
Abstract
Background:
This study examines the relationship between sexual fantasies, sexual dysfunction (SD), and sexual well-being, focusing on individuals with SD group compared to healthy controls.
Methods:
Participants included patients with sexual health concerns diagnosed with erectile dysfunction (ED) or premature ejaculation (PME) and healthy controls. Assessment tools included the Arizona Sexual Experience Scale (ASEX-M), Wilson’s Sex Fantasy Questionnaire (WSFQ), sexual quality of life (SQoL) scale, and subjective sexual satisfaction (SSS) scale. Data were analysed using descriptive statistics, correlation coefficients, and two-way ANOVA tests.
Results:
Socio-demographic profiles of the cases and controls were matched for age, marital status, sexual activity, education, and religion, with a mean age of 30 years. With regards to WSFQ scores, no significant difference in total fantasy scores between the SD group and controls was found. Significant differences in intimate and impersonal fantasy domains were present. The SD group scored significantly poorer than controls in sexual satisfaction, ASEX, and SQoL. The correlation studies showed positive correlations between WSFQ and SSS, WSFQ and SQoL, and a negative correlation between WSFQ and ASEX in controls. No significant correlations in the SD group. ANOVA Studies revealed significant main effects of SD on SSS (F = 165.38, η2 = 0.465, P = .001 variance), SQoL (F = 84.651, P < .001, η2 = 0.308), and ASEX (F = 170.566, P < .001, η2 = 0.473). Sexual fantasies also contributed to the variance in SSS (F = 4.592, P = .001, η2 = 0.088), and SQoL (F = 3.746, P = .006, η2 = 0.073).
Conclusions:
This study highlights the differential impact of sexual fantasies on individuals with and without SD. While fantasies positively affect sexual satisfaction and quality of life in healthy individuals, this effect is diminished in those with SD. The findings emphasize the need for a nuanced approach to addressing sexual fantasies in clinical practice, particularly for patients with SD.
Introduction
Sexual fantasies refer to thoughts, narratives or mental images that affect sexual arousal and play a role in enhancing emotional and physical excitement during sex; that is, they have a drive-facilitating role in sexual activity. 1 However, fantasies can often feel intrusive and become a source of guilt, shame and negative self-image. These fantasies may not necessarily be paraphilic or “deviant,” but include common ones such as imagining another person during sex or wanting to be dominated. 2 Fantasies are integral to sexual desire and are part of the diagnostic criteria for male Hypoactive Sexual Desire Disorder (HSDD) and Female Sexual Interest/Arousal Disorder in the DSM-5. 3 Fantasies also help in maintaining arousal and reaching orgasm and have often been used as a part of clinical intervention in both, erectile dysfunction (ED) and HSDD.4,5 However, to what degree fantasies and sexual well-being are related to each other and in what ways they are independent is one of the driving questions for our research.
This study explores the relationship between sexual fantasies and sexual well-being, focusing on individuals with sexual dysfunction (SD group) compared to healthy controls.
Methodology
This study aimed to explore the relationship between sexual fantasies, SD, and sexual well-being. The study was passed by the ethics committee of our institute (Reg no. ECR/748/inst/MP/2015/RR-18) in 2018. Our cases comprised of patients presenting with sexual health concerns at the outpatient department (Department of Psychiatry) who met the DSM-5 criteria for SD.
Diagnosis of ED or premature ejaculation (PME) was made by the primary author of the study and one more clinician separately. Patients who satisfied the DSM-5 criteria for diagnosis for both ED and PME were grouped together as sexual dysfunction or SD group. Patients with histories of neurodevelopmental disorder, major psychotic illness or any chronic medical illness and the ones who did not agree to consent were excluded from the study. The controls were derived from healthy and sexually active relatives, wards and friends of patients visiting various OPDs and were matched for age, gender, education level, etc.
We went for a convenience sampling method as people are reluctant to talk about sex related issues, so patients coming to us with sexual complaints made for the most approachable population available to us. To calculate the sample size we used the formula, n = [Za √P(1-P)/d]2 and where the confidence interval (Z) was taken as 1.96 and prevalence (P) of low endorsement of sexual fantasies in people with average SSS (in past one month) was taken as 0.08. This was based on previous campus surveys conducted by our department in the past. The estimated sample size according to the formula came to 104.
We carried out the survey till we reached 100 respondents in SD and control groups, both. After making the DSM-5-based diagnosis, consent was taken, and responses were filled by both groups. Responses were collected anonymously in two ballot boxes (one for cases and one for controls). The research was set in a medical college hospital in the central Indian state of Madhya Pradesh, and data were collected over a year. Informed consent in Hindi or in English was taken from each respondent, and a briefing regarding their anonymity and the ballot was given. Subjects were asked to present any queries they might have to the experimenter whenever necessary. The following assessment tools were used to collect responses:
Arizona Sexual Experience-Male (ASEX-M) Scale is used to quantify SD. It is a 5-item scale to quantify different stages of the sexual response cycle and identify ED or PME. Scores range from 5 to 30. Higher scores indicate more severe dysfunction. A validated Hindi translation of ASEX-M was provided to subjects who were more comfortable with Hindi.
Wilson’s Sex Fantasy Questionnaire (WSFQ) comprises 40 items descriptive of sexual fantasies and fetishes that fall into four major domains: intimate, exploratory, impersonal and sadomasochistic. Against each item is a 5-point Likert scale ranging between “have never fantasised about” (0) and “have fantasised about very frequently” (4). The score range falls between 0 and 160. A Hindi translation of WSFQ was prepared in our department with appropriate permissions and was provided to any subject who wished to respond in Hindi.
Sexual Quality of Life (SQoL) Scale-Male consists of eleven negatively constructed statements like, “when I think of my sexual life, I feel guilty” or “embarrassed” or “angry,” etc. The responses against the statements are taken on a six-point Likert-type scale ranging between “completely agree” and “completely disagree.” Higher scores show better sex related quality of life. A validated Hindi translation of SQoL was provided to subjects who were more comfortable with Hindi.
All the subjects were asked to mark their SSS levels in the last six months on a scale of one to ten, ascending towards “complete satisfaction” at ten.
All data collected were analysed using descriptive statistics. Mean and percentage were used to represent the data. Correlation coefficients were calculated to explore the relationship between total WSFQ and SQoL scores in both the SD group and control groups. Two-way ANOVA tests were conducted with SD status (present or absent) and graded WSFQ scores as fixed factors, and SSS, ASEX, and SQoL scores as dependent variables.
To ensure anonymity, subjects were not required to provide personal details on the questionnaire forms.
Results
Socio-demographic Profile
All our cases (SD group) and Controls were matched with regard to age, marital status, sexual activity, education, and religion. The SD group had a mean age of 30.18 years (±7.81), and the control group had a mean age of 29.88 (±6.86). The majority of the subjects were currently married, had higher secondary or better education, had urban residence, were Hindus, and were sexually active.
Comparison of WSFQ Scores Between SD Group and Controls
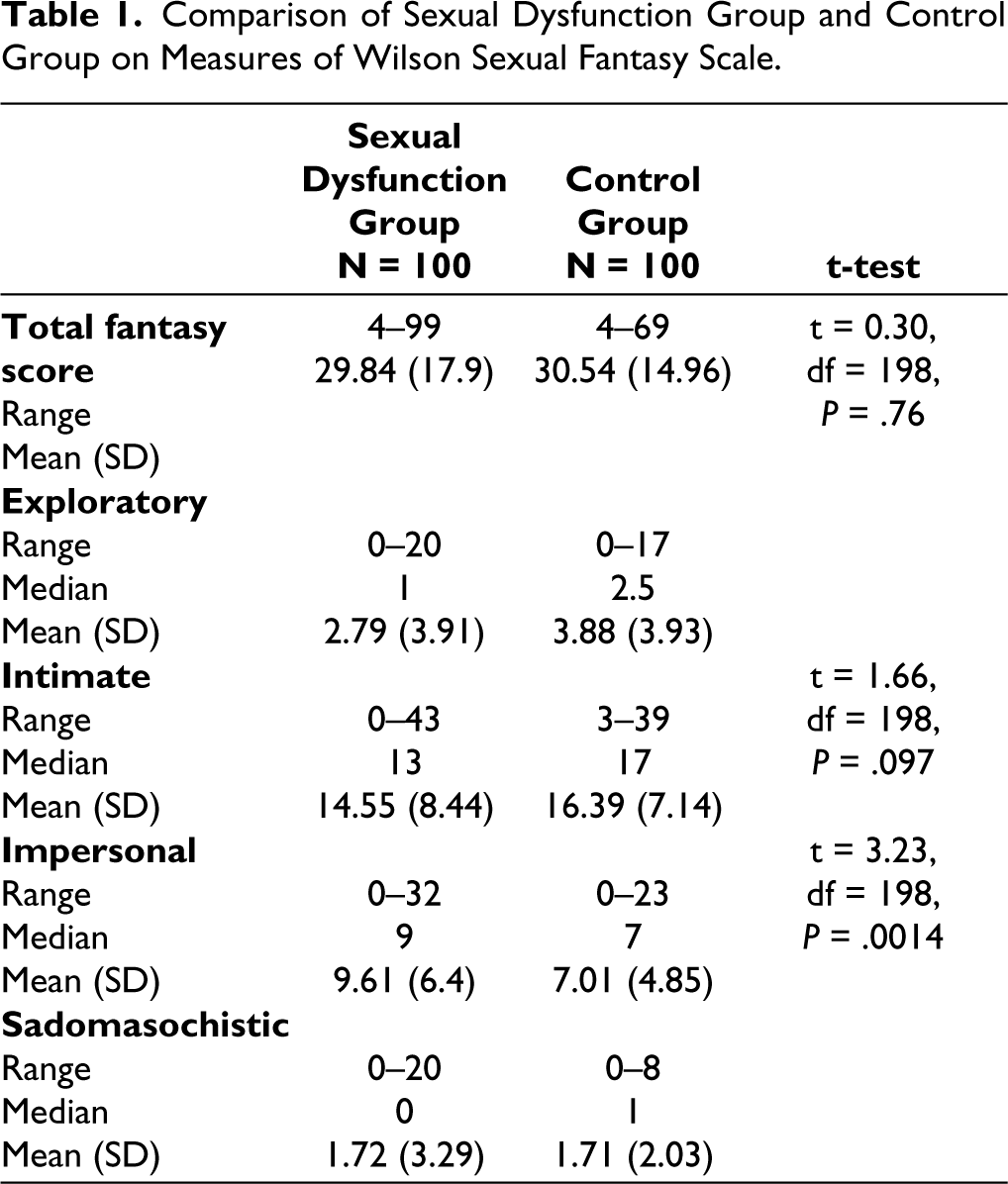
The mean WSFQ scores of the SD group and the controls were comparable and bore no significant statistical difference. Among the mean scores of both groups in the four domains of WSFQ, though, a statistically significant difference was noted in the intimate and impersonal domains. The control group scored significantly higher in the intimate fantasies domain, while the SD group scored significantly higher in the impersonal domain. The responses in the exploratory and sadomasochistic fantasy domains were negligible in both groups. Scores are summarized in Table 1.
Comparison of Sexual Dysfunction Group and Control Group on Measures of Wilson Sexual Fantasy Scale.
Comparison of SD Group and Control Group Scores on SSS, ASEX, and SQoL Scales
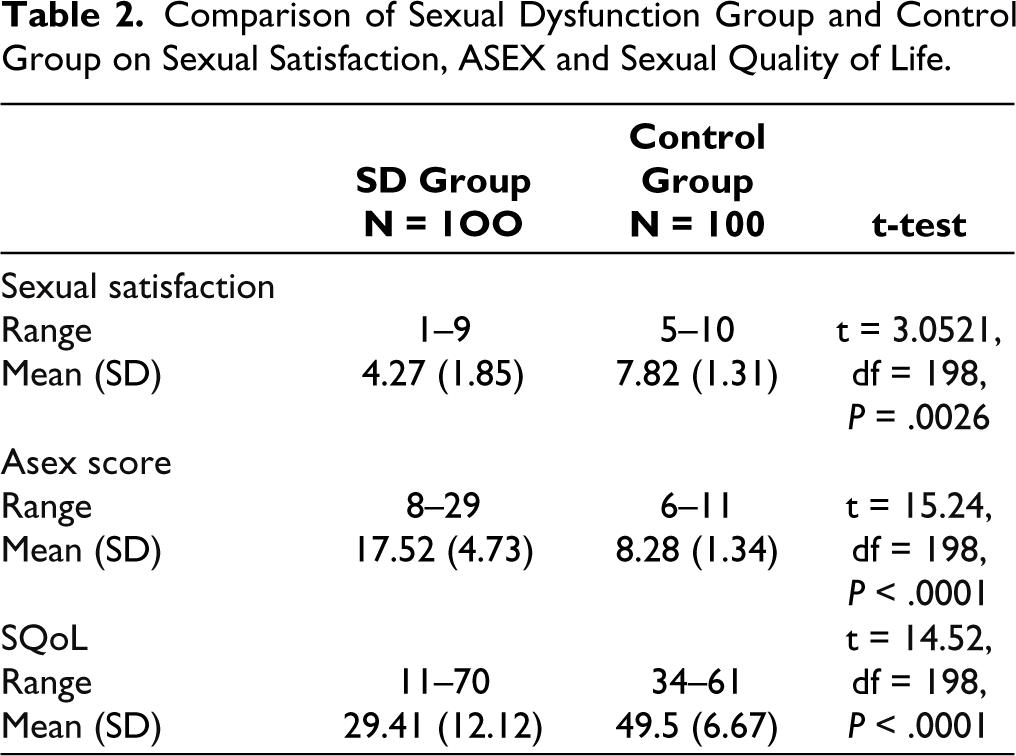
The mean scores of the SD group on the ASEX, SQoL, and SSS scales were significantly poorer than the scores of the control group. The mean scores are summarized in Table 2.
Comparison of Sexual Dysfunction Group and Control Group on Sexual Satisfaction, ASEX and Sexual Quality of Life.
Correlation Studies
In correlation studies, in the control group, we noted a strong positive correlation between WSFQ and SSS (+0.600, P = .001) and between WSFQ and SQoL (+0.459, P = .001). Also, there was a mild but significantly negative correlation between WSFQ and ASEX scores (−0.209, P = .037).
In the SD group, WSFQ scores had no correlation with SSS, SQol, or ASEX scores, but ASEX was negatively correlated with SSS (−0.290, P = .003) and SQol (−0.245, P = .014). While SSS and SQoL scored a positive correlation (0.329, P = .001).
ANOVA Studies
We performed two-way ANOVA tests to see how SSS, ASEX, and SQoL scores are affected at different levels of WSFQ scores in the SD group and controls. Two-way ANOVA tests were performed by taking the presence/absence of SD (Sexual Function Status [SFS]) and graded WSFQ scores as fixed factors against SSS, ASEX, and SQoL scores as dependent variables separately.
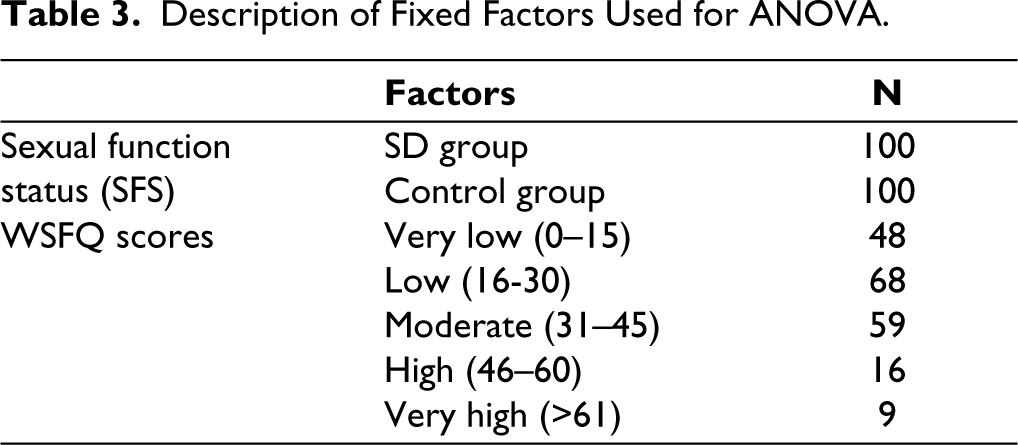
Fantasy scores were divided into categories in the following way, taking the standard deviation of the control group’s mean fantasy score as reference (approx. 15). The values are listed in Table 3, and the results are summarized in Table 4.
Description of Fixed Factors Used for ANOVA.
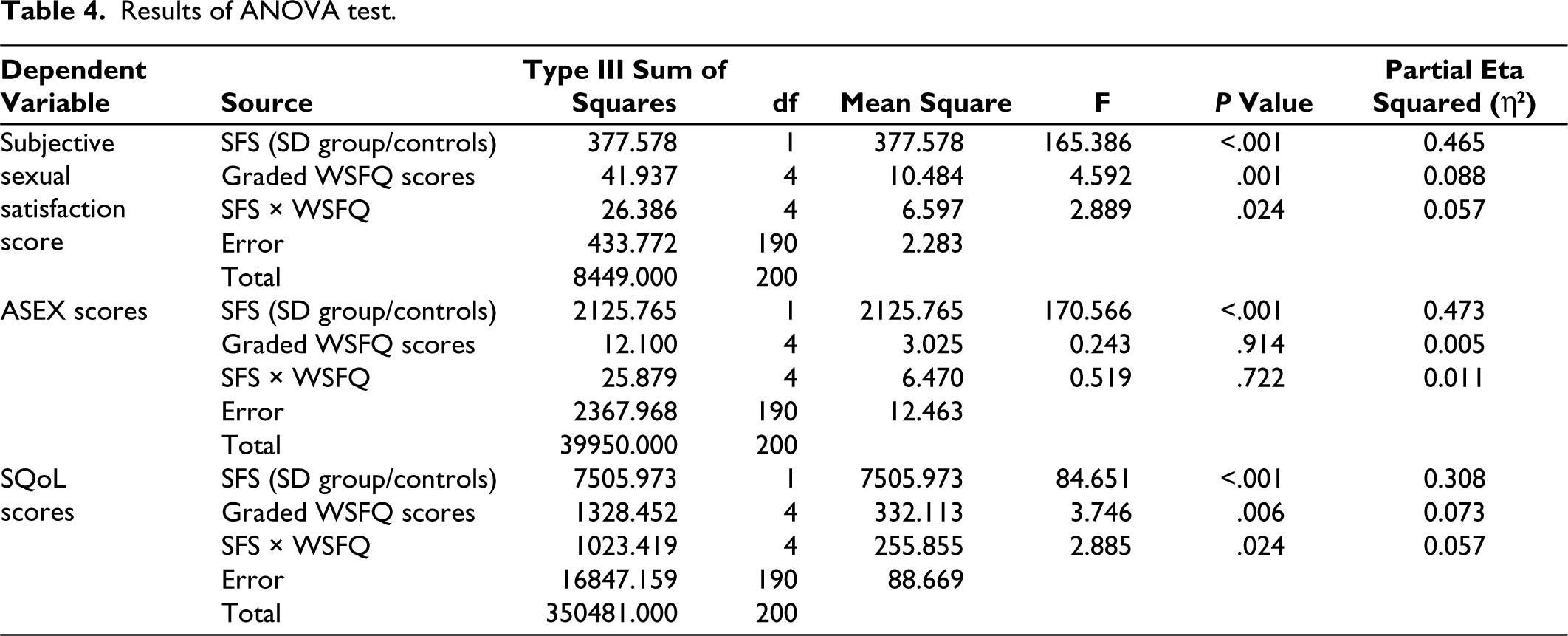
Results of ANOVA test.
Two-way ANOVA with Sexual Satisfaction as the Dependent Variable
Taking SSS scores as the dependent variable we observed a significant main effect of SFS on SSS scores. The presence or absence of SD imparts statistically significant variance of 46.5% on SSS scores (F = 165.386, P < .001, η2 = 0.465). WSFQ scores also showed a significant main effect (8.8%) on SSS scores (F = 4.592, P = .001, η2 = 0.088).
We also found significant interaction effect between SFS and WSFQ on SSS scores Interaction between factors tells us how much of the difference between the SSS scores of both groups seems to depend on WSFQ scores, that is, 5.7% (F(4, 190) = 2.889, P = .024, η2 = 0.057).
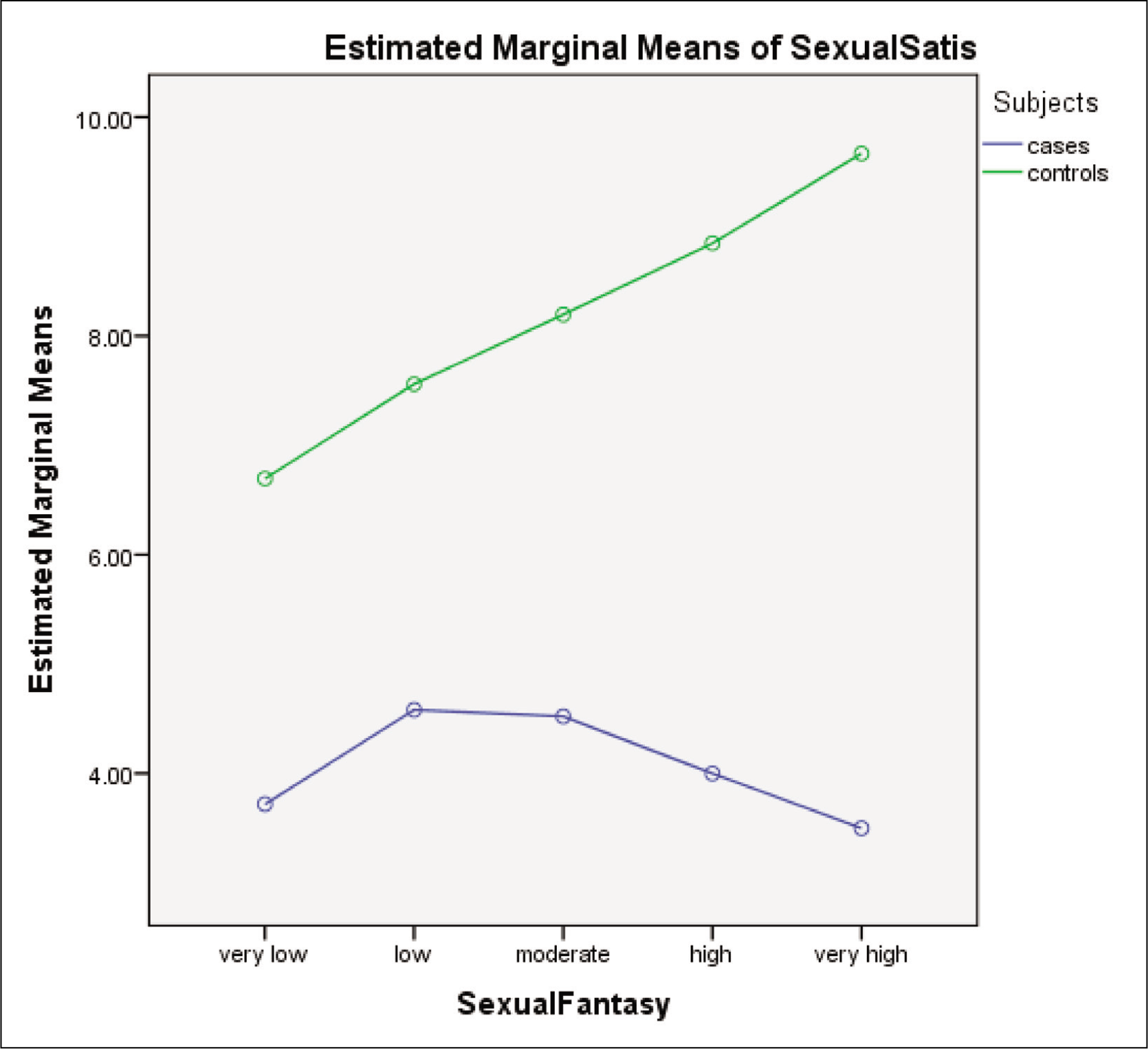
The following profile plot (Figure 1) illustrates the effect of interaction between SFS categories (cases/controls) and WSFQ score levels on SSS scores.
Estimated Marginal Means Profile Plot with SSS Scores as Dependent Variable. In This Plot, We See a Strong Positive Linear Association Between SSS Scores at Each Increasing Level of WSFQ Score Among the Controls. In Cases, the Sexual SSS Levels Rise Initially as WSFQ Level Increases, Then Plateau at Moderate Levels and Start Falling Thereafter. The Largest Difference in the Estimated Marginal Means of Satisfaction Between Cases and Controls Is Seen at the “Very High” Level of Fantasy.
Two-way ANOVA with ASEX Score as the Dependent Variable
Taking ASEX scores as dependent variable we noted that effect of SFS imparts a statistically significant variance of 47.3 % on ASEX scores (F = 170.566, P < .001, η2 = 0.473), but there was no significant main effect of WSFQ on ASEX scores (F = 0.243, P = .914, η2 = 0.005). The interaction between factors (SFS*WSFQ) also bore no effect on the variance.
Two-way ANOVA with SQoL Score as Dependent Variable
SFS imparted a 30.8% variance and had a significant main effect on SQoL scores (F = 84.651, P < .001, η2 = 0.308). WSFQ score levels account for 7.3% of variance in SQoL scores, again statistically significant (F = 3.746, P = .006, η2 = 0.073).
Significant interaction effect (5.7%) between SFS and WSFQ on SQoL scores was also noted (F = 2.885, P = .024, η2 = 0.057).
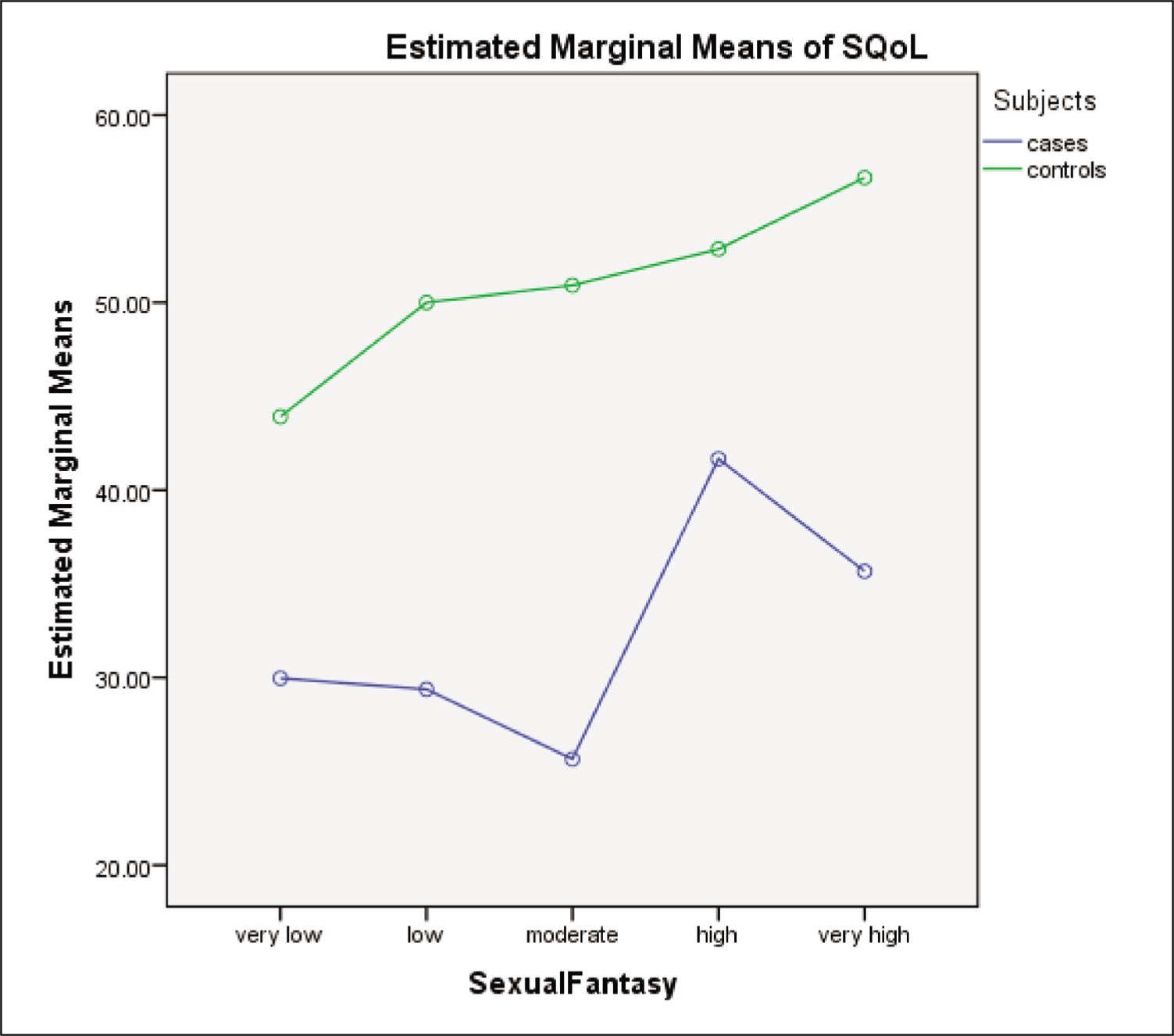
The following marginal means plot illustrates these interactions (Figure 2).
Illustrates the Effect of Interaction Between SFS Categories (Cases/Controls) and WSFQ Score Levels on SQoL Scores. The Plot Shows That the Mean SQoL Scores of the SD Group (Cases) Had the Least Difference with the Scores of Controls at High Sexual Fantasy Level.
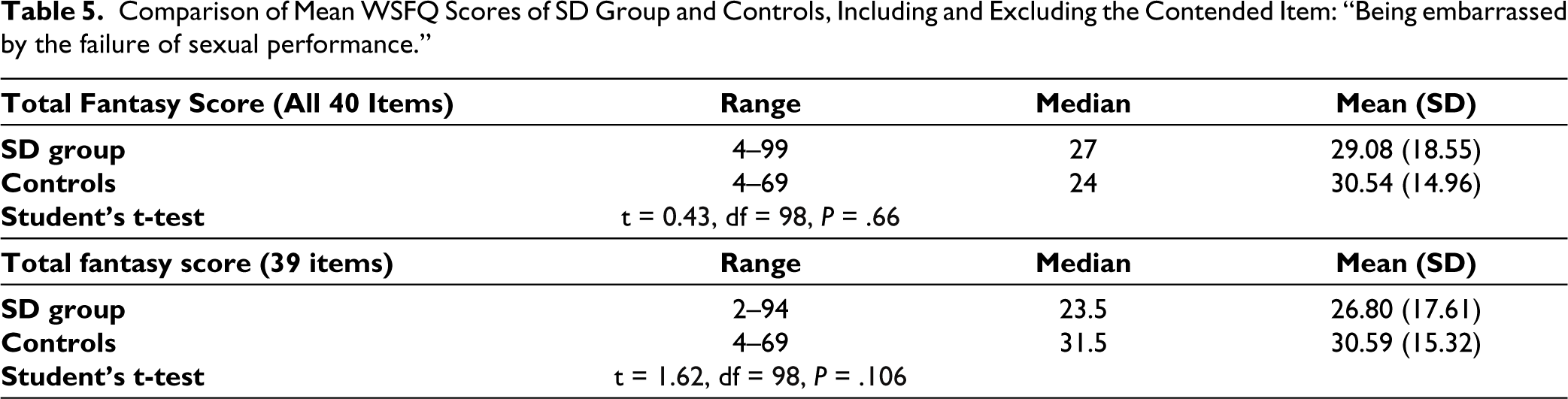
During the data collection process, 16 respondents asked for clarification of one item in the WSFQ. To see how much of an impact this potentially confusing item had on the total WSFQ scores comparison between the two groups, we calculated the difference in the scores when the item was included and when it was excluded (read discussion for further elaboration). The difference in scores is shown in Table 5.
Discussion
Socio-demographic Profile
All the subjects in the SD and control groups were matched with regard to age, marital status, sexual activity, education, and religion. Out of these demographic characteristics, the level of education has been known to influence sex related knowledge, and this, in turn, can affect sexual experience. 6 Also, increasing age has been associated with a decrease in the frequency of sex in general and penetrative sex in particular, but that is not necessarily indicative of poor satisfaction.7,8 Our subjects had a mean age of 30 years, so we can expect that age did not have a significant bearing on sexual experience in this study. The number of years of marriage, indicators of interpersonal conflict with spouse, and sexual activity outside of marriage were not noted, but these could be potential hidden variables affecting sexual satisfaction and fantasies.
A review of different scales measuring sexual function from the point of view of the dual control model of sexual response was conducted by Jenssen and Bancroft. The dual control model emphasizes studying the factors affecting both sexual excitation and inhibition in tandem. This view opens a dynamic way of interpreting the factors at play during or around sex. Jessen and Bancroft noted that partnership status, sexual orientation, porn use have varied but significant effects on sexual excitation and inhibition. 9 This becomes a major limitation in our study that we did not inquire about these factors with our subjects.
Comparison of Scores Between SD Group and Controls
The SD group scored significantly poorer in ASEX, SQoL, and SSS. Similar findings have been shown in various studies. A cross-sectional study from Nigeria that included 508 men concluded that SD was significantly associated with poor quality of life in the “social” domain; however, it did not show strong associations with physical fitness, daily activities, feelings, or change-in-health domains. 10
As for WSFQ, the Control group had better mean scores numerically, but the difference with the SD group was not significant. It is possible that some questions were misunderstood by the subjects even though they were encouraged to clarify any queries while filling out the questionnaire. For instance, an item in the fantasy questionnaire “Being embarrassed by the failure of sexual performance,” got unexpectedly high endorsement from SD subjects, who may already be feeling embarrassed due to their SD. It is possible that this question was not taken in the spirit of sadomasochistic sexual gratification. In a validation study of the Portuguese translation of WSFQ, this item showed poor reliability. 11 Poor sex related knowledge has been documented in surveys of the central Indian region where this study was based, and that may further complicate the understanding of this item in the questionnaire. 12 We compared the mean fantasy scores of SD group and controls excluding this potentially confounding item, but the difference in the means was not statistically significant, although numerically more subjects in the SD group endorsed the potentially ill-phrased item about embarrassment (humiliation) as a fantasy (Refer to Table 5).
Comparison of Mean WSFQ Scores of SD Group and Controls, Including and Excluding the Contended Item: “Being embarrassed by the failure of sexual performance.”
Domain-wise Analysis of Fantasy Scores
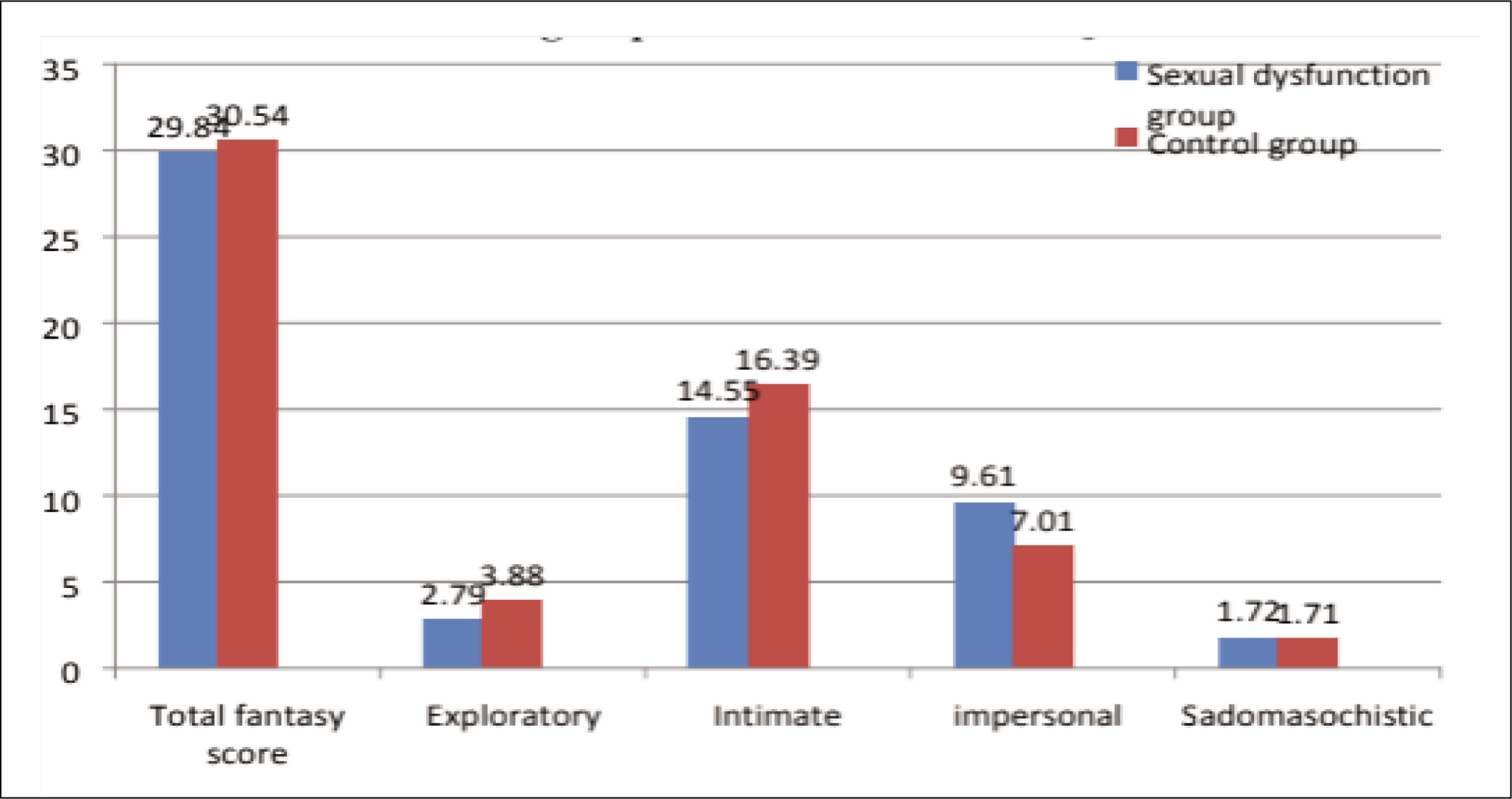
On breaking down the fantasy scores into their domains, we observed that most responses, both in the SD group and controls, fell in the intimate and impersonal domains. Responses in exploratory and sadomasochistic domains were virtually negligible (Figure 3). Also, the SD group had significantly higher scores in the impersonal domain and lower scores in the domain of intimate fantasies when compared with Controls. This is not surprising as a lack of intimacy is often observed in couples where one or both partners are suffering from SD, and most therapeutic models include intimacy-enhancing techniques as interventions. 13 Likewise, impersonal fantasies often exclude direct intimacy, and sexual gratification is achieved through fetishizing objects or through voyeuristic activities. Regarding the lack of responses in sadomasochistic and exploratory domains, similar findings were reported by Rathi et al., in their survey of sexual fantasies of men in the same central Indian region as the current study. In their survey of 151 men, the most endorsed fantasies were in intimate or impersonal domains (like passionate kissing: 86.1%, watching erotic films: 83.4%, romantic sex with loving partner: 77.5%), while sadistic and masochistic fantasies only amounted to 6.6% and 9.2%, respectively. 14
Domain-wise Comparison of WSFQ Scores in SD Group and Controls.
Sadomasochistic fantasies have mostly been studied in the context of “high risk sexual acts” and potential for sexual offence. Rossegger and Bartels, in a review of high-risk sexual fantasies, emphasize the distinction between “Sexual Fantasy” and “Sexual Fantasising.” The former is “a knowledge structure in memory” oriented towards behaviors or activities that someone finds sexually appealing, while sexual fantasizing is a cognitive process that may be initiated by a cue (like a fleeting mental image) that causes intense sexual arousal and leads to actively fantasizing. This can potentially lead to an offensive act if facilitated by factors like the level of physiological reaction and reward (e.g. orgasm), personality traits and offence-supporting beliefs of the individual. 15
WSFQ is more of a list of common sexual fantasies that surveys the frequency of each item but does not collect data regarding the cognition related to active sexual fantasizing. WSFQ and similar scales, according to Rossegger and Bartels, define sexual fantasy in “all-encompassing manner, like, ‘any sexual thought or image that is arousing’.” 15 This would mean that in the current research, we studied fantasy and not the process of fantasizing. We checked the frequency of images rather than the level of arousal response the fantasies had on the subjects. Sadomasochistic fantasies tend to show up more in research based on active engagement in sexual fantasizing than in cross-sectional surveys like ours.
Correlation Studies
We observed that the correlation between WSFQ and SSS was strong, positive and significant in controls. WSFQ scores also showed a strong positive correlation with both SSS and SQoL and a mild but significantly negative correlation with ASEX scores. In the SD group, though, WSFQ had no correlation with SSS, ASEX, or SQoL. It looks like fantasies contribute to positive sexual outcomes only in the absence of SD.
While many studies have found that fantasies tend to increase with decreasing sexual satisfaction and increasing desire (and frequency of masturbation) in men, most of these studies are based on random population samples and not specifically on dysfunctional cohorts. 16 It is also possible that below a certain threshold of sexual dissatisfaction and dysfunction, fantasies do not positively influence sexual function at all. To get a clearer answer to that, we performed two-way ANOVA tests to see how SSS, ASEX, and SQoL scores get affected at different levels of WSFQ scores in the SD group and controls.
Variance Imparted by SFS and WSFQ Scores on Different Scales
In the two-way ANOVA studies, we observed that the major variance in scores of SSS in our subjects depended on the presence or absence of SD (46.5%), but sexual fantasies also contributed to 8.8% of the variance. In the interaction of subjects and sexual fantasies, it was found that up to 5.7% of the difference in satisfaction scores between them was due to their sexual fantasy scores.
So, sexual fantasies did seem to impart an effect that contributed to the difference in SSS scores of the SD group and controls, but the correlation trend (as seen in Figure 1) of SSS and WSFQ in the SD group was not linear, like the trend in controls. As seen in the post hoc analysis, the SSS scores initially rise in the SD group with increasing WSFQ levels, then plateau and thereafter decrease as WSFQ levels further increase.
Likewise, WSFQ scores contributed to 5.7% of the difference in the scores of SQoL between the SD group and controls. While the controls showed a linear increase in SQoL scores with increasing WSFQ levels, in SD, the group SQoL scores were initially low and flat but only started to rise at higher WSFQ levels. So, it seems like fantasies do have a positive outcome in terms of sexual life quality, but satisfaction continues to decrease despite increasing fantasies.
Conclusion
Our findings indicate that while sexual fantasies positively correlate with sexual satisfaction and quality of life in healthy individuals, this relationship is disrupted in individuals with SD.
Specifically, the SD group demonstrated significantly poorer scores in sexual satisfaction (SSS), SQoL, and ASEX, compared to controls. Although total fantasy scores did not significantly differ between the groups, domain-specific differences were observed, with the SD group scoring higher in impersonal fantasies and lower in intimate fantasies.
Correlation studies revealed a strong positive relationship between WSFQ and SSS, and WSFQ and SQoL, and a negative correlation between WSFQ and ASEX in the control group. However, these correlations were absent in the SD group. ANOVA analysis further demonstrated that the presence of SD explained a significant portion of the variance in SSS, SQoL, and ASEX scores. Sexual fantasies also contributed to the variance, albeit to a lesser extent.
Our findings suggest that sexual fantasies may contribute to positive sexual outcomes in the absence of SD. However, in the presence of SD, this relationship is altered.
Future research should explore the underlying mechanisms of this relationship and consider other variables, such as interpersonal conflict, sexual activity outside of marriage, and psychological comorbidities that may influence sexual satisfaction and fantasies.
Limitations
There is an inherent limitation in a cross-sectional study like ours that presents a snapshot of the phenomenon being studied and does not reveal the process of it, like longitudinal studies do. Sexual fantasies have some stable aspects and many dynamic ones, like the process of active sexual fantasizing, which is more relevant in the context of sadomasochistic and exploratory fantasies. Our study saw a low endorsement in these domains across the SD group and controls alike. We checked the frequency of fantasy images rather than the level of arousal response the fantasies had on the subjects. A different study design would be required to clarify the relationship.
Our study did not include rated surveys of depression and anxiety, which often accompany SD, due to limited personnel and departmental resources. Though all the patients were thoroughly interviewed for diagnosis, rated scores could have made the study more robust and more nuanced associations could be studied.
This study did not include data on gender identity, sexual orientation, porn use, avenues for sex related knowledge, etc. These factors have varied but significant effects on sexual excitation and inhibition. 9 This becomes a major limitation in our study as we did not inquire about these factors with our subjects.
It is possible that some questions were misunderstood by the subjects, even though they were encouraged to clarify any queries while filling out the questionnaire. This applied particularly to one item (elaborated in the discussion section) on WSFQ. A prior screening of the questionnaire for items with poor internal consistency and their removal could add more confidence to our study.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This work was approved by the Institute Ethical Committee (IEC) of our Institute (Reg no. ECR/748/ inst/MP/2015/RR-18) in 2018.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
The participant has consented to the submission of the article to the journal.