
Abstract
This study examines the sociocultural impact of adolescent bio-physiological development on sexual health. By using three key metrics: sexual intercourse by age 15, self-reported sexually transmitted infections (STIs) symptoms, and condom use at last intercourse. Results reveal significant gender disparities: 9% of girls reported first intercourse by age 15 against 2% of boys; 14% of girls reported STI symptoms against 4% of boys; and 32% of girls used condoms at last intercourse, against 60% of boys. Theoretically grounded in double standard theory and the social determinants of health framework, analyses link the disparities in this result to sociocultural norms, including gendered stigmatization around female sexuality, lack of comprehensive sex education (CSE), and power imbalance in sexual decision-making that amplify biological vulnerabilities. The study highlights the need for gender trans-formative interventions, scaling (CSE) policies that challenge the gender double standards phenomenon, empowering girls to negotiate condom use, and expanding STI screening for girls. By integrating these biological and sociocultural perspectives, this study underscores the importance of addressing structural inequities geared toward the advancement of adolescent sexual health equity.
Introduction
Adolescence is a pivotal period that manifests profound biological and physiological transformations from the onset of puberty associated with hormonal fluctuations to maturation of the cortical volume and reproductive systems, laying the foundation for sexual development and consciousness.1,2 These biological shifts do not function in isolation, but unfold within a complex scenario of social and cultural contexts, shaping how adolescents experience, perceive, and express their sexuality. 3 Over the years, research has increasingly recognized adolescence sexual attitudes resulting from beliefs, values, norms about sexuality, and gender roles as not merely products of biological maturation, but are attitudes deeply influenced by familial structures, where adolescents who discusses non-judgmental sex, relationships and contraception topics with parents report higher rates of contraceptive use at first intercourse, yielding a to more positive attitudes toward sexual health. 4
However, despite growing attention to this interplay, crucial gaps, such as a detailed study on pubertal timing (early vs. late maturation) known for its significant psychological and social outcomes, limit our understanding of how social and cultural factors interact with biological changes during adolescence to mold their sexual attitudes and reproductive health, particularly in this era of rapid social transformation. This study aims to address these gaps by examining the social and cultural contexts of dynamic adolescent biological/physiological changes, and the formation of sexual attitudes by identifying how culturally specific norms and values moderate the relationship between biological changes and sexual attitudes in adolescents, and exploring intersectional effects on how gender, race, and cultural identity collectively influence the development of sexual attitudes. This study will advance a more nuanced understanding of adolescent sexuality by integrating biological, sociological, and cultural theories through centering diversity and intersectionality. Insights from this study can inform culturally responsive sex education programs, adolescent sexual attitudes and social gender discrepancy, parenting guidance, and mental health interventions, enabling more personalized and empathetic care that avoids cultural biases toward promoting positive sexual attitudes, and ultimately contributing to the well-being of adolescents across diverse sociocultural landscapes.
Literature Review
Pubertal Timing and Association with Sexual Onset
The biological and physiological transformations during adolescence (Puberty), marked by the development of secondary sexual characteristics such as breast buds, facial hair, menstruation, and spermatogenesis, Juraska and Willing 5 play a fundamental role in sexual development, not only driving physical maturation but also giving rise to sexual urges, attraction, and continuing throughout adolescence, Blakemore et al. 6 and Mendle et al., 7 delves into how early puberty, a biological marker, interacts with social factors to heighten the risk of early sexual activity, emphasizing the complex interplay between biological, psychological, and social elements. While Andreas et al., 8 through a population-based study, estimated current ages at pubertal development in both boys and girls. Euling et al. 9 considered the role of environmental factors in the timing of puberty in adolescents, while considering changes in the timing of puberty markers. Similarly, also from environmental variables, Buck Louis et al. 10 concluded that available experimental animal and human data support a possible role of endocrine-disrupting chemicals and body size in relation to alterations in pubertal onset and progression in boys and girls. Luo et al. 11 through a longitudinal cohort study, and using realistic color images and the Pubertal Development Scale, investigated the validity of self-assessment pubertal Tanner stages, where the concordance of genital development self-assessment was fair in boys, wk = 0.285 (P < .001), while Ernst et al. 12 and Campisi et al., 13 emphasized the importance of proper structuring of the Self-assessment of puberty. Furthermore, Granados et al., 14 used data from a longitudinal growth study to examine the relationship between peak height velocity (PHV) and Tanner staging, where they observed a substantial variability in the timing across Tanner stages, which is an important marker for clinicians when assessing growth. Ljubicic et al. 15 and Gacemer et al., 16 argued the development of external genitalia during mini-puberty, linking it to somatic growth or reproductive hormones, relating to an early study conducted by Johannsen et al., 17 which evaluated sex differences in reproductive hormone concentrations in serum from healthy infants to define sex-specific cutoff values applied to infants with disordered sex development (DSD).
Hormonal Shifts and Sexual Desire
Hormonal fluctuations, particularly the increase in gonadotropins (LH, FSH), estrogen, and testosterone, are responsible for both physical maturation and the emergence of sexual desire. Comprehending how these hormones regulate attraction, arousal, and behavior is of utmost importance. Duke et al. 18 utilized a 27 longitudinal study to examine the testosterone and aggression level in adolescents; their results showed little relationship with concurrent changes in aggression. Sisk, 19 studied the onset of puberty, ovarian hormones increase inhibitory tone in the prefrontal cortex of adolescents, postulating that pubertal hormones may trigger the opening of a critical period for experience-dependent rewiring of adolescent underlying executive function. Schulz and Sisk 20 studied the role of gonadal steroid hormones in shaping adolescent brain and behavioral development, highlighting the perinatal period as a sensitive period for adolescent sex-specific effects on brain and behavioral development. Herting and Sowell 21 also expanded on the context, arguing that sex hormones continue to influence the brain beyond the prenatal period, with both organizational and activational effects occurring during puberty. Corinna et al., 22 through a review of animal and human brain imaging studies, explored how potential change in neural resources and behavioral repertoire differs across age groups, indicating the pivotal role of pubertal hormones in regulating the experience-dependent plasticity mechanisms during adolescence. Dongmei et al., 23 employed a systematic review of 55 papers aimed at synthesizing the evidence of pubertal hormones, while Chafkin et al., 24 through a linear regression analysis, tested estradiol associated with adolescent social sensitivity that interacts with pubertal stage, while Abigail et al., 25 also studied the association between the endogenous sex hormone estradiol and emotional attentional biases in adolescent females.
Neurobiological Development and Sexual Decision-making
Adolescents’ bodies display distinct physiological reactions to sexual stimuli, which are linked to both biological readiness and psychological factors. Hegde et al. 26 and Jennifer and Leslie, 27 treated the deficiencies of legal treatment of juvenile decisions in the context of sex with an adult, while integrating new scientific information regarding the decision-making of minors in vulnerable conditions. Ciranka and Wouter 28 argued that the reason for this lack of proper decision-making in adolescents can be linked to the absence of precisely formulated models such as social motivation, reward sensitivity, and distraction. Hartley and Somerville 29 also attributed decision-making ability to the interactions between prefrontal cortical, striata, and salience processing systems that constrain and amplify various component processes of mature decision-making, while Orma et al., 30 from neurodevelopmental literature, evidence argues that brain immaturity undermines decision-making, as it also relates to gender-affirming care (GAC) in adolescents.
Adolescent Sexual Attitude and Reproductive Health
Adolescent Sexual Attitudes Toward Early Intercourse
Adolescent reproductive health entails prevention of unintended pregnancy, control of sexually transmitted infections (STIs), and lifelong reproductive wellness, 31 deeply shaped by sexual attitudes, values, beliefs, and norms from parents that shape how teens interpret personal biological changes, such as puberty and hormonal drives, that help them navigate sociocultural expectations around sex. 32 Many adolescents equate sexual maturity as a social marker with early intercourse while growing up—an attitude often fueled by sociocultural norms, rewarding boys for sexual experience, and penalizing girls for the same act. Several public health data have confirmed that girls who initiate sex by 15 are 2.3× more likely to have an unintended pregnancy than those who wait until 17+, largely due to lower condom use driven by shame-based attitudes. Adolescents with a low reproductive autonomy are far more likely to engage in intimacy early, a sexual attitude rooted in sociocultural dis-empowerment, where girls have limited access to education, have little or no power over their bodies, or are involved in early marriages, thereby normalizing early intercourse. Also, early pubertal development (boys with early voice changes and girls starting menstruation at 10) intersects with attitudes to drive early intercourse, where adolescents who experience such early biological maturity often face pressure to act “above their age,” which socially shapes their attitudes toward having early age intercourse.
Adolescent Sexual Attitudes Toward STIs and Reproductive Health
Genital discharge, soreness, or ulcers are prevalent symptoms, which, if untreated, have the capacity to cause long-term reproductive harm such as pelvic inflammatory disease, ectopic pregnancy, and infertility. Yet, based on the CDC 2024 report, only 28% of adolescents with these symptoms seek care. Other attitudes toward STIs are the stigma of being associated with such a disease, linked to societal moral failure, and that STIs are a punishment for “bad” sexual behavior. For girls, this stigma is compounded by gendered shaming, where a girl with an STI may be tagged as “impure,” resulting in attitudes of self-blame and avoidance of seeking adequate care. Whereas, boys’ stigma often manifests as “macho,” delaying treatment until symptoms worsen. Similarly, most adolescents also avoid reporting STIs even when symptoms are severe, an attitude rooted in systemic barriers, where a 2022 East Africa study also found a slow care-seeking behavior in women due to relatively low educational status and household wealth index. 33 Most adolescents hold attitudes that STIs will go away on their own, have the notion that only HIV is serious, a misconception also fueled by a lack of comprehensive sex education (CSE). For example, a teen with chlamydia (often experiencing a mild discharge), may dismiss symptoms as “a cold down there,” delaying care until pelvic pain, which is a sign of advanced infection, eventually develops. This attitude directly increases long-term reproductive system harm, as adolescents who delay STI treatment are three times more likely to develop infertility or chronic pelvic disease.
Adolescent Sexual Attitudes Toward Condom Use
Condoms are the only method that can effectively prevent both unintended pregnancy and STIs, yet global condom use among sexually active adolescents remains inconsistent, 34 an attitude primarily driven by limited sexuality awareness. This situation’s most common factor is the attitude that “condom use ruins the moment” or makes sex less intimate, a belief most times reinforced by mainstream media and peer norms. For boys, this attitude is attributed to their feeling of masculinity, that real men do not need condoms, or “I can tell if and when my partner is clean” syndrome. For girls, it often originates from pressure to prioritize their partner’s pleasure. Adolescent girls who hold these attitudes are 70% less likely to use condoms, thereby increasing their risk of unintended pregnancy and STIs. Also, many adolescents in committed relationships have the attitude that they are exclusive, so the use of condoms is not needed. This attitude ignores the risk of pre-existing STIs contracted from previous relationships.
Adolescent Sexual Attitudes and Social Gender Discrepancy
A core dimension of discrepancy in adolescent sexual health lies in gendered interpretations of sexual responsibility and biological development 35 which skew perceptions of sexual accountability and behavior. Both male and female adolescents undergo biological hormonal shifts, but sociocultural norms frame these changes through unequal lenses. A 1,057-adolescent mixed-method study by Agu et al., 36 in southeastern Nigeria, found that 69.6% of respondents hold the opinion that sex should be initiated by boys, while 66.5% hold girls responsible for preventing pregnancy. This divide reflects cultural ideologies that cast male sexual curiosity as inevitable and natural, but frame female sexuality as an act to be controlled. Equally helpful in understanding adolescent social gender discrepancy is the gender gap in access to sexual health services and knowledge, which is constantly widening despite parallel biological needs. A 2024 study of Ekiti state (Southwestern Nigeria) adolescents also found that 72.5% of females had better sexual and reproductive health (SRH) knowledge, against just 57.2% of males. 37 A gap attributed to gendered assumptions that girls need (SRH) education more to avoid pregnancy, while boys are left to rely on informal and peer networks. Unfortunately, this discrepancy persists even when parents advocate for an enhanced school-based sexuality education. Social gender discrepancy in adolescent sexual health does not merely overlay their biological development, but rather it reshapes it.
Data, Methodology, and Results
Data Collection
Data for this research is a demographic and health survey of Nigeria extracted from the UNICEF publicly available database (
Methodology
We employed a descriptive statistical method to analyze of categorical variable (×) (“boys vs. girls”) against our numerical variable (y) (percentage of estimated metrics), and the following formula for estimation was constructed as follows:

Where β denotes event count (Group), γ denotes the total size of the group.
Result
Based on the above Formula (1), our categorical variable descriptive statistics were conducted, and the results are presented as follows:
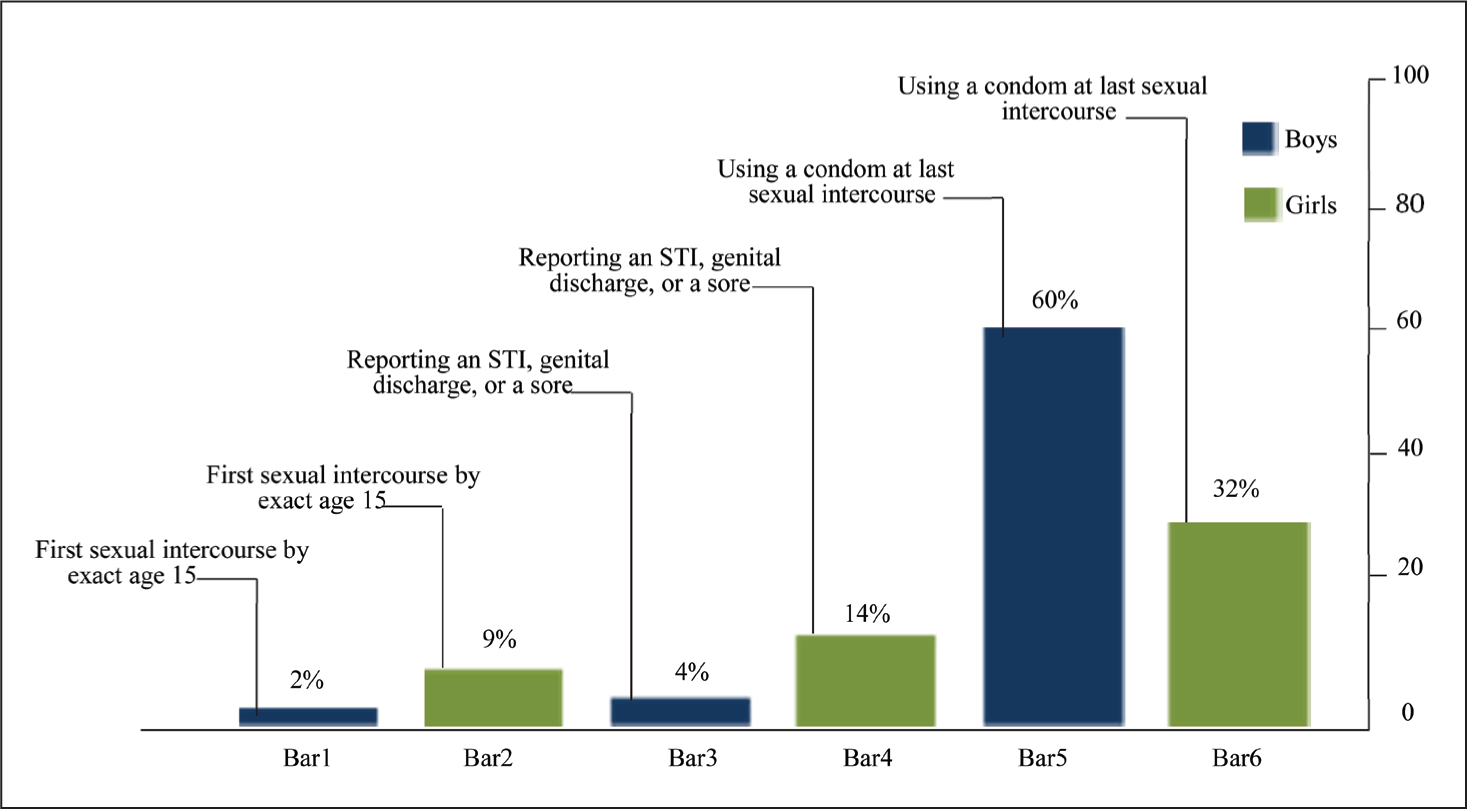
Bar 1 represents the number of adolescent boys who had first sexual intercourse at the exact age of 15, with the value of 10 representing 2% of the entire population. Bar 2 represents the number of adolescent girls who had first sexual intercourse at the exact age of 15, with the value of 45 representing 9% of the entire population. Bar 3 represents the number of adolescent boys that reported STIs, genital discharge, or s sore, with the value of 20 representing 4% of the entire population. Bar 4 represents the number of adolescent girls that reported STIs, genital discharge, or s sore, with the value of 70 representing 14% of the entire population. Bar 5 represents the number of adolescent boys who reported usage of a condom at last sexual intercourse, with the value of 300 representing 60% of the entire population. Bar 6 represents the number of adolescent girls who reported the use of a condom at their last sexual intercourse, with the value of 160 representing 32% of the entire population (Figure 1).
Adolescence Sexual Attitude and Reproductive Health.
Discussion
Grounded in double standard theory and the social determinants of health framework, our analyses link the disparities in this result to sociocultural norms. Our data reveals significant gender differences in adolescent health indicators and sexual behavior, where only 2% of boys engage in first sexual intercourse by age 15 compared to 9% of their female counterparts. In many cultures, there exists a sexual double standard, where early sexual initiation is sometimes seen as a sign of masculinity or a rite of passage for boys, 38 but the relatively low percentage (2%) of boys engaging in sex by age 15 might be due to multiple factors. This condition agrees with the study by Ji-Eun, 39 a qualitative research on Laotian adolescents, emphasizing social norms as a deterrent, where the sociocultural environment is an important enhancer of family values and education that frowns on early sexual activity, leading to adolescent boys being less likely to engage in early sex. On the other hand, the 9% of adolescent girls having sex by age 15 is a concerning figure, as in some patriarchal societies where girls may be more vulnerable to sexual coercion, or engage in early sex due to misinformation, mostly pronounced in certain low-income societies with limited sex education, significant number of adolescent girls might believe that early sexual relationships can provide a sense of belonging or financial security. This situation aligns with Sychareun et al., 40 suggesting that early marriage and pregnancy are the aftereffect of such a scenario.
The huge difference in the reporting of STI symptoms between boys (4%) and girls (14%) can be linked to several sociocultural factors. For example, in Nigeria, a study by Granados et al., 14 found that gender differences in seeking treatment for STIs were dominant, as males were less likely to seek treatment due to a lack of financial resources (64% boys vs. 48% girls). Sapna et al., 41 also reported (rural: 66.2% boys, 23.1% girls; urban: 69.4% boys, 30.7% girls) for adolescents who reported symptoms of genital infections in India not seeking medical care, which also corresponds with our result. However in some cases, adolescent girls shy away from seeking treatment for STI due to concerns of being severely judged or stigmatized, thereby leading to more severe health complications in the future, while sociocultural contexts in developing countries also influence the epidemiology of STIs, a condition that aligns with Hussain et al., 42 study on the health care-seeking pathway of eight hundred reproductive age women (15–49 years) suffering from RTls/STls, out of total 359 participants with symptoms of RTls/STls, only about one-third (37.3%) had sought medical treatment, and only 4.5% had sought treatment within one month of symptoms appearance, thereby requiring a multi-faced policy and corresponding measure to tackle.
The 60% condom reported value among boys compared to 32% among girls indicates a significant gender gap, with sociocultural norms playing a major role. If the sociocultural environment does not encourage gender equality in sexual decision-making, girls may find it difficult to convince their partners or insist on condom use. Also, in many adolescent relationships, there exists a power dynamic where boys have more say in sexual decisions than girls. A study on sexual negotiation in adolescent relationships 43 a study conducted with 104 adolescents that reported a higher compromise and submission by girls against their own sexual satisfaction and comfort, justifies our result. Moreover, the influence of media and misinformation also contributes to this gap, as the media often portrays sexual relationships in an unrealistic light and has repeatedly downplayed the importance of condom use and promoted sexual coercion. 44 When adolescents are exposed to such social content, it reshapes their attitudes toward the use of condoms during intercourse. For adolescent boys, the relatively higher value of condom use might be associated with peer influence and level of sex education. This assertion aligns with the early study by Jennifer et al., 45 that examined the multiple domains of influence on condom use behaviors among male adolescents in the United States found that adolescents who receive formal sex education had more positive attitudes about condom use.
Recommendation
Mandatory Gender-transformative CSE
CSE, as defined by UNESCO, should include topics like anatomy, consent, STI prevention, and gender equality, as in-depth awareness of these metrics is proven to delay early sexual intercourse in adolescents, increase condom use, and reduce STI contraction. For this to be effective, (CSE) must be gender-transformative: Prioritize comprehensive and culturally responsive sex education that centers consent, accurate information, and diversity. Educate parents and provide guidance to have open, non-judgmental sexual conversations regardless of religious or cultural background. Regulate harmful digital content as it is currently being consumed by adolescents, while promoting positive sexual health campaigns on social media, and effectively address structural barriers that disproportionately affect marginalized adolescents.
Gender-sensitive STI Screening and Treatment Programs
Due to biological differences in STI vulnerability, targeted screening is required to foster testing and treatment. This can be achieved through school or community-based STI screening for girls aged 13–17, while focusing on asymptomatic infections such as chlamydia that often go undetected for a longer period of time. The provision of gender-sensitive treatment services can also be considered, where, for confidentiality and avoidance of stigmatization purposes, girls may my treated outside the clinics, while also empowering girls through Peer-Led Sexual Health Advocacy.
Address Structural Barriers in Adolescent Sexual Care
Addressing anti-stigma policies that disproportionately affect marginalized adolescents should be applied. Also, moving beyond the “one-size-fits-all” approaches, and creating environments that appropriately support adolescents of both genders in low- and medium-income countries through informed sexual identities, including those from racial/ethnic minorities, low-income households, LGBTQ+, and those with disabilities, to freely access health care services should be considered. To achieve this, policy-driven steps that replace discriminatory policies like parental consent requirements with “mature minor” policies that allow adolescents to independently access sexual health care should be put in place.
Research Limitation
This study examines the sociocultural impact on adolescent bio-physiological development and sexual health using three metrics: sexual intercourse by age 15, self-reported STI symptoms, and condom use at last intercourse. For more robust analysis, we encourage future research to include more parameters, and the research scope be extended to a global scale, as this will aid in a more nuanced understanding of the topic.
Conclusion
Our study examined adolescent biological and physiological change, its sociocultural impact on their sexual attitude and reproductive health. Study results revealed striking gender disparities: girls are more likely to engage in sexual intercourse by age 15, report STI symptoms, and use condoms less frequently than boys. These disparities are not accidental but rooted in sociocultural norms that sustain unequal power dynamics. The study highlights the crucial role of sociocultural factors in reshaping adolescent sexual attitudes and improving adolescent reproductive health, which can only be achieved through targeted and CSE, reduction of STI stigmatization and promotion of gender equality to help bridge the gender gaps in sexual health outcomes, while ensuring all adolescents are equipped with the necessary resources and knowledge to make informed decisions about their sexuality and sexual health.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
The participant has consented to the submission of the article to the journal.