
Abstract
This article argues for the integration of Sexual Orientation, Gender Identity and Expression, and Sex Characteristics (SOGIESC) content into academic training of mental health professionals in India to address significant gaps in understanding and treatment of SOGIESC diverse individuals. Despite growing recognition of SOGIESC as critical determinants of mental health, current curricula often neglect these aspects, perpetuating biases that adversely affect diagnosis and care. This article highlights the structural inequalities faced by SOGIESC communities and the resultant impact on mental health outcomes, emphasising the need for a rights-based approach in mental health education. Through a comprehensive review of existing literature, this article identifies pervasive stereotypes and discrimination within healthcare settings that hinder effective treatment. It proposes a multi-stage integration pathway, beginning with audits of current curricula, followed by content development that incorporates SOGIESC awareness into training programmes for mental health professionals. This article advocates for participatory processes involving stakeholders from SOGIESC communities to ensure that training is relevant and effective. It is argued that enhancing competency in SOGIESC issues among mental health professionals is essential for fostering equitable care. By addressing both stigma related to mental health and discrimination based on sexual orientation or gender identity, this integration can contribute to a more inclusive healthcare landscape in India, aligning with the broader goal of achieving ‘health for all’.
Introduction
The importance of Sexual Orientation, Gender Identity and Expression, and Sex Characteristics (SOGIESC) as major determinants of mental health, and their relevance to diagnosis and treatment, has not received adequate academic attention. 1 Existing evidence shows the importance of gender as a cross-cutting variable influencing diagnosis, treatments and long-term outcomes in mental health. 2 Gender plays a role in determining one’s vulnerability to certain mental illnesses. Also, gender stereotypes and norms internalised by trained professionals can have an impact on health inequality, especially in societies where misogyny is highly prevalent.
As our understanding of SOGIESC continues to evolve thanks to insights from biological, neuro and social sciences, there is a need to integrate these insights into the education being imparted to mental health professionals. This article lays out a case for the integration of SOGIESC-related content to the academic training of mental health professionals in India, acknowledging the progress made in this direction. Mental health education in the context of this article includes postgraduate training in psychiatry, psychiatric social work and clinical psychology. The term mental health professionals used in this article also covers all these professions. The more inclusive phrase ‘SOGIESC diverse’ is used in this article in place of the often-used initialism of Lesbian, Gay, Bisexual, Transgender, Queer, Intersex, Asexual and other (LGBTQIA+). 3
SOGIESC, Bias and the Fallouts for Curricula
Structural gender inequalities can have far-reaching consequences for the lived experiences of people. Societal gender inequality can be associated with structural brain differences between men and women, with palpable differences noted in cortical thickness in limbic regions, seen more in countries with higher levels of gender inequality. 4 Such differences have consequences at the community level and can lead to higher rates of prevalence of specific mental illnesses5,6 and lower levels of positive mental health—effects that could be even more pronounced for persons belonging to non-hetero sexual orientations and diverse gender identities.
What is also noteworthy is that gender stereotypes and insensitivity prevalent in a society may be reflected among medical students 7 with implications for attitudes and treatment outcomes. Gender bias and stereotypes have been found to influence the diagnosis, treatment and interpretation of symptoms in cases ranging from pains to coronary heart disease.8,9 This phenomenon has been observed even in the practice of specialised areas such as forensic psychiatry. 10
The bias and stereotypes faced by persons with diverse gender and sexual identities could be deeper and more nuanced than those faced by women 11 owing to the intersectionality of factors. Strong negative stereotypes about transgender persons are found to exist even among healthcare professionals. These stereotypes even reach the extent of wrongly equating being transgender to a mental illness. 12 Discrimination against persons belonging to the diverse SOGIESC communities found in other parts of the world13,14 is found in the Indian healthcare sector also, though it is comparatively less in psychiatry departments. 15 Still, lack of awareness combined with the absence of an intersectional approach among healthcare professionals can lead to humiliating and dehumanising experiences for non-cis-hetero individuals while seeking mental healthcare. 16 In societies where homomisia and transmisia/transphobia are prevalent, this situation could lead to multiple issues such as low quality of care or even denial of care, leading to further distress and mental health issues, 17 thereby leading to a paradoxical situation of care seeking becoming a trigger for more traumatising experiences.
Reviews of medical curricula and teaching practices from different parts of the world have shown the existence of discrimination, 18 lack of awareness19,20 and specific gaps in SOGIESC-related content in the curricula and training provided to students.21-24 Lack of awareness and prevalence of stereotypes and the resulting discrimination are common findings from such studies. Biases related to gender and sexuality could be more difficult to understand and address when they are implicit 25 which is the case most often.
Redressing these identified gaps is essential in making medical training more inclusive and effective, and making public health systems more equitable. Bridging the gaps in SOGIESC inclusion is particularly important in mental health where the relationship between a client and practitioner is crucial in deciding treatment outcomes. The power dynamics inherent in the therapeutic set-up also necessitate attention to SOGIESC as an important consideration for therapeutic success.
SOGIESC Diversity and Professional Training in Psychiatry/Mental Health
The available evidence on attitudes and awareness among mental health professionals regarding SOGIESC diversity shows gaps in training and some related issues. Audits have revealed gaps in medical training curricula with regard to SOGIESC diversity.26-29 The ‘two-gender’ logic 30 prevalent in medicine in general is visible in the mental health field too. It is found that the confidence level of practitioners is even lower when dealing with gender-diverse clients than when providing care to clients with diverse sexual orientations. 31
Exposure to individuals from diverse SOGIESC groups can help address some of these gaps. Practicing professionals in mental health have expressed a need and readiness for training in SOGIESC diversity and providing such training has shown to increase the competency and confidence of professionals in providing care to SOGIESC diverse clients as well.32,33 Surveys with medical students have also shown readiness and an acknowledgement of need for SOGIESC diversity-related content in medical curricula. 34 The revised Competency-Based Postgraduate Training Programme guidelines for MD Psychiatry by National Medical Commission (NMC) of India is one of the first moves to address this need by integrating SOGIESC-related competencies, such as gender identity assessment and ethical care practices, into its framework. 35 The guidelines mandate competencies such as assessing gender identity, counselling LGBTQIA+ clients and rejecting unethical conversion therapy.
There is limited evidence available on the experiences of SOGIESC-diverse individuals seeking mental healthcare in India. In available studies from the medical field, SOGIESC diverse persons have reported having to face bias and discrimination from within the medical domain while seeking care.15,36,37 Persons belonging to sexual minorities have reported experiences of lack of understanding and ignorance from the side of mental health professionals. 38 Lack of proper training and rights-based approach among mental health professionals has been shown to create problems including discrimination 15 and misdiagnosis in sexual mental healthcare. 16 Misconceptions such as homosexuality being an illness are prevalent at least among a small section of medical students. 39 Many medical professionals are uncomfortable caring for SOGIESC—diverse patients, primarily because of inexperience, lack of skills or negative attitudes. 40
One theme that emerges from the literature is a lack of a rights-based approach—something that has characterised the recent legislations such as the Transgender Persons (Protection of Rights) Act, 2019 and the Mental Healthcare Act (MHCA), 2017. Another theme is the lack of awareness among practitioners. These issues could be attributed as important reasons for the prevalence of unethical and unscientific practices like conversion therapy still existing in India despite legal provisions and position statements by professional organisations against such practices.41,42
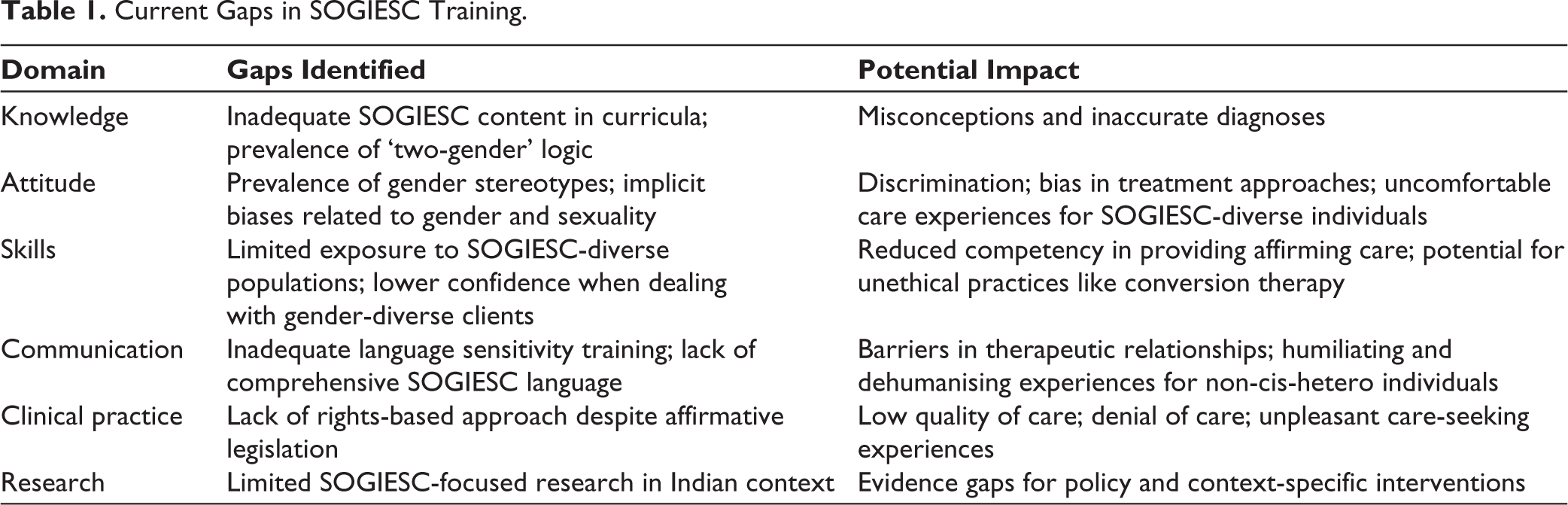
Over the past few decades, there have been demands for modifications and interventions from a gender perspective in the training and practice of medicine and mental health in India. 43 The lack of adequate representation of women in psychiatry has been pointed out as a significant issue to be addressed. 44 The need for developing a comprehensive language concerning SOGIESC 45 and the necessity for greater awareness, research and change of attitude regarding diverse sexual orientations 46 have all found a place in the academic discourse. More recently, the need and ways for mental health professionals to become queer affirmative in mental healthcare have also been discussed. 47 Assessments of some medical textbooks have suggested that a rights-based approach to gender is lacking and that patriarchal biases still exist. 48 Judicial interventions in response to rights groups representing SOGIESC diverse persons have also happened where courts have directed governments to look into ‘queerphobic’ content in undergraduate medical textbooks. Table 1 provides a summary of SOGIESC-related gaps that exist in present training curricula and their potential impact. 49
Current Gaps in SOGIESC Training.
The Case for SOGIESC Integration
Research has established that knowledge about SOGIESC diversity and a positive attitude is necessary for medical professionals to avoid stereotypes and biases and also to provide equitable care to all. 19 It is such knowledge and attitudes, along with skills and communication ability that constitute competency in the Competency Based Medical Education (CBME) framework. 50 Professionals aware of SOGIESC will be better equipped to comprehend and unlearn the stereotypes related to gender and sexuality that they may inadvertently carry. This awareness can facilitate an understanding of the diverse experiences of SOGIESC clients, which could have influenced the pathologies they present. Professionals with the right attitude, knowledge and competency are instrumental to mitigating existing health disparities faced by SOGIESC diverse individuals and fostering a healthcare environment that is inclusive and affirming for all individuals. The integration of SOGIESC concepts into curricula can enhance the professional competence of trainees as well. The goal of ‘health for all’ cannot be achieved without providing inclusive and affirming care to all with due consideration to their experiences and contexts.
SOGIESC integration is particularly important for the mental health field. SOGIESC awareness can improve therapeutic relationships by facilitating better communication, increased trust and comfortable disclosure, thereby improving treatment outcomes.51,52 Mental health concerns are higher among SOGIESC-diverse individuals in India 53 as found elsewhere. In the Indian context, there is the added dimension of the generally existing stigma related to mental health topics 54 coupled with the discrimination and neglect faced by SOGIESC diverse individuals15,55 that need to be addressed. SOGIESC integration in the curricula is one of the ways how this double disadvantage can be addressed. There have been some models and frameworks available from existing literature that could inform such an integration process.
A Suggested Integration Pathway
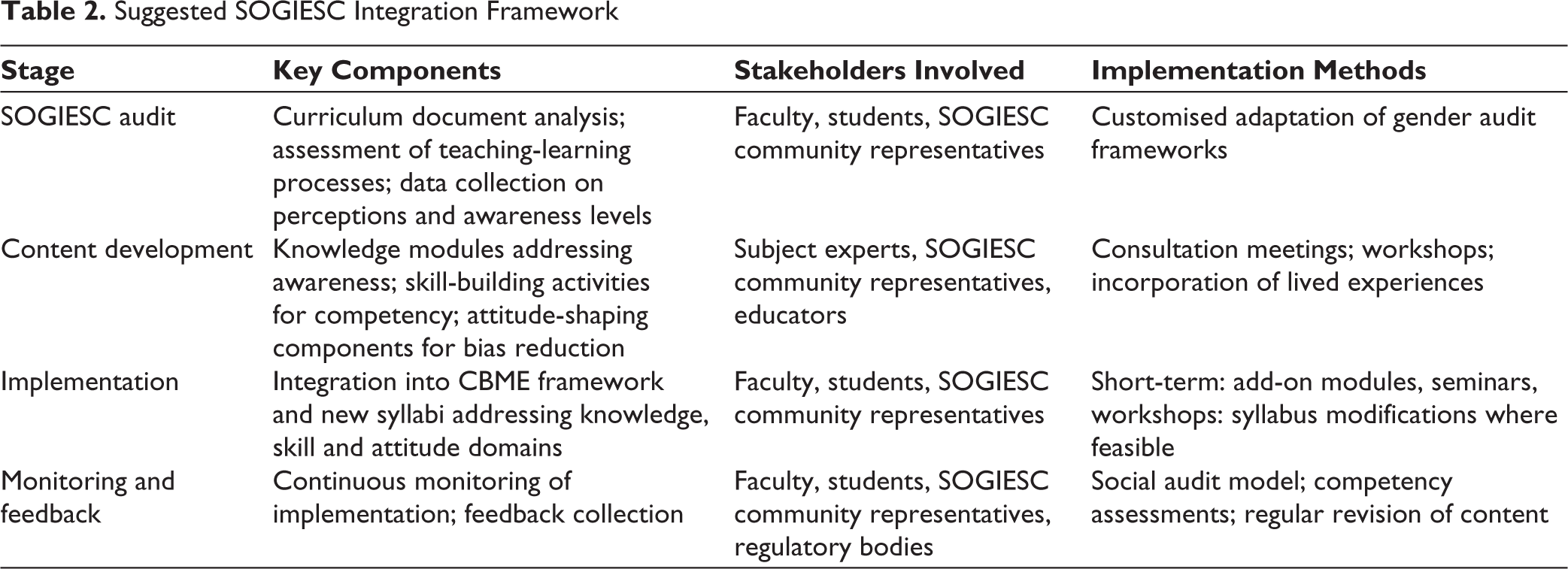
The suggested SOGIESC integration in mental health training begins with an audit of the existing curricula and progresses through the development of SOGIESC inclusive content, integration of the content to the CBME framework and monitoring with special initiatives for exposure and familiarisation. The components are described below as a general blueprint and can be adapted for different contexts such as the training of Psychiatrists, Clinical Psychologists and Psychiatric Social Workers as per regulations of the Rehabilitation Council of India (RCI) and the training of Psychologists and other Behavioural Health Professionals as per upcoming regulations to be framed by the National Commission for Allied and Healthcare Professions (NCAHP). The Table 2 provides a summary of the suggested integration framework, listing the major components, stakeholders, and cues for implementation.
Suggested SOGIESC Integration Framework
SOGIESC Audit of Curricula
The SOGIESC audit of the existing curricula and the teaching-learning process in psychiatry and mental health education is essential to identify the existing gaps and specific needs. Existing literature provides sufficient evidence for the efficacy of such audits.20,27,28 The audit can be conducted using a customised adaptation of the commonly used gender audit frameworks 56 employing both the analysis of curriculum documents and the analysis of the processes through which these curricula are implemented as teaching-learning processes. The audit shall also include data collection on the perceptions and awareness levels of key stakeholders, including students and educators. The outcomes of the audit would inform the content development process.
Content Development
The instructional content for SOGIESC awareness and best practices would need to be developed through a consultative process with the outcomes of the audit serving as the primary source of information on needs, gaps and awareness levels. Existing academic literature, expert consultation and consultation with the interest groups of SOGIESC diverse communities can also inform the content development process. Consultation meetings and workshops will help in knowledge exchange and collaborative development of content that is informative, inclusive, affirmative and actionable. The content needs to address Knowledge, Skill, and Attitude domains of learning as envisaged in the CBME framework. 50
Implementation
Implementation of the SOGIESC integration content into the teaching-learning process can be accomplished as a multi-stage process. Different channels and integration strategies as envisaged in the CBME framework can be utilised for this. 57 Since modifying syllabi in postgraduate medical education may not be immediately feasible, other knowledge transaction methods such as add-on modules, seminars and workshops may need to be utilised while rolling out the implementation. The NMC’s revised CBME framework facilitates SOGIESC integration through structured modules, such as the mandatory training on gender identity assessment and ethical history-taking. For example, the module on Gender Dysphoria provides a template for institutions to develop workshops on counselling SOGIESC-diverse clients. Add-on modules (e.g., workshops on ethical history-taking) and interdisciplinary rotations (e.g., community psychiatry placements focusing on SOGIESC-diverse populations) can operationalise the guidelines without requiring immediate syllabus changes.
In the case of programmes where the syllabi are being designed, such as the replacement of the MPhil Clinical Psychology course with the proposed MA Clinical Psychology programme, the content can be incorporated into the syllabi being developed. Similarly, the syllabi being framed for the training of Behavioural Health Professionals under NCAHP regulations can also be designed by incorporating the SOGIESC-related content.
One essential component to be ensured in the training process is avenues for listening to the perspectives and experiences of the persons belonging to SOGIESC diverse communities. This is significant because of the importance of the lived experiences of patients/clients in the caregiving process, which usually goes unnoticed in the medical practice. Co-production of knowledge about mental health conditions and enhancement of quality of care have already been hinted as possible outcomes of such a perspective to psychiatry. 58 This is even more important in the Indian context since most professionals need not have had interactions with SOGIESC-diverse patients/clients before the professional training in mental health.
Monitoring and Feedback
The final and important component in the SOGIESC integration process is the continuous monitoring of the implementation of the SOGIESC-related content in the teaching-learning process and the feedback collection on the same. The feedback can be obtained by utilising a social audit model. The social audit model has already been experimented with as a method to improve the participation of the community in the health services delivery process, elevating them from the status of passive beneficiaries 59 to empowered partners. Social audits do offer the potential to improve the quality of care and also facilitate improved programme outcomes,60,61 two effects that are expected in the present context too.
Conclusion
It is high time that medical education in psychiatry and other mental health-related professions in India be made more responsive and sensitive to SOGIESC diversity. The integration of SOGIESC content into mental health training curricula is crucial for achieving this and providing affirming care to all individuals, regardless of their gender identity or sexual orientation. This integration needs to be taken up as a participatory process with multiple steps and needs to be monitored and improved continuously. Initiatives like the revised NMC curriculum for PG psychiatry need to be expanded and mainstreamed. By addressing the double disadvantage faced by SOGIESC diverse individuals in India, who often experience stigma related to both mental health and their gender identity or sexual orientation, this integration process can help create a more inclusive and equitable healthcare landscape in the country. It can also improve the competency of mental health professionals in the country. Ultimately, the goal of ‘health for all’ can only be achieved by providing affirming and quality care to all individuals, considering their unique experiences and contexts.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Declaration Regarding the Use of Generative AI
While preparing the manuscript, the author used the Claude 3.7 Sonnet by Anthropic to rewrite the content and improve readability. The author reviewed and edited the artificial intelligence (AI)-generated content as needed and takes full responsibility for the content of the publication.
Ethical Approval and Informed Consent
Ethical approval and informed consent are not applicable since there are no human participants involved.
Funding
The author received no financial support for the research, authorship and/or publication of this article.