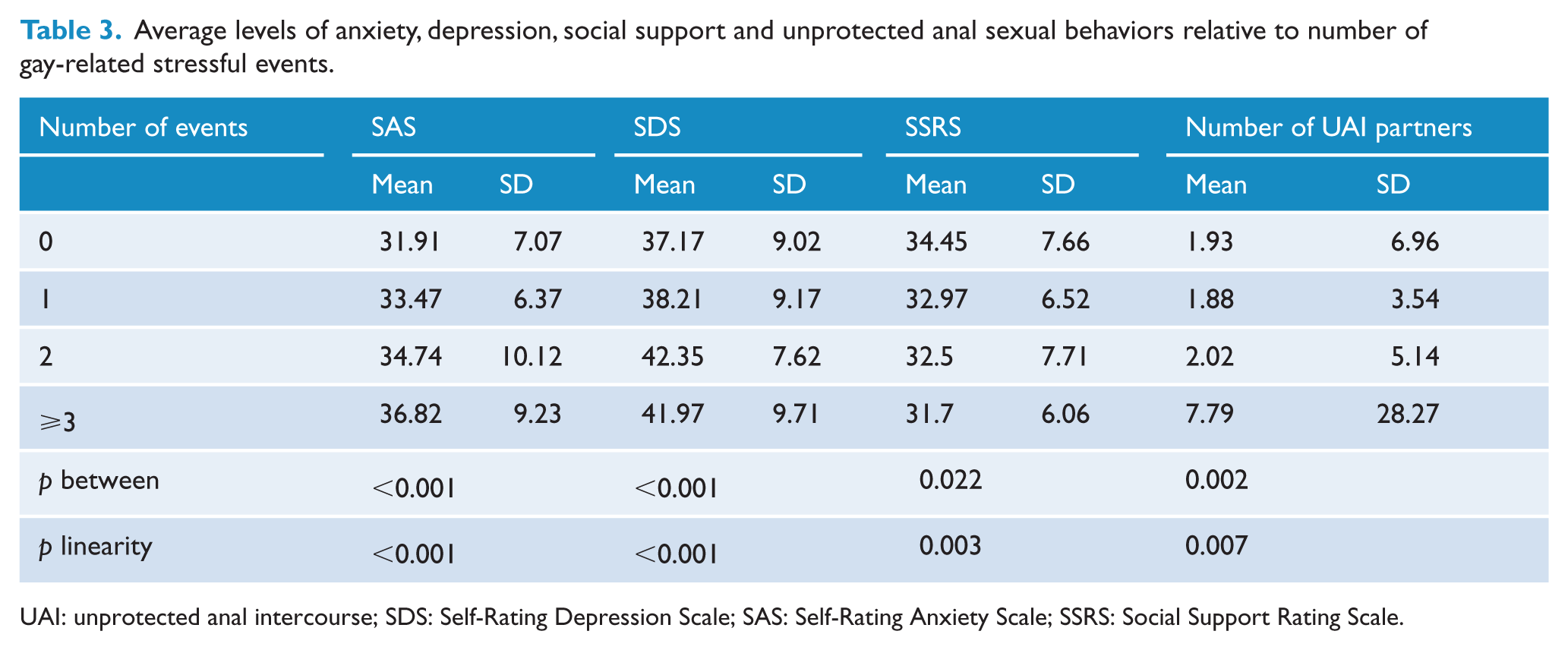
UAI: unprotected anal intercourse; SDS: Self-Rating Depression Scale; SAS: Self-Rating Anxiety Scale; SSRS: Social Support Rating Scale.
Table 4 shows the significant correlations among stressful events, social support, anxiety and depressive symptoms and the NUAIP. Stressful events correlated significantly and positively with anxiety (r = 0.167, p < 0.001), depression (r = 0.165, p < 0.001) and NUAIP (r = 0.13, p < 0.001) while correlating significantly and negatively with social support levels (r = 0.107, p = 0.002).
Standardized partial correlation coefficients between number of gay-related stressful events, social support and anxiety and depression scores among 807 Chinese MSM.
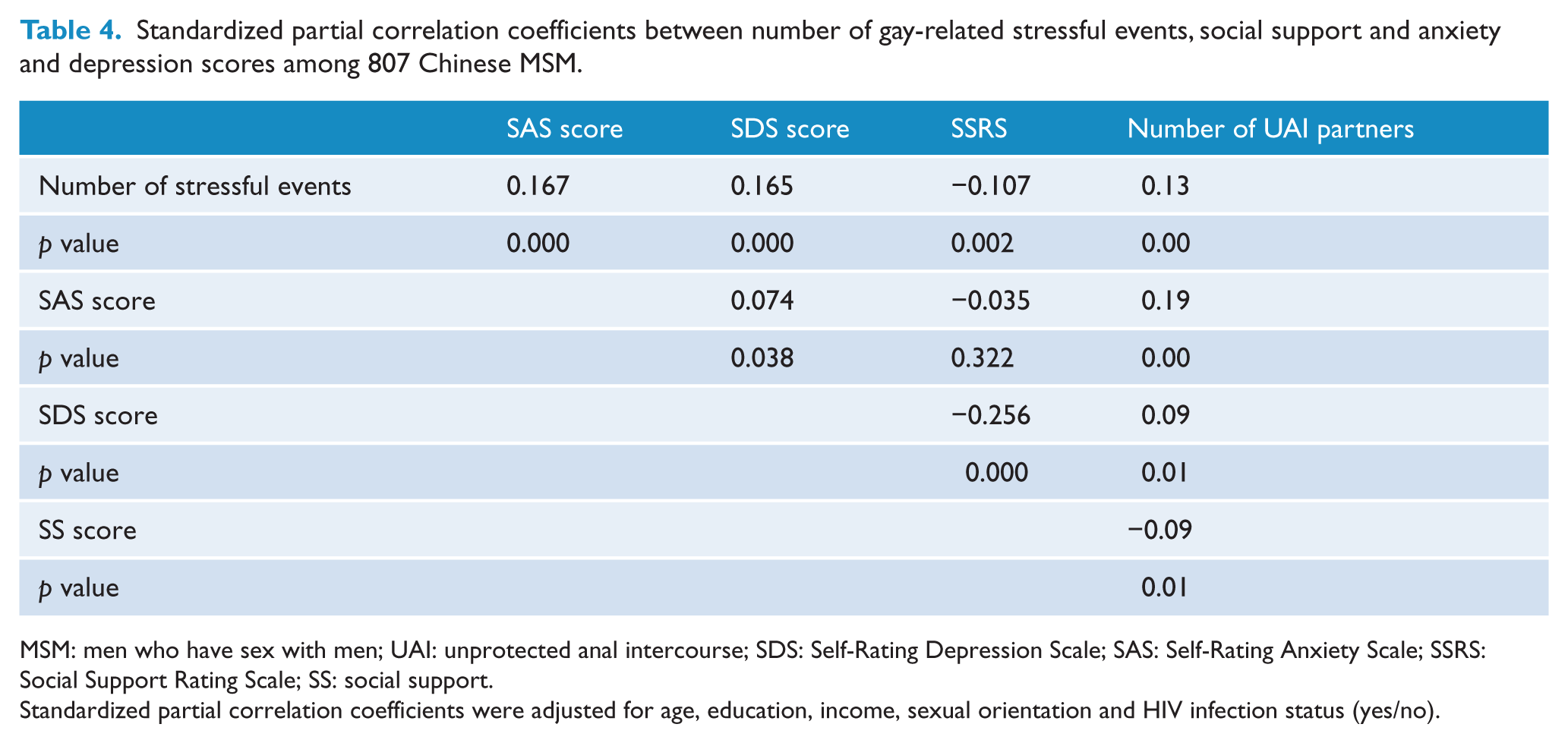
MSM: men who have sex with men; UAI: unprotected anal intercourse; SDS: Self-Rating Depression Scale; SAS: Self-Rating Anxiety Scale; SSRS: Social Support Rating Scale; SS: social support.
Standardized partial correlation coefficients were adjusted for age, education, income, sexual orientation and HIV infection status (yes/no).
Discussion
We used a standardized RDS procedure to sample 807 MSM in four cities in Liaoning province, China. A previous analysis confirmed the good representativeness of the study sample (Yu et al., 2013). To the author’s knowledge, this is the first report on the type and frequency of GRSEs among Chinese MSM. Over 25% of Chinese MSM had experienced gay-specific violence, verbal abuse and/or rejection associated with their homosexual identity during the previous 3 months, indicating that Chinese MSM frequently encounter GRSEs. It is interesting to find that the average number of GRSEs encountered by those who have revealed their homosexual identity to family members (0.61 ± 0.70) was significantly higher than that of those who hide their homosexual behaviors (0.34 ± 0.72). Homosexual behaviors are not negatively stigmatized if an individual hides a homosexual identity (Zhang et al., 2007). Some Chinese MSM may be avoiding GRSEs and the feeling that they are disgracing their families by keeping their homosexual behavior a secret. Similar findings have been observed in other ethnic, non-Caucasian MSM (Jarrett, 2006), which may reflect a lower tolerance to homosexual behaviors by certain ethnic groups.
Similar to previous findings in China, we found that MSM had higher levels of depression and anxiety symptoms, but lower social support, compared to heterosexual peers (Huang et al., 2010; Zhang et al., 2007; Zheng et al., 2005). More respondents had depressive (33%) than anxiety (13.04%) symptoms. The experienced high level of gay-related stressors and strong stigma against homosexuality in society could be the main causes of these psychosocial problems (Mays and Cochran, 2001; Meyer, 2003; Rosario et al., 2002).
We found that 82.2% of Chinese MSM had engaged in anal same-sex behavior, with an average of 4.52 ± 12.15 male partners, during the previous 6 months. Similar results were observed in a national survey on MSM in six large cities in China, in which 80.85% had engaged in anal same-sex behavior with an average of 4.33 ± 8.72 male partners (Zhang et al., 2007). We also found that 38.41% of MSM in our survey had engaged in UAI behaviors with an average of 2.19 ± 8.50 male partners in the previous 6 months. These findings indicate that UAI behaviors with multiple male partners are common, which may be the main reason for the rapid increases in HIV infection rates among Chinese MSM (Shang et al., 2012).
The significant relationships of symptoms of anxiety and depression, social support and NUAIP with the number of GRSEs, as well as the complex interactions among these factors, provide support for the hypothesis that exposure to gay-related negative life events and lack of social support are associated with higher levels of unprotected sex and emotional distress in Chinese MSM, and advance the knowledge of how syndemic is socially produced (Deuba et al., 2013; Dilley et al., 1998; Folkman et al., 1992; Huebner et al., 2004; Mays and Cochran, 2001; Meyer, 2003; Mustanski et al., 2007; O’Brien et al., 1993; Rosario et al., 2002; Semple et al., 2010; Wong et al., 2010). Frequently encountered GSREs reflect the external stigma and discrimination toward same-sex behavior that exists within Chinese society and may serve as distal stressors that affect an individual through more proximal processes, including expectations of rejection, concealment and internalized homophobia. These individuals may subsequently present with increased depression and anxiety symptoms, and they may be more likely to engage in risky sex (Meyer, 1995, 2003; Stall et al., 2003; Strathdee et al., 1998). Thus, the experience of acute gay-related stress and lack of social support may cause some Chinese MSM to attempt to escape from or ameliorate unpleasant emotions by engaging in activities that are deemed pleasurable (Semple et al., 2010). The above results are consistent with the cognitive escape model utilized to explain engagement in unprotected sex and substance use (Hoyt et al., 2006; Williams et al., 2000). GRSEs and lack of social support may result in a heightened and negative self-awareness that leads to depression or anxiety symptoms, resulting in risky behavior as a method of escaping aversive self-awareness and negative affect (Heatherton and Baumeister, 1991; McKirnan et al., 1996, 2001). It may be difficult for MSM to focus on sexual behavior changes when they are faced with numerous competing life priorities, or condom use may be deemed unimportant in the face of negative life events (Jie et al., 2012). Alternatively, UAI behaviors may partly contribute to symptoms of anxiety and depression due to the high risk of HIV transmission and the current homophobic environment for conducting homosexual activities in China.
We observed stronger correlations between the NUAIP and anxiety symptoms (r = 0.19, p < 0.01) than those with depression symptoms (r = 0.09, p = 0.01). Most studies on negative affect and HIV risk have focused on the role of depression, not anxiety (Crepaz and Marks, 2001). The causal association between anxiety and high-risk sex has not been as thoroughly studied, although daily anxious affect has been found to predict sexual risk behavior on that day (Mustanski, 2007). The few studies performed to date have failed to find a consistent association between anxiety and unprotected intercourse (Bancroft et al., 2003; Kalichman, 1999; Marks et al., 1988; O’Cleirigh et al., 2007; Rosario et al., 2006; Yi et al., 2010), whereas a meta-analysis of the association between measures of anxiety and HIV risk found a very weak effect size across studies (Crepaz and Marks, 2001). Some studies reported that high social anxiety was more common among MSM than heterosexual men (Gilman et al., 2002; Pachankis and Goldfried, 2006; Safren and Pantalone, 2005) and that social anxiety was significantly associated with UAI behaviors (Hart et al., 2008; Hart and Heimberg, 2005). However, most studies have examined anxiety as a unitary construct (Bancroft et al., 2003; Kalichman, 1999; Marks et al., 1988; O’Cleirigh et al., 2007; Rosario et al., 2006; Yi et al., 2010), without assessing the distinct types of anxiety. Future studies should be more specific on the types of anxiety associated with HIV risk behaviors (O’Cleirigh et al., 2007).
There are a number of limitations within this study that need to be acknowledged. First, the temporal misalignment between GRSEs (in the past 3 months), depression and anxiety (in the past week), social support (not specified) and NUAIP (in the past 6 months) may bias their associations. The cross-sectional design of this study makes it impossible to determine directionality or causality between GRSE and sexual risk behavior. Second, gay-related stress is multidimensional. Some aspects are external in nature and involve the experience of violence, verbal abuse, rejection and other stressful life events perpetrated by other individuals, whereas other aspects are chronic and internal in nature, involving internalization of society’s stigmatization of homosexuality. The comparability of our findings may be limited by our use of a 12-item questionnaire, and someone may not feel comfortable disclosing their true sexual behaviors or GRSE in the face-to-face interview, which may have measured only a fraction of external stressors. Finally, the 807 MSM were selected from four cities of northeast China. It is not certain that our findings can be generalized to other regions of China.
Conclusion
Our findings showed that a substantial portion of Chinese MSM in our sample experience GRSEs. These negative events, along with the lack of social support and the experience of symptoms of depression and anxiety, may interact with high-risk sexual behaviors and form worsening feedback loops. A greater experience of these stressful events was associated with more UAI partners, which could be partly mediated by emotional distress and lack of social support. Our findings suggest that the ‘synthesis’ of these problems and the HIV epidemic in MSM are rooted in cultural, historical and social structures of Chinese society. Due to the environmental, psychological and social factors that create these health disparities, HIV prevention efforts must be embedded within a larger collective framework. New interventions to reduce risky sexual behaviors should incorporate multifaceted approaches, such as reducing social discrimination toward homosexual behaviors; increasing the buffering or coping capabilities of MSM, including coping skills, self-efficacy and social support; and screening and early treatment of depression and anxiety. More studies are warranted to identify the underlying mechanisms that link negative life events to risky sexual behavior. Knowledge of when, how and why MSM engage in these behaviors may help identify potential points of intervention to prevent or reduce high-risk sexual behaviors associated with negative life events.
Footnotes
Acknowledgements
We thank all the study participants for their co-operation and support. We also thank Dr Guowei Pan, Lianzheng Yu, Jun Na and other doctors from Liaoning Provincial Center for Disease Control and Prevention for their contribution to the field work and data management.
Declaration of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Liaoning Provincial Science-Technology Department grant 2008225001. The funders had no role in study design, data collection and analysis, decision to publish or preparation of the manuscript.