
Abstract
Objective
To investigate gender-specific relationships between self-reported sexual abuse, antisocial behaviour and substance use in a large community sample of adolescents.
Method
A cross-sectional study of students aged, on average, 13 (n = 2596), 14 (n = 2475) and 15 years (n = 2290), from 27 schools in South Australia with a questionnaire including sexual abuse, frequency and severity of substance use, depressive symptomatology (CES-D), family functioning (McMaster Family Assessment Device), and antisocial behaviour (an adapted 22-item Self-Report Delinquency Scale). Logistic regression analyses using HLM V5.05 with a population-average model were conducted.
Results
In the model considered, reported sexual abuse is significantly independently associated with antisocial behaviour, controlling for confounding factors of depressive symptomatology and family dysfunction, with increased risks of three- to eightfold for sexually abused boys, and two- to threefold for sexually abused girls, compared to nonabused. Increased risks of extreme substance use in sexually abused girls (age 13) and boys (ages 13–15) are more than fourfold, compared to nonabused. Age differences were not statistically significant.
Conclusion
Childhood sexual abuse is a risk factor for the development of antisocial behaviour and substance use in young adolescents. Clinicians should be aware of gender differences.
Adolescents with a history of childhood sexual abuse (CSA) face many problems in their psychosocial development [1]. They are at greater risk for major depression, anxiety, posttraumatic stress disorder [2], conduct disorder (CD), and substance use/dependence [3,4]. Childhood sexual abuse, mood disorders and suicidality in adolescents have been the subject of numerous investigations [5–7]. Relationships between CSA and antisocial and health-compromising behaviours have seldom been studied [8]. A recent metaanalysis of the effects of CSA [9], for instance, did not include antisocial behaviour, delinquency or substance abuse in six outcomes investigated. Yet, increasing rates of psychosocial disorders in youth [10], disruptive behaviours, delinquency, and substance abuse are escalating public health problems, resulting in great costs to individuals and communities. Although aetiology is complex and exact knowledge of progression during adolescence and prognosis into adulthood remains elusive, many risk factors for antisocial behaviour have been consistently identified [11–14]. Childhood sexual abuse is one such factor. Adverse family factors and negative parenting style frequently coexist [12,15], yet after controlling for significant sociodemographic, family and parental confounding factors [3], and lack of family connectedness [16], CSA is still independently and significantly associated with increased risk for CD [3] and other health compromising behaviours such as substance abuse [16]. Further, a history of CSA is common in delinquent populations in custody [17,18], and longitudinal studies [19] support strong relationships between family problems, physical and sexual abuse, adolescent delinquency and drug abuse.
Studies of antisocial behaviour (not involving CSA) in both clinical and epidemiological samples of adolescents have found strong positive associations between substance use disorders (SUD) and both externalizing behaviours [20] and internalizing behaviours [21]. It is not yet resolved whether SUD leads to antisocial behaviour, or early antisocial behaviour leads to later SUD, or whether SUD and antisocial behaviour are both manifestations of other underlying factors or social influences (e.g. peer affiliations). Developmental models of multiproblem youth [22] and longitudinal studies [19] recommend early intervention before drug use and delinquent careers become established. Further, ages 11 and 14 years have been identified as turning points at which delinquent attitudes and behaviour escalate [23], and early onset of substance use before 14 years is associated with continued impairment in behavioural and emotional functioning in later adolescence [24].
Responses to CSA may be influenced by gender [25], age and developmental stage [2]. For example, Neumark et al. [16] found CSA strongly associated with substance use only for young adolescents (grade 6 compared to grades 9 and 12). The weak initial association of CSA with delinquency at grade 6 increased with age for boys and decreased with age for girls. These results suggest interventions should be both age- and gender-related [26]. This is of particular importance in adolescence, as early onset CD and substance use lead to greater dysfunction in later years [20].
The current study, part of a longitudinal investigation into risk factors for adolescent suicidality, investigates relationships between CSA, antisocial behaviour and substance use in a large community sample of adolescents. Cross-sectional analyses examine relationships, possibly gender-specific, between self-reported CSA, antisocial behaviour and substance use in the same group of adolescents, on three occasions, when aged approximately 13, 14 and 15 years. Family functioning, parenting style, depressive symptomatology, and sociodemographic variables are investigated as possible confounding factors.
Method
The South Australian Early Detection of Emotional Disorders Program (EDED) was approved by the Department of Education and Children's Services, the Catholic Education Office, the Independent Schools Board and Flinders Medical Centre Ethics Committee on Clinical Investigation. The central focus was early detection of suicidal behaviours, and risk/protective factors implicated in later suicide. Research design was a prospective time series study, in which the sample was surveyed yearly on three occasions. Participants at time one (T1) were in year 8 high school, averaged 13 years; at time two (T2) 14 years, and time three (T3) 15 years. Data on antisocial behaviour, substance use and CSA used in the present study, previously unreported, is drawn from T1, T2 and T3.
Participants
High school students from 17 public and 10 private, rural and suburban schools in lower to upper middle socio-economic areas of South Australia participated in the study. Following parental assent, 2596 actively consenting students were surveyed at T1, 2475 at T2 and 2290 at T3, an overall participation rate of approximately 85%. Students completed the questionnaire under the supervision of teachers, placing their responses in a sealed container. A group debriefing session followed, and a school counsellor was available for any student showing distress.
Measures
Items of interest reported here form part of a larger comprehensive questionnaire [27].
Occurrence of CSA was assessed simply: ‘Have you ever been sexually abused' with a ‘yes/no’ response. Second: ‘If yes, then by whom?’ has a choice of responses ‘a friend, a family member, someone else known to me, a stranger’. Third: ‘How distressed do you feel about this now?’ has response choices on a 7-point Likert scale of 0 (not at all distressed) to 6 (extremely distressed).
Antisocial behaviour (ASB) was assessed with an adaptation of the Self-Report Delinquency Scale [28]. Students responded with ‘yes’ (score 1) or ‘no’ (score 0) to statements such as 7 have stolen out of a little shop’. Four additional items were included to cover behaviours in DSM-IV diagnostic guidelines for CD. These were: 7 have set fire to things in public places just for fun'; ‘I have graffitied (tagged) things in public places'; 7 have deliberately tried to physically hurt someone'; 7 have deliberately tried to attack someone in a sexual way‘. For this analysis, two items in the original scale regarding alcohol and illegal drug use were disregarded, to avoid overlap with the current study's more detailed assessment of substance use. Reliability for the adapted 22-item scale was good (α = 0.87). Principal components factor extraction with varimax rotation resulted in three factors with eigenvalues greater than 1 (6.29, 1.46, 1.16) accounting for 40.4% of total variance. Total scores were calculated and recoded to new 2-category variables based on two cut-offs calculated from the T1 mean (2.53) plus one standard deviation (3.41), and T1 mean +2 SD. Thus, total scores equalling 6 were coded ‘not antisocial'; scores equalling 7 or more were coded as ‘serious'; and scores equalling 10 or more were coded as ‘extreme’. These points were chosen to set baseline measures at T1 against which future antisocial behaviour at T2 and T3 could be compared.
Substance use was assessed by asking: ‘Which of the following drugs have you used in the last year? alcohol; tobacco; marijuana, acid or LSD; sniffed glue, petrol, or solvents; injected illegal drugs (heroin, speed); oral stimulants (speed, crack, or ecstasy), magic mushrooms’. Respondents rated frequency of use for each on a 5-point scale: 0 (never); 1 (less than once per month); 2 (one to three times a month); 3 (once a week); or 4 (more than once a week). Total scores (0–32) were recoded to new 2-category variables based on cut-offs of the T1 mean (1.82) plus 1 SD (2.87), and T1 mean +2 SD. Thus, total scores ≤5 were coded ‘serious'; and scores ≥ 8 were coded ‘extreme’. Cut-offs were chosen to set baseline measures at T1 against which substance use at T2 and T3 could be compared. Reliability for the summed items was good: T1 (α = 0.82); T2 (α = 0.88); and T3 (α = 0.85). Finally, if alcohol or marijuana were used in the month prior, respondents were asked to rate ‘how drunk' or ‘how stoned' on a scale of 0 (not at all) to 6 (extremely).
Socio-demographic information collected included school, gender, age, country of birth, main language spoken at home, Aboriginal or Torres Strait Islands origin.
Depressive symptomatology was measured with the Centre for Epidemiological Studies Depression Scale (CES-D), a self-report 20-item instrument recommended for use with community samples of adults [29] and adolescents [30]. Respondents rate frequency of depressive symptoms in the past week on a 4-point scale ranging 0–3.
Family functioning was assessed using the McMaster Family Assessment Device – General Functioning Subscale (FAD-GF) [31]. Scores for the 12 items range 1–4; higher scores indicate family pathology.
Parenting style and quality of the relationship between parents and adolescents were assessed with the Influential Relationships Questionnaire, a 37-item instrument consisting of care, protection and criticism subscales [32].
Data analysis
Data analysis was undertaken with SPSS V11 and HLM V5.05 [33]. The latter was chosen to take into account the effect of the 2-stage survey design [34] of the EDED Program, where schools were selected first, then students from within those schools. Logistic regression analyses were performed to investigate strength of relationships between CSA (the independent variable) and self-reported antisocial behaviour or substance use (as dichotomous dependent variables), controlling for potential confounding factors. Preliminary analyses indicated that the extent of school-based clustering in the EDED dataset for the dependent variables under consideration was minor, and the HLM results are very similar to those obtained from standard logistic regression procedures (using SPSS). For statistical accuracy, however, the HLM results are presented. Two–way interactions between gender and CSA were significant, thus separate analyses were conducted for boys and girls. The HLM results from the population average model with robust standard errors are reported, along with 95% confidence intervals.
Sample attrition
An attrition analysis of the sample was conducted, as there were some difficulties tracking participants from year to year, and higher than expected numbers appeared to leave or join the study between T1–T2 and T2–T3. Respondents reporting CSA at T1 who dropped out (n = 40) were not significantly different from those who continued participation (n = 59) at T2, on measures of ‘distress following CSA’, depressive symptomatology or family functioning. Small but significant differences were found for serious drug use (χ21 = 4.165, p < 0.05; 43% dropouts vs 23% continuers); and serious ASB (χ21 = 9.385, p < 0.01; 49% dropouts vs 19% continuers). Respondents reporting CSA at T2 who dropped out (n = 47), or continued participation (n = 40) at T3, were significantly different on measures of ‘distress following CSA’ (χ22 = 6.401, p<0.05; 49% dropouts vs 26% continuers); serious drug use (χ2, = 7.583, p < 0.01; 70% dropouts vs 40% continuers); and serious ASB (x2, = 10.282, p< 0.001; 62% dropouts vs 27% continuers). New entrants to the study at T3 reporting CSA (n = 25), however, were not significantly different from those already present. Thus samples at T2 and T3 may under-represent adolescents reporting sexual abuse, serious drug use and antisocial behaviour.
Results
Table 1 shows the prevalence of ‘serious’ and ‘extreme’ antisocial behaviour and substance use. In boys, antisocial behaviour increases sharply from T1 to T2, then stabilizes at T3 with a small decrease in those classified serious and a small increase in extreme. In girls, antisocial behaviour also increases sharply at T2, followed at T3 by a small increase in serious and a small decrease in extreme. Overall, boys categorized as serious and extreme outnumber girls by two- to threefold.
Prevalence of CSA, antisocial behaviour and substance use in boys and girls at mean age 13 (T1), 14 (T2) and 15 (T3) years
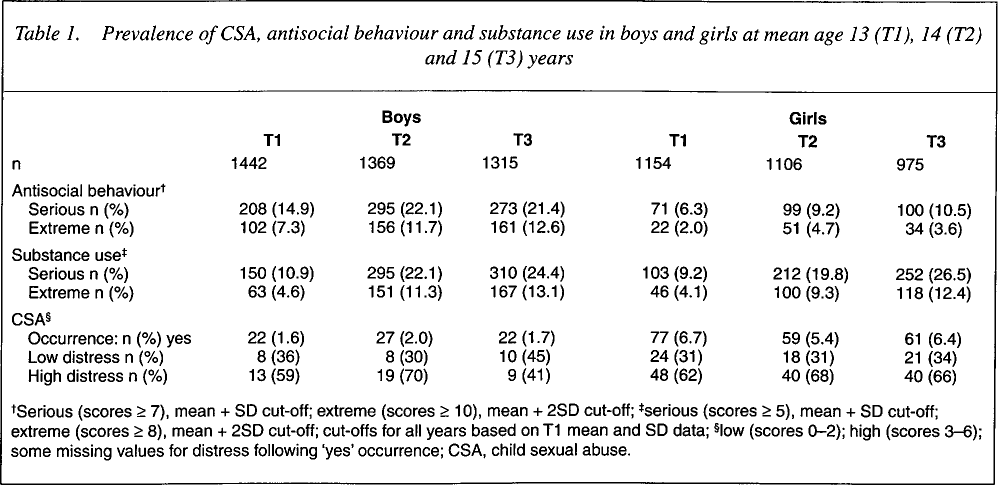
Serious (scores ≥ 7), mean + SD cut-off; extreme (scores ≥ 10), mean + 2SD cut-off;
serious (scores > 5), mean + SD cut-off; extreme (scores ≥ 8), mean + 2SD cut-off; cut-offs for all years based on T1 mean and SD data;
low (scores 0–2); high (scores 3–6); some missing values for distress following ‘yes’ occurrence; CSA, child sexual abuse.
In contrast, percentages of boys and girls classified with serious and extreme substance use are similar and increase with age.
More girls report experience of CSA than boys, with percentages remaining steady over T1, T2 and T3. The majority also report high levels of current distress following CSA.
Differences between sexually abused and nonabused adolescents in patterns of substance use and antisocial behaviour are significant. (See Table 2)
Frequency and severity of substance use and antisocial behaviour among sexually abused and non-abused adolescents at mean age 13 (T1), 14 (T2) and 15 (T3) years
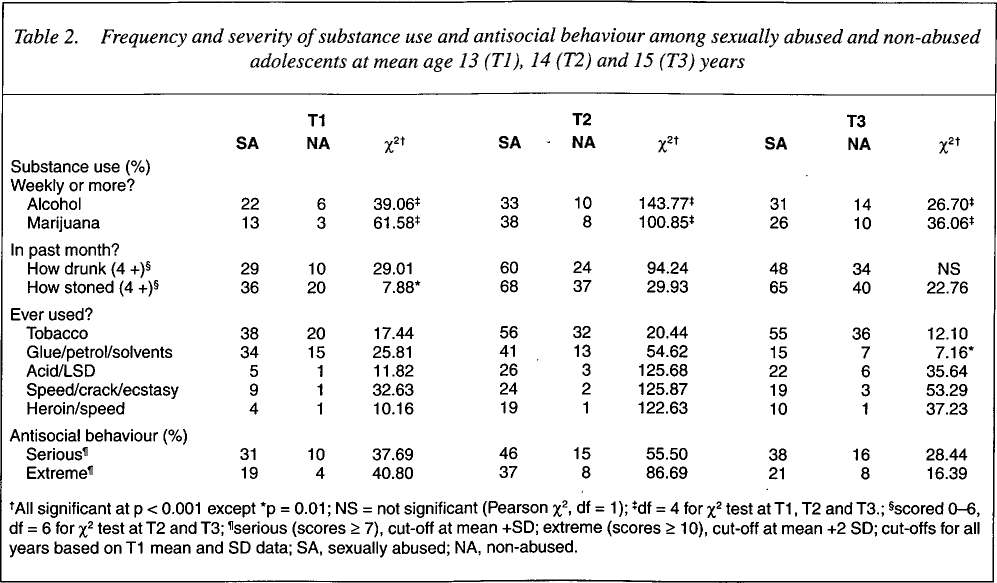
AII significant at p < 0.001 except
p = 0.01; NS = not significant (Pearson χ2, df = 1);
df = 4 for χ 2 test at T1, T2 and T3.;
scored 0–6, df = 6 for χ2 test at T2 and T3;
serious (scores ≥ 7), cut-off at mean +SD; extreme (scores ≥ 10), cut-off at mean +2 SD; cut-offs for all years based on T1 mean and SD data; SA, sexually abused; NA, non-abused.
More sexually abused adolescents use alcohol and marijuana, report higher scores on ‘how drunk’ and ‘how stoned’, and use other illegal/harmful drugs such as opiates and stimulants, than nonabused adolescents. Sexually abused adolescents are also significantly more likely to be classified with serious and extreme ASB.
Cross-sectional logistic regression models and adjustment for confounding factors
Separate logistic regression analyses were performed to assess the increased risk (odds ratio) of self-report serious and extreme antisocial behaviour and substance use (dichotomous dependent outcome variables) in sexually abused compared to nonabused individuals. To investigate the unique association of CSA with antisocial behaviour and substance use, significant confounding factors were controlled for by inclusion into the regression models as covariates. Depressive symptomatology and family functioning (continuous variables) made significant contributions to regression models for antisocial behaviour and substance use in boys and girls at all ages. Further adjustment by forward stepwise conditional (p < 0.05) inclusion of parenting style variables, in few instances, resulted in reduction of the Wald statistic for family functioning, and insubstantial changes in the association of CSA with outcome. Thus parenting style variables were not included in the final regression models.
Few adolescents were of ‘Aboriginal and Torres Strait Islands origin’ (T1, n = 25 [1.0%]; T2, n = 32 [1.3%]; T3, n = 27 [1.2%]). Included as a covariate in preliminary regression models, it contributed significantly (in boys only) to serious antisocial behaviour at T1 (OR = 6.4, 95% CI = 1.6–26.5, p<0.05); T2 (OR = 5.6, CI = 1.9–16.4, p<0.01) and T3 (OR = 3.2, CI= 1.0–10.1, p<0.05), and to serious substance use at T2 (OR = 6.2, CI = 2.1–18.5, p <0.05). However, concurrent reduction in the unique association by CSA was very small due to the small numbers involved, thus the ‘origin’ variable was not included in final analyses.
Final HLM models – antisocial behaviour
Results from population-average models for antisocial behaviour are presented in Table 3. For boys, unadjusted ORs for CSA onto serious antisocial behaviour are high at T1, T2 and T3 (6- to 15-fold). After adjustment for significant confounding factors of depressive symptomatology and family dysfunction, the association of CSA with both serious and extreme antisocial behaviour remains strong (3- to 8-fold).
Odds ratios (95% CI) for serious and extreme antisocial behaviour associated with childhood sexual abuse, unadjusted and adjusted for family functioning and depressive symptomatology at mean age 13 (T1), 14 (T2) and 15 (T3) years
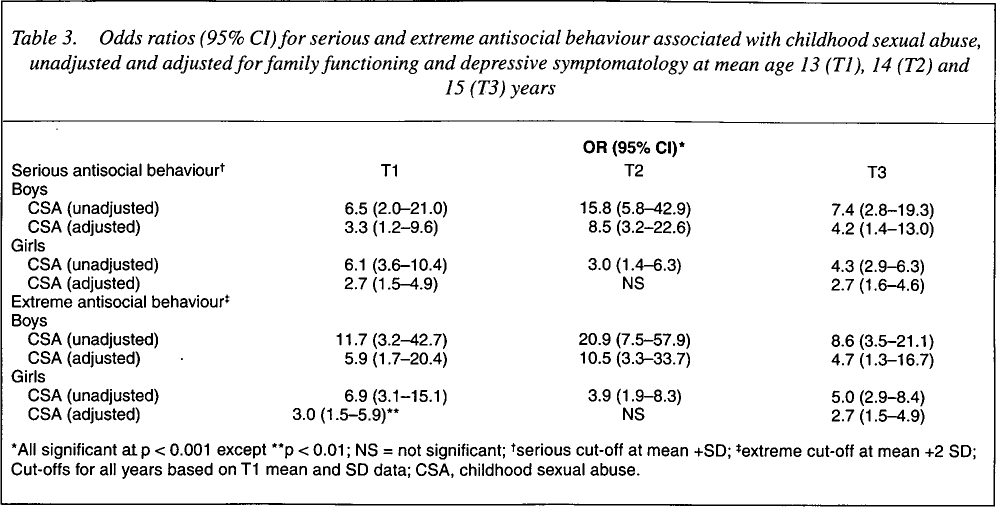
AII significant at p < 0.001 except
p < 0.01; NS = not significant;
serious cut-off at mean +SD;
extreme cut-off at mean +2 SD; Cut-offs for all years based on T1 mean and SD data; CSA, childhood sexual abuse.
In girls, the association of reported CSA with both serious and extreme antisocial behaviour is less strong than in boys, at all times with unadjusted ORs ranging from three- to sixfold. After adjustment for family dysfunction and depressive symptomatology, the independent association of CSA with serious antisocial behaviour is approximately two- to threefold at T1 and T3, but not significant at T2, in contrast to the strong association at T2 in boys.
Substance use
Results from population average models for substance use are presented in Table 4.
Odds ratio (95% CI) for serious and extreme substance use associated with childhood sexual abuse, unadjusted, and adjusted for family functioning and depressive symptomatology at mean age 13 (T1), 14 (T2), and 15 (T3) years
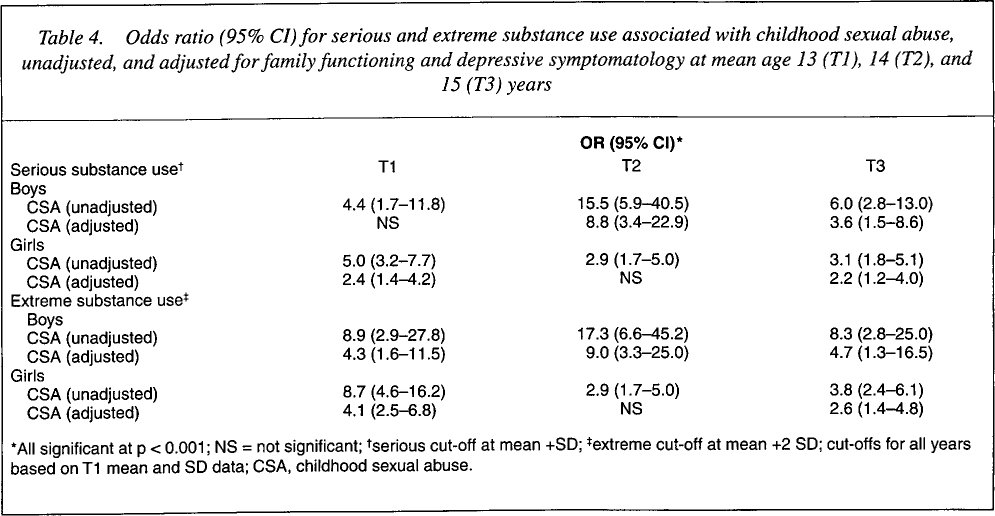
AII significant at p < 0.001; NS = not significant;
serious cut-off at mean +SD;
extreme cut-off at mean +2 SD; cut-offs for all years based on T1 mean and SD data; CSA, childhood sexual abuse.
For boys, unadjusted ORs for CSA onto serious substance use are high, ranging four- to fifteenfold over the three time points. After adjustment for family dysfunction and depressive symptomatology, CSA is not significant at T1. At T2 and T3, ORs remain high (more than 8-fold and 3-fold, respectively) and significant (p<0.001). For extreme substance use, adjusted ORs are high (4–9-fold) and significant (p < 0.001).
In girls, unadjusted ORs for CSA onto both serious and extreme substance use are high at T1, T2 and T3. After adjustment for family dysfunction and depressive symptomatology the association of CSA with substance use is reduced though still significant at both T1 and T3 (4- to 2-fold).
Discussion
The findings of this cross-sectional study of a large normal sample of adolescents indicate that reported sexual abuse is significantly and independently associated with antisocial behaviour and substance use. ‘Serious’ antisocial behaviour, as classified in this study, involves self-report of seven or more activities (prerequisites for a DSM-IV diagnosis of conduct disorder requires only three). ‘Extreme’ behaviour comprises 10 or more. After controlling for depressive symptomatology and family functioning, young sexually abused adolescents (13 years) are at greatly increased risk of serious and extreme antisocial behaviour, compared to nonabused. For older boys the association between CSA and antisocial behaviour remains consistently strong, with increased risks (adjusted) of eight- to tenfold at age 14 years and fourfold at 15 years. Apparent differences between age groups, however, are not statistically significant, in part due to small sample sizes.
In girls, the association between CSA and antisocial behaviour is in some agreement with Neumark et al. [16] and, relative to boys, the unique contribution by CSA is smaller after adjustment for family factors and depressive symptomatology. Our results support existing evidence that girls respond to CSA with fewer externalizing behaviours and more internalizing coping strategies and symptoms [12].
In contrast to antisocial behaviour, the pattern of substance use by boys and girls is similar, with increasing usage reported with increasing age. Serious substance use, as classified in this study, comprises very frequent use of two or more drugs, or greater variety of illegal, harmful or addictive drugs. In boys, adjusted associations of CSA with serious substance use are not significant at 13 years, but range from eight-fold to three-fold at 14–15 years. For extreme substance use, the increased risk is more than fourfold at all ages. For sexually abused girls, increased risk of serious and extreme substance use is two- to fourfold at 13 years, and not significant at 14 years, in some agreement with other studies [4,16] which found stronger associations between reported abuse history and alcohol use at younger ages.
However, although depressive symptomatology and family functioning were controlled for, other confounding factors not present in the model may account for the ‘independent’ association of CSA with antisocial behaviour and substance use. Further, odds ratios presented are an estimate of increased risk that must be appreciated in conjunction with the wide 95% CI.
Limitations include the three-item assessment of sexual abuse. Questions were restricted by the need to gain ethical, parental and educational approval, a constraint noted by others investigating large normal adolescent populations [8]. However, although the exact nature and extent of abuse are not explored with direct questioning, an item assessing severity indirectly, in terms of ‘distress’ following abuse is included. In previous work [35] a graded relationship between ‘low’ and ‘high’ distress following abuse, and suicidality, was found. However, in the present study, use of a categorical distress variable in regression analyses, already split by gender, would have further reduced sample numbers and statistical precision, thus self-reported abuse (yes/no) alone was chosen as the independent variable.
Rates of reported CSA are low, probably underestimating the true prevalence in the population. Fergusson et al. noted the greater likelihood of false-negative reporting of CSA compared to false-positive by young adults [36]. Thus, although reported rates are low, confidence in the perception of the abuse experience and veracity of responses by these adolescents is increased. Indeed, the self-report questionnaire and normal population sample are strengths of the study. Further, our analysis takes account of the clustered sampling (by schools), leading to best practice estimation of standard errors.
It seems clear that sexual abuse, most likely prior to our study, after taking into account depressive symptomatology and family discord, plays a unique role in increasing risks for both antisocial behaviour and substance use. Possible clinical implications are that early detection of sexual abuse, and adequate clinical work to reduce impact, may reduce long-term development of both antisocial behaviour and substance use. Alternatively, clinicians faced with even the most extreme cases of antisocial behaviour and substance use need to be aware that both may have their beginnings in sexual abuse; targeted programs should include relevant history and sensitive exploratory therapy as part of behaviourally-oriented management.
Footnotes
Acknowledgement
The original research was financially supported by the South Australian Health Commission.