
Abstract
Introduction:
Sexual disorders are practically not addressed in community and primary care settings in India. Understanding the profile of patients visiting tertiary care centers’ psychosexual clinics (PSC) may be of value, to map some critical gaps in the service utilization.
Aim:
To understand the demographic profile and presenting complaints of patients with psychosexual disorders visiting a PSC.
Methods:
An audit of patients’ case records, diagnosis based on ICD-10 classification system, in a PSC over last 1 month was done, noting demographic factors and their frequency distributions.
Results:
Out of 55 patients visiting the clinic, most common age group was 21 to 30 years (49.09%) and only 2 were females. Maximum patients had education up to higher-secondary level (69.09%), were married (65.4%), and had a sexual partner during past 3 months (70.09%). Premature ejaculation (occurring singly or along with other sexual disorders) was diagnosed in 45.28% patients.
Conclusion:
Further exploration is needed into the services provided by the PSC. There is scope for sensitizing female patients, customizing psychoeducation suitable to the educational status and work holistically in the PSC.
Introduction
Sex has been identified as one of the basic needs of human being and it finds an important place in literature, right from the Darwinian theory of evolution to Maslow’s hierarchy of needs. Sexuality is considered as an important aspect of health and well-being. 1 Various cultural and religious endorsements and assumptions have influenced understanding and expressions of sexuality to a great extent. Sex, as an integral part of health, is not yet an appreciated subject. Hence, even if sexual health issues are common in India, they are very less attended and systematically researched. In spite of being very common, psychosexual disorders remain missing in major epidemiological studies. 2 It is important to note that traditional Indian systems of medicines have percolated to the grassroots level, as they share complex connections with Indian culture, traditions, and mythology. Certain myths related to cultural sanctions may have played a role in syndromes like Dhat syndrome. There is evidence that patients suffering from common sex-related symptoms often prefer practitioners of Indian systems of medicine more than allopathic doctors. 3
In modern medicine service framework of India, services for sexual health are often delivered mostly at tertiary level of specialized care. These may be psychiatry and urology departments of tertiary hospitals or attributed departments of sexual medicine, which are very meagre. Secondary, primary, and community health services for sexual complaints are practically nonexistent in India. For a greater understanding of these missing bridges, along with larger community studies, it is also very important to understand the current sexual health service uptake at tertiary centers of care. This may give us an idea of shortcomings in our service delivery and pave further in-depth research into the problems.
Although practice guidelines for treatment of sexual disorders have been stated in literature for practice in India, 4 there are no clear cut algorithms about referral to specialized services for psychosexual complaints. Thus, a study to understand the profile of patients visiting a specialized psychosexual clinic (PSC) may be valuable to begin mapping of critical gaps in the existing service framework.
Aim
To understand the demographic profile and common presenting complaints of patients visiting PSC of a tertiary care center.
Methodology
Study type and setting: The study is an audit of the case record forms of patients visiting specialized PSC of a tertiary care hospital in Mumbai. The Department of Psychiatry has been catering to a wide population of western part of Maharashtra for more than 35 years. In spite of absence of any well-arrived consensus on transferring patients with psychosexual complaints to specialized clinics, the department had set its standard practice of referring patients to this PSC. All those patients in whom a primary diagnosis of psychosexual disorder is made (based on International Classification of Diseases, ICD-10 system) or current most distressing complaints are related to sexual functions, are encouraged to follow-up in the specialized PSC held once in a week.
Study duration and population: The case records of all those patients that visited the PSC over the month of December 2019 were noted, which gave a sample of 55.
Study tool: The PSC standard case records forms consisted of information on demographic profile, sexual complaints, and diagnosis of the patients, which was noted.
Data analysis: A descriptive analysis of the dependent variables was made.
Results
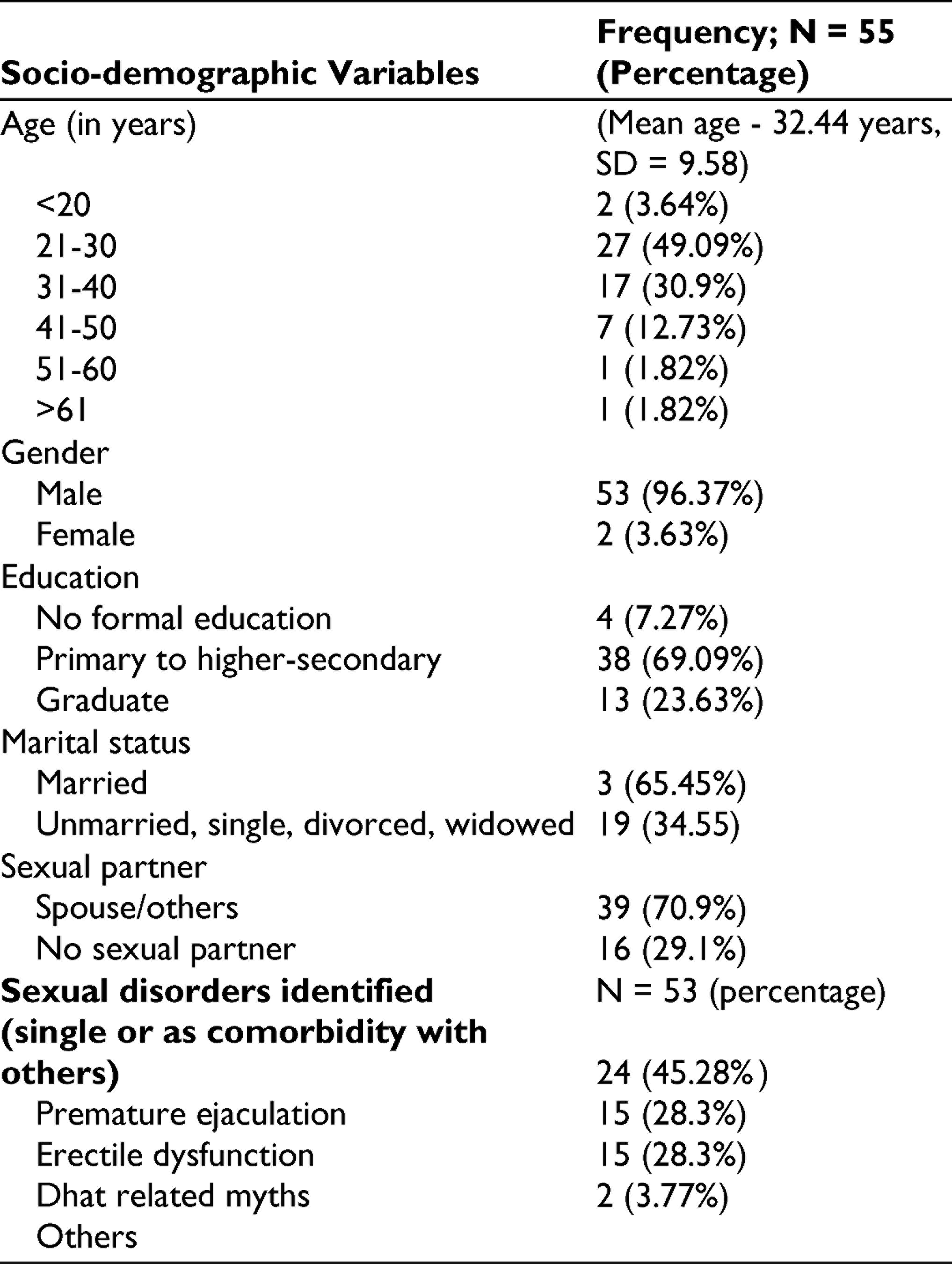
This study was carried out in a specialized PSC of a psychiatry department which is held once in a week. On an average of daily 3 to 4 patients from general psychiatry outpatient department are referred to this PSC, amounting to 75 to 100 patients referred in a month. However, only 55 patients turned up in the PSC in the given month. As shown in Table 1, the maximum number of attendee patients was in age group 21 to 30 years. Out of 55 patients, only 2 of them were females. Maximum patients had educational level of higher secondary (38 out of 55, 69.0%) and the least were illiterate. A total of 34.5% (19 out of 55) patients had never been married. A total of 29.0% (16 out of 55) patients did not have any sexual partner since last 6 months. A total of 37.7% (20 out of 53) patients had 2 or more sexual disorders occurring together. Maximum patients presented with complaints suggestive of premature ejaculation (PME) (45.3%), alone or in combination with other symptoms. This was followed by erectile dysfunction (ED) (28.3%) and Dhat syndrome (28.3%).
Socio-demographic profile and sexual disorders identified in patients visiting psycho-sexual clinic of a tertiary care centre
Discussion
The discrepancy between patients referred to PSC and those actually attending it, necessitates further evaluation of the barriers to attend a specialized clinic. Sexuality is influenced by many cultural and religious sanctions and its disorders are often considered shameful and stigmatizing. People are hesitant about seeking appropriate and timely help. Also lesser understandings and misconceptions about modern medical practice may be a contributory factor for which individuals resort to traditional Indian Systems of Medicine instead. 5
In this study, maximum patients were found to be in age group 21 to 30 years. In a larger epidemiological study in South India, 6 which was carried out by a door-to-door survey, maximum prevalence of sexual disorders was found in 41 to 60 years age group. Also a few other researchers7,8 have shown that prevalence of sexual disorder increases with age. This discordance in our study could have been because of more help-seeking behavior in this young age group. This could also be probably because these years of age are the early years of active sexual life and people, then, may have been more concerned about their sexual complaints than the older age groups. This needs further research which may help us promote help-seeking behavior.
Strikingly, we had only 2 female (3.6%) patients visiting PSC against 53 male patients (96.3%). Pal et al 9 and Arafat and Ahmed 10 found similar pattern of very low number of female patients attending such clinics in eastern India and Bangladesh, respectively. Studies in Western countries 11 suggest sexual disorders being more common in females, compared to males. Also, a community epidemiological study in South India 6 revealed around 14% of the female subjects being diagnosed to have female sexual disorders. This discrepancy between prevalence of female sexual disorders in community and those attending a sexual clinic calls for further in-depth assessment of factors preventing help-seeking behavior in Indian female patients and inadequacies in women-friendly orientation of available services.
Out of all the patients attending the PSC, maximum number of patients (38, 69.0%) had an educational level of higher secondary while those with no formal education constituted only 4 (7.3%) of the total attendees. In a community-based study in South India, 6 up to 29.5% of the total illiterate population had at least 1 sexual disorder. The meagre percentage of illiterate patients in attendees could have been because of lack of awareness about medical treatments, stigma, or greater confidence on traditional systems of healing. We may also need to investigate further if the social determinants that are usually associated with low educational level, have any bearing in help-seeking behavior for sexual complaints in illiterate individuals.
A total of 65.4% (n = 36) of the patients in our study were married as against 34.5% (n = 19) who were never married. Similar finding is seen in other community and hospital-based studies9,12-14 in India. In our study, 29.0% (n = 16) had no sexual partners during last 6 months. This may indicate that self-perception of sexuality is a major distressing factor for an individual leading to sexual dissatisfaction and complaints. Role of peer influences also cannot be ruled out. It would be interesting to research further about how does sex influence self-esteem and concept of well-being.
Further assessment of sexual disorders was done on only males (N = 53) due to inadequate representation of female patients. It was valuable to understand the subset of sexual complaints that present most commonly in PSC. On assessment of sexual complaints, 37.7% (20 out of 53 patients) had 2 or more psychosexual disorders occurring together. In our study, maximum patients were found to have PME, alone or in combination, whereas in community-based study 14 in North India, self-perceived defects in semen, loss of libido, and masturbation guilt were much more prevalent than PME and ED. In community-based study in South India, 6 ED (15.8%) was found to be most common than PME (8.8%). Referring to community studies here is especially important, as it may indicate the pattern of symptoms for which individuals seek help in specialized clinics. In a similar study in Bangladesh, 10 29% of the patients visited PSC only for misconceptions related to sex. In our study, it may also be possible that most of the complaints that are related to myths, self-perceptions, and culturally unsanctioned practices like masturbation are either normalized, unattended, or consulted with either traditional systems of medicine or quacks.
Conclusions
This study strongly indicates the need for further exploration into tertiary and specialized care settings for psychosexual disorders. A lesser attendance rate of female patients hints toward need for more women-friendly settings. Higher attendance rate of young adults and its contradiction to the community prevalence of psychosexual disorders in this age group, suggests need for in-depth understanding of health seeking behavior in psychosexual disorders.
It is concerning that, not only do the primary and community settings lack in appropriate services for sexual health but also the tertiary settings that have large lacunae. This includes lesser attendance rates of patients to such specialized clinics and discordance of demographic profile of individuals affected by sexual disorders in community and as represented in a specialized PSC. It is important to note that, it is not just the provider side to be a discussant but also the users, as a greater understanding of the users’ attitudes toward sexuality in general and psychosexual disorders in particular is required.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.