
Abstract
Background:
Sexual dysfunction is common in patients with psychiatric disorders and also considered as a known adverse effect of psychotropic medications.
Aim:
This study aimed at delineating the sociodemographic and clinical correlates of various types of sexual dysfunction among psychiatric patients receiving psychotropic medications.
Materials and Methods:
It was a cross-sectional hospital-based study conducted at Institute of Mental health and hospital, Agra. The sample consisted of 210 married psychiatric patients of both the genders between the age range of 20–59 years who were on regular treatment with psychotropic medications for at least three months at the outpatient department (OPD) of the institute. The patients having sexual dysfunction before the start of psychotropic medications were excluded from the study. The International Index of Erectile Function (IIEF) and the Female Sexual Function Index (FSFI) were used.
Results:
Age, duration of illness, duration of treatment, and occupation were significantly associated with erectile dysfunction, intercourse dissatisfaction, orgasmic dysfunction, sexual desire dysfunction, and overall dissatisfaction in male patients but medicine compliance was associated with sexual desire dysfunction only. Education, domicile, and socioeconomic status were not associated with any of the sexual dysfunction domains in male patients. Age, duration of illness, and duration of treatment occupation were significantly associated with desire, arousal, lubrication, orgasm satisfaction, and pain in female patients. Medicine compliance was also associated with each dysfunction except arousal dysfunction. Education, domicile, and socioeconomic status were not associated with any of the sexual dysfunction domains in female patients.
Conclusion:
The results of this study clearly suggest that the demographic variables of age, occupation and clinical variables of duration of illness, and duration of treatment are significantly associated with sexual dysfunction in both male and female patients. Medicine compliance is a significant factor in female sexual dysfunction more than that is seen in male patients. Both clinical and nonclinical variables contribute to the sexual dysfunction in the psychiatric patients.
Keywords
Introduction
The phases of the sexual response cycle include excitement, plateau, orgasm, and resolution. 1 Sexual dysfunction can occur in any of the phases of the sexual response cycle. 2 The prevalence estimate of sexual dysfunction in the general population is 31% in men and 43% in women. 3 Similar prevalence was reported in other studies.4,5 In an international survey of 13,882 women and 13,618 men aged 40–80 years from 29 countries, it was found that the reported prevalence of sexual problems was higher in East Asia and Southeast Asia than in other regions of the world. 6 In India, one study reported that the prevalence of female sexual dysfunction was 55.55% and the other study showed that 68.32% of female patients were having sexual dysfunction. 7 General medical illness, gynecological problems, psychological and emotional factors, and use of various medications were found to be the known causes of sexual dysfunction. 8 The participants who had diagnosed medical illness were 4.90 times more likely to have sexual dysfunction than the participants who did not have such illness. 9
From a psychiatric point of view, sexual dysfunction might arise from psychopathology of psychiatric disorders, psychotropic medications, substance use, and psychosocial issues.10,11 The psychiatric patients are more vulnerable to sexual dysfunction. In half of the patients with schizophrenia, sexual dysfunction was attributed to the nature of illness itself.12,13 Seventy-eight percent patients with depression, up to 80% patients with anxiety disorders, and 30%–60% patients with schizophrenia were reported to have one or the other sexual problems. 14 In depressive disorder, posttraumatic stress disorder, and schizophrenia sexual desire were the most affected phase of the sexual response cycle. Patients with obsessive compulsive disorder (OCD) and anxiety disorders most frequently reported dysfunction in the orgasm phase. 15 Anxiety, schizophrenia, and depression are the most common neuropsychiatric disorders in patients with sexual dysfunction. 16
Substance use also leads to sexual dysfunction. Twenty-six percent of alcohol users were found to have sexual dysfunction. Of these, males had about 72% of dysfunction. 17 Fifty percent smokers with more than 20 cigarettes per day had sexual dysfunction.12,18,19,20 In a systematic review of Indian studies on patients with substance use disorders, 22.2%–76% patients with alcohol dependence and 40%–90% patients with opioid dependence were reported to have sexual dysfunction. 21
The studies have shown that sexual functioning has different neurophysiological mechanisms. 22 Various neurotransmitters such as dopamine, acetylcholine, and nitric oxide serotonin and norepinephrine play an important role in sexual functioning.23,24 Psychotropic medications used in the treatment of psychiatric disorders act as antagonists or agonists to various neurotransmitters to reduce or interfere with sexual functioning. 14 The researchers have viewed sexual dysfunction as the side effects of use of various psychotropic medications. 25 The prevalence of sexual dysfunction in patients on antipsychotic medication varies from 18% to 96%. 26
Antidepressants and antipsychotics are associated with sexual dysfunction. It is reported that sexual dysfunction occurs due to both typical and atypical antipsychotics. 27 Conventional antipsychotic medications are dopamine blockers and 30%–60% of patients using these medications experience disturbances of sexual function. 28 The combination of typical and atypical antipsychotics produced greater sexual dysfunctions than the atypical antipsychotics alone. 29 Risperidone increases the prolactin levels, produces menstrual disturbances, galactorrhea, erectile dysfunction, and decreased libido. 30 Research findings have also suggested that the medications such as benzodiazepines, carbamazepine, and phenytoin are also associated with sexual dysfunctions.31,32
In patients attending a sexual dysfunction clinic, sexual dysfunction occurred in 45% of patients taking antipsychotic medication. 33 The patients on neuroleptics are reported to have sexual dysfunction to the extent of 60% in men and 30%–93% in women. Thioridazine was found to produce maximum dysfunction.34,35 The factors that are significantly associated with sexual dysfunction include being on typical antipsychotic treatment, being on psychiatric treatment for 24 months and more, moderate level of alcohol use, and being aged 35 and above. 9
Sexual dysfunction is common in both the general and psychiatric population. In India, the patients still find it difficult to openly discuss their sexual problems. The delineation of associated factors do alert the clinician to consider the presence of sexual dysfunction. Hence, it is essential to catalog the factors associated with sexual dysfunction including the psychotropic medications.
Aim
This study aimed to find out the sociodemographic and clinical correlates of various types of sexual dysfunction among psychiatric patients receiving psychotropic medications.
Materials and Methods
This is a cross-sectional hospital-based study conducted at Institute of Mental Health and Hospital, Agra (IMHH). This study sample consisted of 210 married psychiatric patients of both the genders who presented at the outpatient department (OPD) of the institute for consultation. The following inclusion and exclusion criteria were followed:
Inclusion criteria: (a) The psychiatric condition was diagnosed by the psychiatrist as per the International Classification of Diseases, Tenth revision (ICD-10) criteria; (b) patients aged between 20 and 59 years who were on regular treatment with psychotropic medications for at least three months; (c) patients having sexual activity for the past one month; and (d) patients who gave informed consent.
Exclusion criteria: (a) Patients with acute psychopathology who were not stable enough to co-operate in the process; (b) patients who were having sexual dysfunction before the start of psychotropic medications.
Tools
The following tools were used in this study to get information about sexual functioning.
The International Index of Erectile Function (IIEF)
It is a widely used, multidimensional self-report instrument for the evaluation of male sexual function. The IIEF consists of 15 questions (Q), rated on a scale of 0–5, with 0 indicating no sexual activity or no attempt. It has five domains: Erectile dysfunction (Q1–5, 15), orgasmic function (Q9, 10), sexual desire (Q11, 12), intercourse satisfaction (Q6–8), and overall satisfaction (Q13, 14), each addressing a unique dimension of sexual function. The higher scores indicate better sexual functioning. The reliability coefficient (Cronbach’s α) is 0.921. 36
Female Sexual Function Index (FSFI)
This is a widely-used measure of female sexual function. It was developed as a brief, multidimensional self-report instrument for assessing the key dimensions of sexual functions in women. 37 It assesses six domains: desire, arousal, lubrication, orgasm, satisfaction, and pain. Validation studies in women aged 21–70 have demonstrated excellent internal consistency and two to four weeks test–retest reliability for each subscale. Discriminant validity was significant for all subscales, as well as the summary score.
The proposal was cleared by the institute’s ethics committee. The patients presenting at the OPD of the institute were screened on the inclusion/exclusion criteria. The patients who met the criteria were approached and called to the consultation room for a detailed interview. The interviews were conducted by the consultant psychiatrist and research staff and assurance was given to maintain confidentiality. Informed consent was obtained. Patient’s socio-demographic details, clinical diagnosis, psychotropic medications being received, duration of treatment etc. were recorded using a sociodemographic sheet specifically designed for the study. Medicine compliance was assessed through specific questions. Then the above-mentioned tools were administered individually on the participants by the last author (SM). Since the tools were in English, the items were rated by interviewing the participants.
Results
Table 1 shows that the number of female patients was more than the male patients. Majority of the patients were in the age range of 20–39 years. The education level was similar in both male and female patients. The mean and SD of duration illness of the male patients were 9.54 ± 3.55 years and 7.81 ± 4.77 years in females. The mean and SD of duration treatment of the male participants were 8.32 ± 3.70 years and 6.68 ± 4.13 years in females. Majority of female patients were not working and the socioeconomic status was low in greater numbers of female patients. Almost equal number of patients hailed from rural communities in both males and females.
Sociodemographic and Clinical Characteristics of Participants .
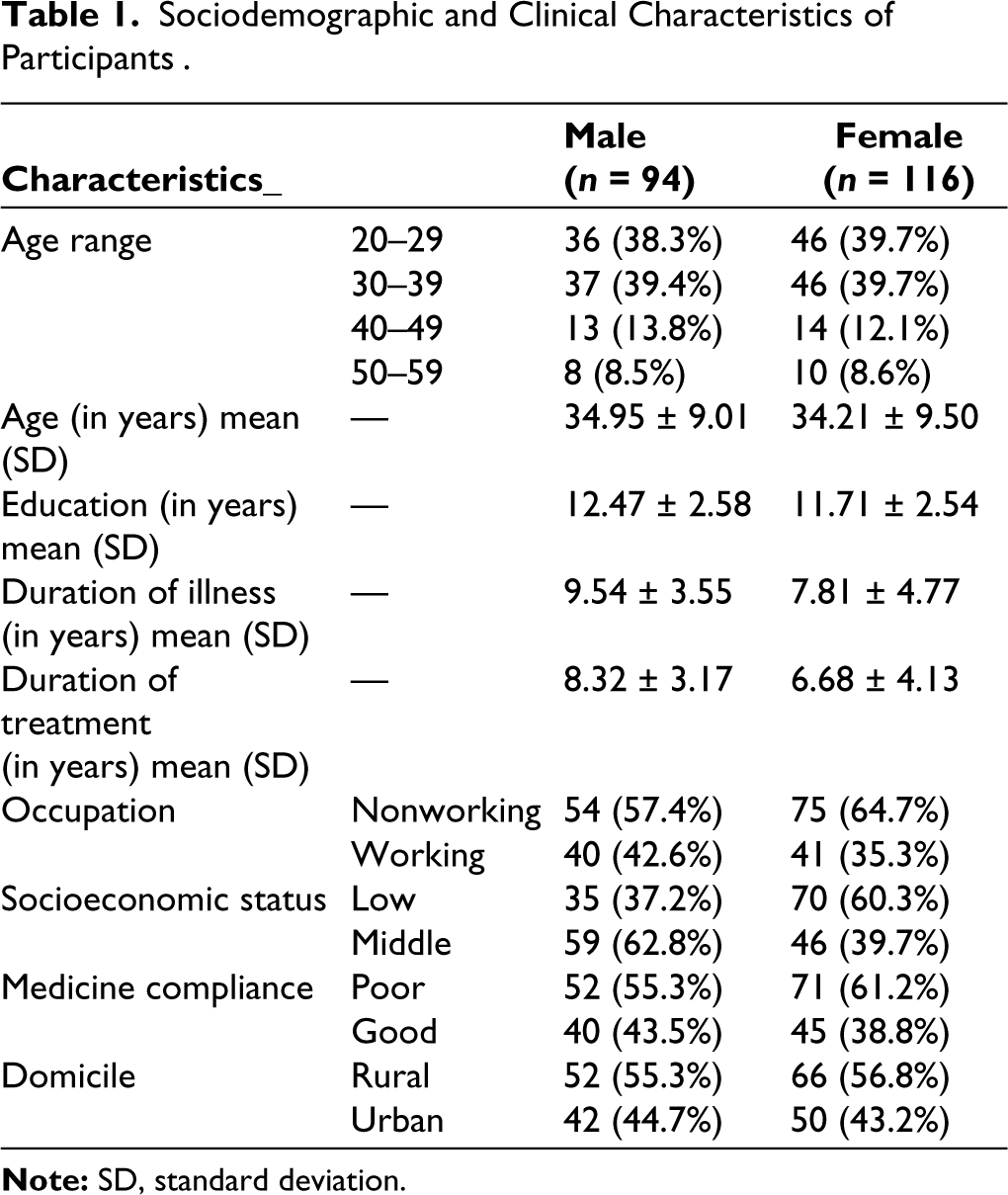
Table 2 describes the types of sexual dysfunction across gender. In male patients, overall dissatisfaction was 22.8%. Erectile dysfunction was the highest (47%) followed by desire and orgasmic dysfunction. Intercourse dissatisfaction was least prevalent. In female patients, lubrication (35.1%) and desire dysfunction (28.8%) were the most prevalent. The other dysfunctions, arousal, orgasmic, satisfaction, and pain, were reported in 11.3%–18.5% of female patients.
Sex Distribution of the Various Forms of Sexual Dysfunction.
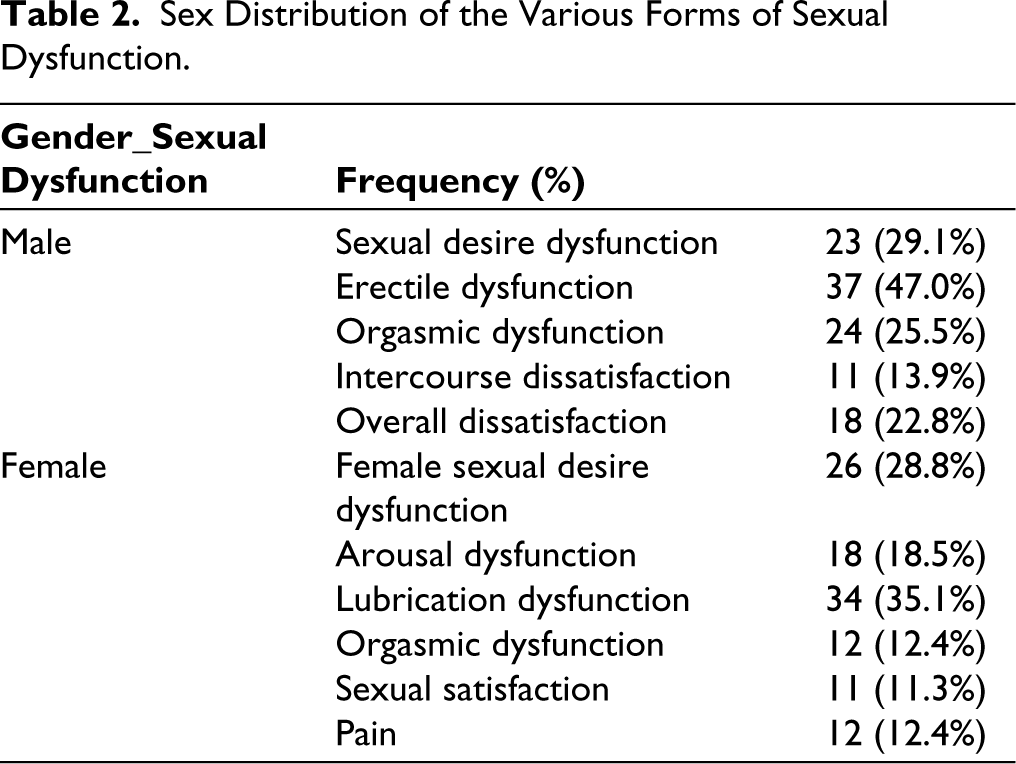
Table 3 shows the clinical and medication-related characteristics of the participants. Most of the patients had a diagnosis of schizophrenia in both the genders. There was no patient of substance use in the female sample. Majority of the patients, 33% males and 25.9% females, were on typical antipsychotics plus trihexyphenidyl.
Clinical and Medication-related Characteristics of Participants.
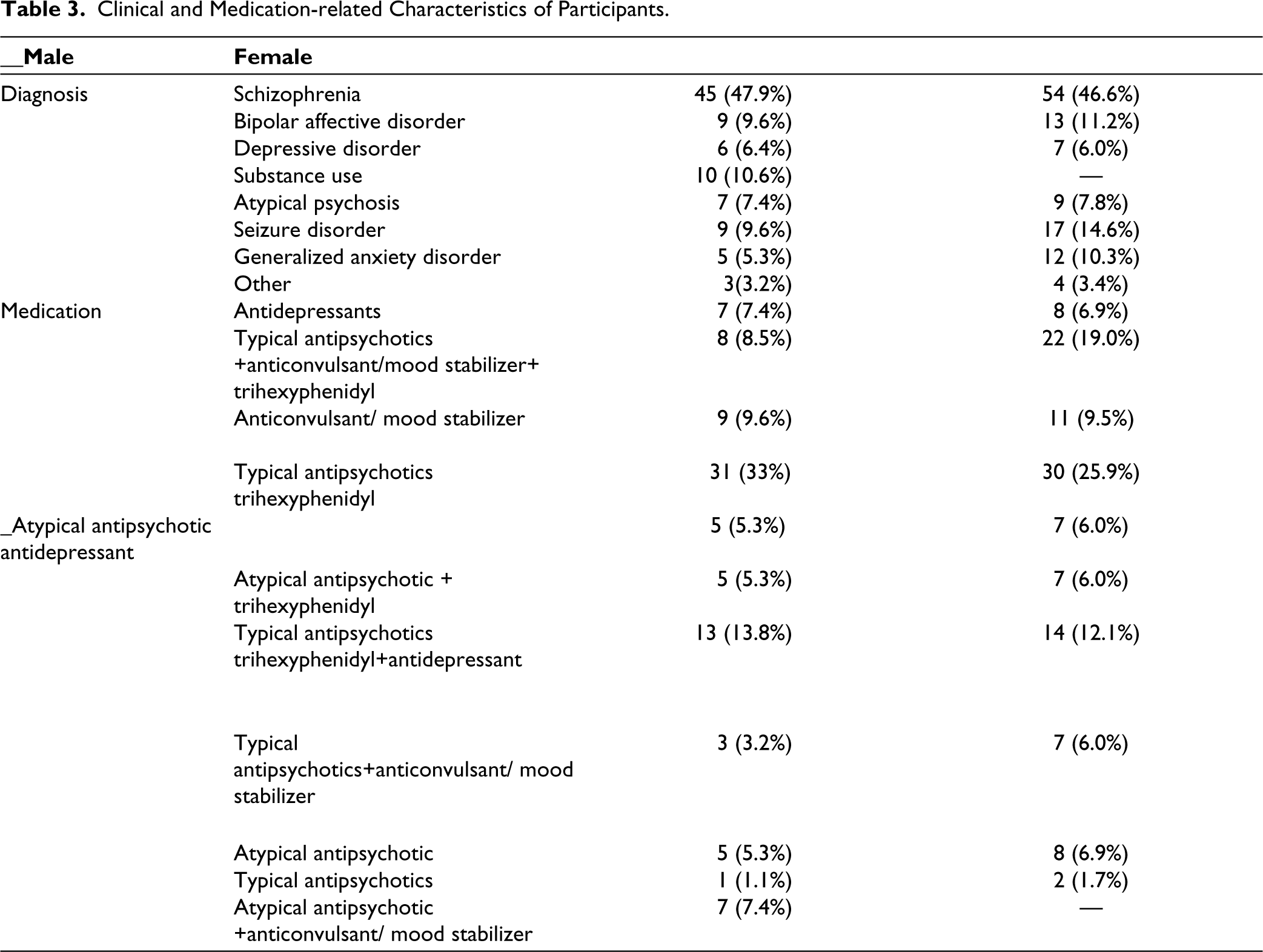
Table 4 shows that age, duration of illness, duration of treatment, and occupation were significantly associated with erectile dysfunction, intercourse dissatisfaction, orgasmic dysfunction, sexual desire dysfunction, and overall dissatisfaction in male patients but medicine compliance was associated with sexual desire dysfunction. Education, domicile, and socioeconomic status were not associated with any of the sexual dysfunction domains.
Correlation Between Specific Sexual Dysfunctions and Sociodemographic, Clinical, and Medication-related Variables in Male Participants.
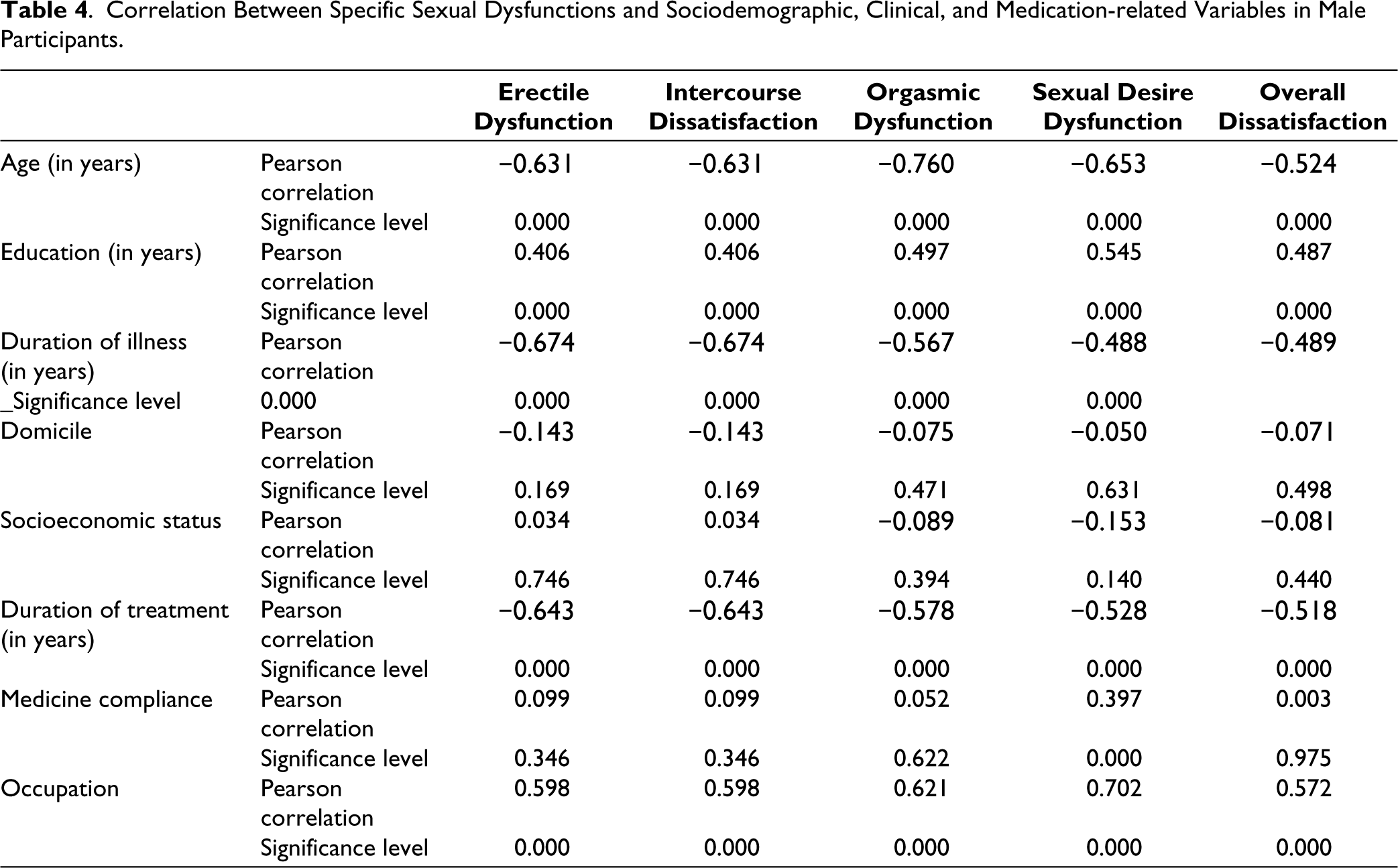
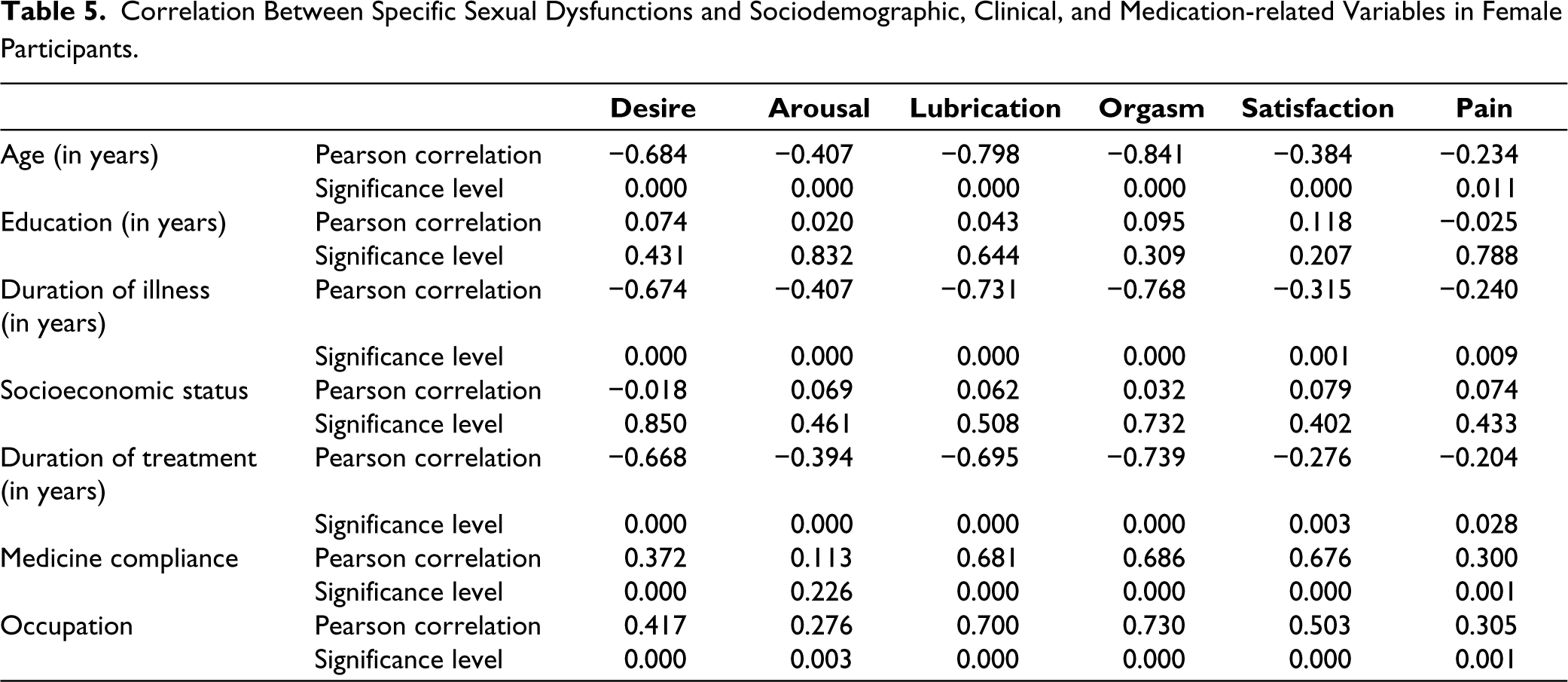
Table 5 shows that age, duration of illness, duration of treatment, and occupation were significantly associated with desire, arousal, lubrication, orgasm satisfaction, and pain in female patients. Medicine compliance was also associated with all dysfunction except arousal dysfunction. Education, domicile, and socioeconomic status were not associated with any of the sexual dysfunction domains.
Correlation Between Specific Sexual Dysfunctions and Sociodemographic, Clinical, and Medication-related Variables in Female Participants.
Discussion
This study examined the correlates of sexual dysfunction among male and female psychiatric outpatients receiving psychotropic medications at institute of mental health and hospital, Agra. This study sample consisted of 94 male and 116 female patients. Majority of both male (57.4%) and female (64.7%) participants were unemployed and diagnosed with schizophrenia. Schizophrenia is a chronic and debilitating disorder that impairs occupational and social functioning in most of the patients. The high unemployment ratio may be attributed to impaired occupational functioning.
About 76.6% male and 75.9% female participants used more than two psychotropic medications. These findings are similar to the findings of other studies. 38 Majority of both male patients (33%) and female patients (25.9%) were on typical antipsychotics and trihexyphenidyl. The combination of typical antipsychotics, trihexyphenidyl, and antidepressant was being given to 13.8% male patients and 12.1% female patients. Many studies have already reported the adverse effects of these medications via their mechanisms of action.39-42 The use of these combinations might be a factor in precipitating sexual dysfunction in patients. The mean age of the male participants was 34.95 years and female participants was 34.21 years. Similar findings have also been reported where the mean age was 34.7 years which is considered as the reproductive age group and patients are more concerned with sexual functioning. 38
Erectile dysfunction was found to be the most common sexual dysfunction in men (47.0%) receiving psychotropic medication. This was followed by sexual desire dysfunction (29.1%) and then orgasmic dysfunction (25.5%). This finding is similar to the results of some other studies.43,44 Lubrication disorder was seen in the majority of female patients (35.1%) followed by female sexual desire dysfunction (28.8%) and arousal dysfunction (18.5%). This study also found that men were more dissatisfied with their sexual functioning (22.8%) compared to women (11.3%) that is similar to other studies which reported that sexual dysfunction is more disturbing in men than in women taking psychotropic medications.33,43
Majority of participants (male = 59.6%) and (female = 64.7%) received typical antipsychotics and 76.6% male and 75.9% female participants used more than two psychotropic medications, especially conventional antipsychotic (antidopaminergic), trihexyphenidyl (anticholinergic), and antidepressant (serotonergic/ noradrenergic) combinations. Studies have found that libido is primarily regulated by dopamine, arousal by acetylcholine and nitric oxide, and orgasm by serotonin and noradrenaline. 24
Therefore, the mechanism of action of these psychotropic medications may be implicated as a cause of sexual dysfunction. A feeling of inadequacy is observed in men due to their inability to achieve a good penile erection for optimal sexual satisfaction. Stigma and spousal abandonment also increase the feeling of inadequacy. 45 Once patients recognize that their psychotropic medications produce one form of sexual dysfunction or the other, it often results in poor treatment adherence. 43 This study found that age is related to all forms of sexual dysfunction among both male and female patients. The natural process of aging increases sexual dysfunction, 46 but the use of psychotropic medication further increases the risk of developing sexual adverse effects through their mechanisms of action as reported by many studies.24,41,42
This study also reported that employment status was significantly associated with all the domains of sexual dysfunction in both male and female patients which is similar to the finding of a study. 44 Overall, employment status was found to be predictive of sexual dysfunction in male patients receiving psychotropic medication. Unemployment produces financial stress in both male and female patients which in turn negatively affects sexual functioning. Several studies have shown that unemployment was associated with low sexual desire and erectile dysfunction in the general population47,48 and mentally ill patients. 38
Duration of illness and duration of treatment are associated with all forms of sexual dysfunction in both male and female participants. Patients usually take regular maintenance doses for continuous illness and try to be in symptom-free condition. By the time they realize the negative impact of psychotropic medication and start to drop the medication, impairment in sexual dysfunction had already taken place. 38
This research showed no association between the clinical diagnoses of participants, domicile and education, and sexual dysfunction. Sexual functioning is a biological phenomenon that has a universal pattern of presentation across diagnosis, educational background, and domicile. Use of psychotropic medication probably causes decreased sexual performance and satisfaction.49,50
Psychotropic medication use was found to be associated with sexual dysfunction in male and female participants. In this study, 76.6% male and 75.9% female participants used more than two psychotropic medications. Studies have reported that typical antipsychotic use was associated with erectile dysfunction in males and orgasmic dysfunction in males and females, while antidepressant use was associated with orgasmic dysfunction in males and females.28,44
This study simply reported the status of various types of sexual dysfunction among male and female psychiatric patients receiving psychotropic medications. But the diagnosis of psychotropic drug-induced sexual dysfunction still needs further exploration
Conclusion
The use of psychotropic medication has adverse effects on sexual functioning of the psychiatric ill patients which associated with various demographic, illness-related, and medication-related variables.
Limitations
It was cross-sectional study which is only predictive but not sufficient to establish the causal relationship between sexual dysfunction and, psychotropic medications, sociodemographic, and clinical variables.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval and Informed Consent
The study was approved by the Institution Ethics Committee (IEC) of Institute of Mental Health and Hospital, Agra vide approval number: IEC/IMHH/N88/V1.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.