
Abstract
Sexual pleasure holds significant importance for individuals, relationships and societies due to its physiological, psychological and social dimensions. It is an individual experience that can signify or represent one or many aspects of personal importance in one’s life. Humans have always sought various means to enhance sexual pleasure. These may be physical, psychological or pharmacological. Of these, the substances with positive pharmacodynamic effects on the nervous system and the reproductive system are of particular importance. Such substances are called as aphrodisiacs. In the last few decades, recreational drugs have been abused quite a lot as aphrodisiacs, especially by the younger population. Recreational drug use has the potential to impact various aspects of sexual experience, from enhancing desire and pleasure to compromising sexual function and overall well-being. This is why the relationship between recreational drugs and sexual health is a complex, multifaceted topic and can have significant implications for both physical and mental well-being. It is important to approach this topic with care and awareness with respect to its potential risks and consequences. This review article delves into the intricate interplay between substance abuse and sexual health, shedding light on both the positive and negative dimensions of this connection.
Introduction
Sexual pleasure holds significant importance for individuals, relationships and societies due to its physiological, psychological and social dimensions. It is an individual experience that can signify or represent one or many aspects of personal importance in one’s life. For some, sexual pleasure may signify physical well-being due to the release of happy hormones like endorphins, oxytocin and dopamine, and for others, it may represent an emotional connection that enhances trust and care towards a partner. For some, it may signify satisfaction in a relationship, whereas for others it may be a means of stress reduction, self-exploration or open communication. Apart from this, for couples trying to conceive, sexual pleasure is essential to encourage regular sexual activity, which can improve the chances of conception.
For these reasons and many more, humans have always sought various means to enhance sexual pleasure. These may be physical, psychological or pharmacological. Of these, the substances with positive pharmacodynamic effects on the nervous system and the reproductive system are of particular importance. Such substances are called aphrodisiacs. An aphrodisiac is defined as any food or drug that arouses the sexual instinct, induces venereal desire and increases pleasure and performance. 1 This word is derived from Aphrodite, the Greek Goddess of love.
In the last few decades, recreational drugs have been abused quite a lot as aphrodisiacs, especially by the younger population.2,3 Also, people using recreational drugs tend to engage in risky sexual behaviour more frequently.4-6 Recreational drug use has the potential to impact various aspects of sexual experience, from enhancing desire and pleasure to compromising sexual function and overall well-being. This is why the relationship between recreational drugs and sexual health is a complex, multifaceted topic and can have significant implications for both physical and mental well-being. It is important to approach this topic with care and awareness with respect to its potential risks and consequences.
Methods
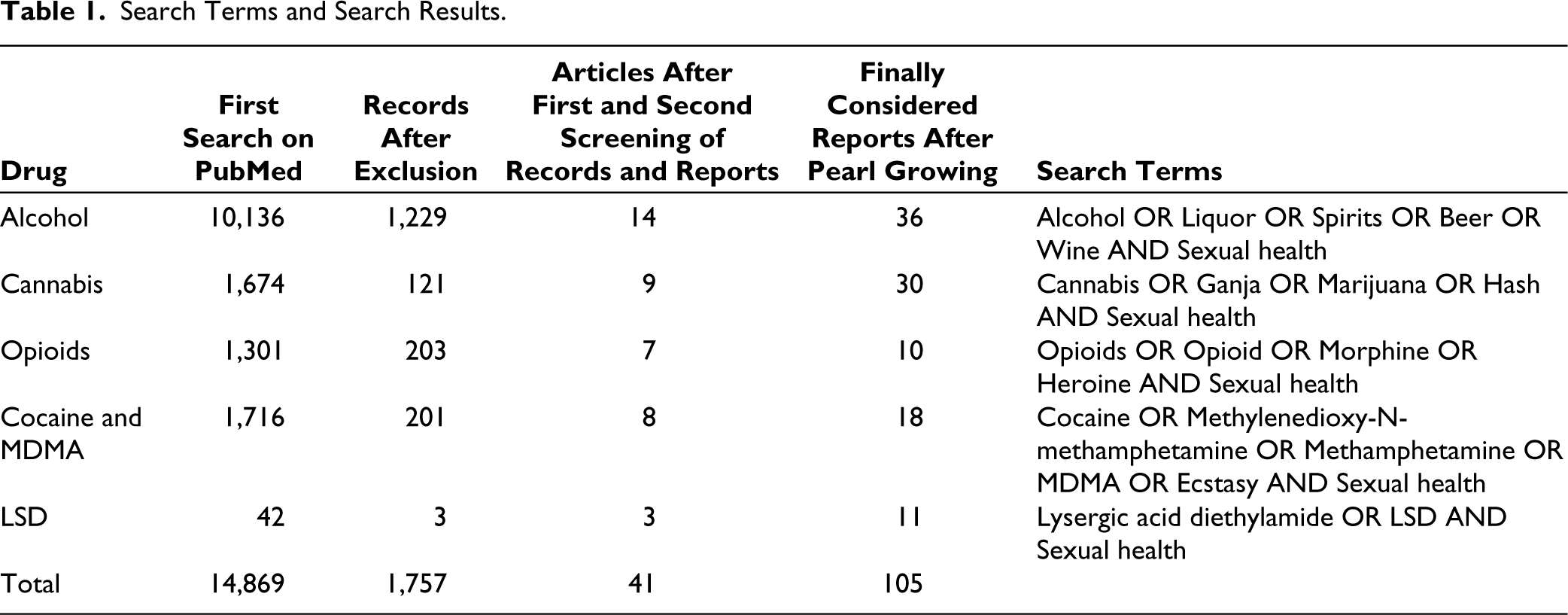
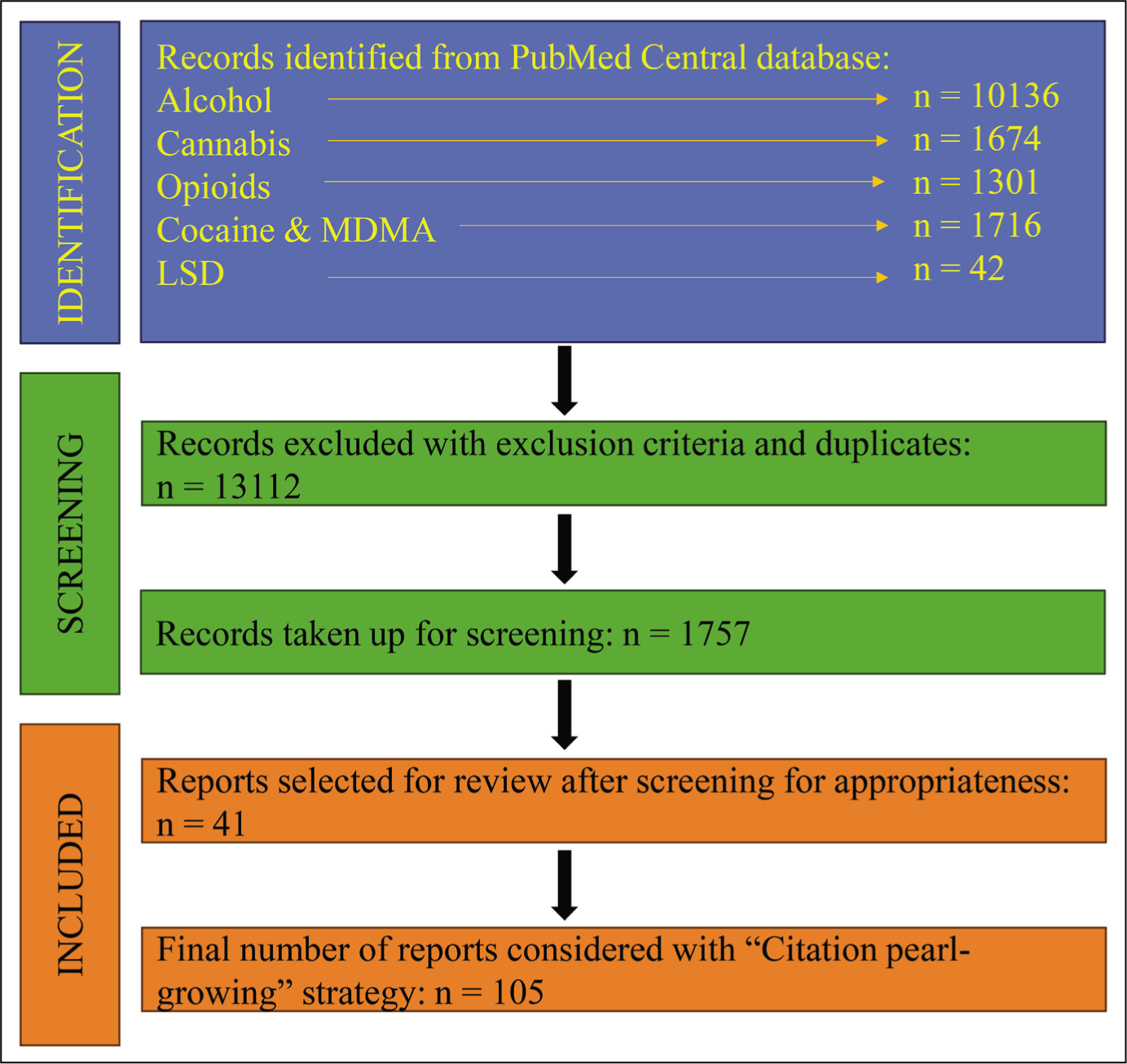
The electronic database of PubMed was searched for articles for the purpose of writing this review. Primary research articles and other review articles published in the English language were selected for review. Due consideration was given to assigning credit to appropriate authors who conducted the primary research for their results while reviewing review articles. Editorials, news articles, letters to editors, retracted articles, personal narratives, patient education handouts, legislation or legal articles, articles on conferences/seminars/webinars, historical articles, government publications and duplicate reports/articles were not considered for the review. There was no age bracket or specific publication period considered for searching the literature. The primary search on PubMed yielded 14,869 results. The various search terms used for each recreational drug along with the respective search results have been provided in Table 1. Out of these, 13,112 results or records were excluded based on exclusion criteria. The remaining 1,757 records were taken up for further review. The primary and corresponding authors separately screened 1,757 records by title and abstract for appropriateness, and selected records were considered for further review. Three separate reviewers then screened the selected records for appropriateness by title and abstract, as well as full text, and a total of 41 articles or reports were selected. Disagreements among reviewers were resolved by consensus. Further search strategy was carried out using the ‘Citation pearl-growing’ strategy, where the literature and citations provided in 41 selected reports were used to screen and search for further articles by the primary and corresponding authors, separately. Finally, a total of 105 articles or reports were considered for writing this review. Drug-wise distribution of the same has been provided in Table 1, and a flow chart of the above search strategy has been provided in Figure 1.
Search Terms and Search Results.
Study Flow Diagram of Literature Search.
Discussion
The impact of recreational drugs on sexual health can vary depending on the specific drug, the dosage, the individual’s physiological and psychological characteristics and the context in which the drugs are used. From altered perceptions and heightened sensations to impaired cognitive, physical and sexual functions, recreational drugs can exert a range of effects that intertwine with intimate encounters. This review article delves into the intricate interplay between substance abuse and sexual health, shedding light on both the positive and negative dimensions of this connection.
Recreational Drugs
There are numerous illicit recreational drugs available in the grey market today. Of these, the most commonly abused ones are alcohol (not illicit), cocaine (tropane alkaloid), heroin and morphine (opioids), ganja/cannabis (tetrahydrocannabinol)), ecstasy (3,4-methylenedioxymethamphetamine [MDMA]) and lysergic acid diethylamide/acid (LSD). Amongst these, alcohol is the most commonly abused substance followed by cannabis, which is the most commonly abused illicit substance in India. 3
Effects of Recreational Drugs on Sexual Health
Alcohol
Alcohol has been an integral part of human culture and social interactions for millennia. Throughout history, alcohol has played a role in religious ceremonies, celebrations, social gatherings and social interactions on a day-to-day basis. 7 It is a psychoactive substance that is commonly consumed in various forms, such as beer, wine and spirits. Its effects on individuals, families and communities are complex and multifaceted, influencing social dynamics, relationships and health (physical, mental and sexual) in both positive and negative ways.
The effects of alcohol on sexual health mainly depend on the quantity and duration of alcohol consumption. 8 Although low to moderate amounts of alcohol have been shown to increase sexual libido in both males and females, chronic and high consumption is associated with decreased desire, arousal, delayed orgasms in both sexes and erectile dysfunction (ED) in men.8-11 Nevertheless, even a moderate quantity of alcohol can lead to disinhibition, which leads to risky sexual practices and the spread of sexually transmitted diseases. Also, it can be a cause of sexual victimization.12,13
Acute Effects of Alcohol: The Disinhibition Hypothesis
The disinhibition hypothesis states that all the impulses that can affect behaviour are controlled by inhibiting forces.14-16 It is proposed that alcohol weakens these inhibiting forces, thus making people more responsive to these impulses, or in other words impulsive! The concept of ‘disinhibition’ is defined as ‘loss of self-control upon overindulgence in alcohol or while under influence of drugs’. 17 Alcohol (ethanol) is primarily a central nervous system depressant. 18 It has been observed that the electroencephalogram (EEG) of people who have consumed alcohol shows lower amplitude waves and action potential when measured also has a shorter duration.19-22 Alcohol depresses various parts of the brain in a dose-dependent manner. The cortical nerve fibres seem to be most sensitive and affected first. The cortex normally controls impulses from other regions of the brain, such as the limbic system. 23 At low to moderate doses, alcohol has an inhibitory effect on nervous activity in the cerebral cortex, which results in deteriorated impulse control and decreased apprehension when drunk. Thus, the disinhibition or impulsiveness caused is responsible for risky sexual behaviour in alcoholics. Numerous studies carried out on alcohol consumption and risky sexual behaviour have supported the hypothesis that rising alcohol intoxication increases the likelihood of intercourse without barrier contraception (condoms) with non-steady partners.24-29 Furthermore, disinhibited aggression in males has also been an important cofactor for sexual victimization, especially in females.30,31 Low amount of alcohol has also been linked with increased sexual desire, arousal and pleasure in both men and women.32,33 Low amounts of blood alcohol have been shown to increase blood testosterone levels in males as well as females. 31
But as the quantity of consumption increases, the risk of unprotected sexual encounters and victimization also increases, as acute intoxication with alcohol leads to impairment of judgement and retrograde amnesia. Toxic or high alcohol levels also lead to acute episodic erectile failures that can have a great psychological impact on males. 34 Such episodes can create doubts in the minds of males regarding their own virility and sexual potency, as ED, which was physiological in nature to begin with, can now have a psychogenic component to it. 35 This can adversely affect self-confidence as well as personal relationships, thereby hampering mental as well as sexual health. Research on alcohol’s effect on orgasm is limited. In males, alcohol increases the latency to orgasm, and this latency has a linear relationship with blood alcohol levels. 36 Whereas in females, it was found that alcohol was related to inconsistent, fewer and delayed orgasms. 37
Chronic Alcoholism and Its Effects on Sexual Health
Chronic alcoholism can have significant negative effects on sexual health, apart from general health, in both men and women.
In men, the most common sexual dysfunction associated with chronic alcoholism is ED, followed by decreased libido. 38 There are several plausible explanations for the same. Chronic alcoholism leads to alcoholic neuropathy or alcohol-induced damage to nerves. Although the exact mechanisms involved in the genesis of alcoholic neuropathy are unknown, several explanations have been proposed, some of which are as follows. Nerves are damaged by the direct toxic effects of alcohol. 39 Apart from this, chronic alcoholics invariably suffer from vitamin deficiencies, especially thiamine (Vit-B1) deficiency. Thiamine plays an unidentified role in propagating nerve impulses and also takes part in myelin sheath maintenance. 40 Also, the oxidation of alcohol, which is a part of alcohol metabolism, generates free oxygen radicals. Free oxygen radicals directly damage the myelin sheet of nerves. Also, the generation of free oxygen radicals causes an imbalance between oxidants and anti-oxidants, thus creating oxidative stress. Neuropathy-induced ED is a common finding amongst chronic alcoholics, similar to ED found in diabetics due to diabetic neuropathy. Also, reduced levels of nitric oxide (a potent anti-oxidant and vasodilator), due to oxidative stress, cause insufficient vasodilation in the penile vessels, leading to ED.
Chronic alcoholism also depresses the hypothalamic–pituitary–gonadal (HPG) axis. This causes the release of reduced levels of gonadotropins and testosterone and leads to decreased libido, testicular atrophy and inhibition of spermatogenesis.41,42 Additionally, the oxidative stress present also directly damages the sperms and testicular cells, resulting in low sperm count and unhealthy sperms. 38 In females, the depression of the hypothalamic–pituitary–adrenal axis causes decreased levels of follicle-stimulating hormone (FSH) and luteinizing hormone (LH). This leads to a wide variety of problems that can range from decreased libido to menstrual irregularities, vaginal dryness, dyspareunia, and so on. 38 Chronic alcoholism is also associated with orgasmic dysfunction in both males and females, which can manifest as pre-mature or delayed ejaculation in males and difficulty in achieving orgasms in females. 34
Cannabis
Cannabis, also known as marijuana or ganja, can have various effects on sexual health, and these effects can vary from person to person. Research on this topic is ongoing, and while some studies suggest potential benefits in certain cases, others point to potential drawbacks. Individual responses to marijuana differ based on factors like dosage, frequency of use and the strain of cannabis involved. Cannabis contains about 60 pharmacologically active cannabinoid compounds. 43 The most studied and active among them is delta-9-tetrahydrocannabinol (THC). It acts on G-protein-coupled cannabinoid receptors, CB1 and CB2. While CB1 is expressed in the brain and responsible for its mental effects and addiction-forming capability, CB2 is expressed in peripheral tissues. In the brain, CB1 is present in the basal ganglia, hippocampus, cerebellum and association cortices. 44 When the CB1 receptor in the brain is stimulated by THC, it enhances the user’s sensory perceptions and mood. It decreases dopamine sensitivity in the limbic system and activates the reward pathway. It also disturbs memory function and learning, leading to impaired judgement. Additionally, it also causes loss of time perception and disruption of psychomotor behaviour and can occasionally lead to psychosis.45-47
As mentioned earlier, cannabis has some beneficial effects on sexual functioning, but its overall long-term effects on sexual health are deleterious. Increased libido in both males and females is a potential benefit and has been demonstrated in many studies to date.48-50 It has also been found to increase sexual frequency, with daily and weekly users having significantly higher sexual frequency compared to never-users. 51 Thus, cannabis is an aphrodisiac with muscle relaxant and pain-relieving properties. The aphrodisiac effect of cannabis is due to the binding of THC at CB1 receptors in the paraventricular nucleus of the hypothalamus. 52 Due to its aphrodisiac effects, cannabis has also been used to potentially manage sexual dysfunctions like decreased sexual desire.49,53 Apart from this, due to its pain-relieving properties, cannabis has also been used to manage dyspareunia due to vaginismus, endometriosis, and so on. 53 Finally, being a muscle relaxant with anti-anxiety properties, cannabis can improve sexual experience and performance at times of stress.51,54
Negative effects of cannabis on sexual health have been typically found in heavy and/or long-time users. This is especially true with ED. Owing to its muscle relaxant properties, cannabis users have reported difficulty in achieving and maintaining erection with full-blown ED being a problem in heavy and chronic users.48,55 Cannabis has also been shown to produce vascular endothelial dysfunction and damage. Veno-occlusive plethysmography in such patients has revealed impaired endothelium-dependent vasodilation. 55 All this evidence points to the fact that ED in cannabis users has an organic aetiology and is not psychogenic. Additionally, men have also reported problems with orgasms. Although there is increased intensity of orgasm in cannabis users initially, later it is also associated with problems such as reaching orgasm too quickly as well as reaching orgasm late. A study carried out by Smith et al. 56 in Australia found that people who smoke cannabis daily are four times more likely to have trouble reaching orgasm than men who do not smoke. As found in other studies, frequent users are more likely than others to report two or more sexual partners in the previous year, irrespective of their gender. 57 Also, female daily cannabis users are significantly more likely than non-users to report sexually transmitted diseases in the previous year. 57
Chronic marijuana use has been associated with reduced fertility in both men and women. For couples trying to conceive, it is important to be aware of this potential impact on reproductive health. When used chronically, the active compound THC suppresses the HPG axis. Several animal studies have demonstrated that intraperitoneal administration of THC in rodent animals was associated with a decrease in the levels of LH and FSH.58-60 Lower levels of LH and FSH levels are associated with menstrual irregularities and reproductive problems in females. A study carried out by Mueller et al. 61 revealed that women who had smoked marijuana within 1 year of trying to conceive were twice as likely to have infertility because of ovulatory dysfunction than their counterparts who did not use marijuana (relative risk = 2.1; 95% confidence interval 1.1-4.0). Naturally, such women are prone to resort to assisted reproduction techniques (ARTs). But THC exerts its deleterious consequences during such times as we do. Heavy cannabis use adversely affects in vitro fertilization and gamete intra-fallopian transfer (IVF/GIFT). 62 A study carried out by Klonoff-Cohen et al. 62 found that women who smoked cannabis within a year prior to IVF/GIFT had 25% fewer oocytes retrieved, and these couples also had 28% fewer oocytes fertilized. Another study done in women undergoing ART found that the proportion of pregnancy loss in women who were cannabis smokers at enrolment was significantly higher than in women who were non-smokers or past smokers (54% versus 26%; P = .0003). 63
Suppression of the HPG axis has also been seen in males. The HPG axis plays a critical role in both spermatogenesis and testosterone production. Many studies have found that THC suppresses LH levels.64,65 Vescovi et al. 66 carried out a study in daily cannabis users versus non-users and reported significantly lower LH levels in users as well as low response to exogenous gonadotropin-releasing hormone (GnRH) when compared with non-users. Low LH levels also mean low testosterone levels that can affect the process of spermatogenesis. Animal studies have demonstrated decreased spermatogenesis and spermatogenetic arrest in animals with THC exposure. Human studies have also demonstrated a reduction in sperm count and concentration after THC exposure. Additionally, CB1 receptors have been found on sperm, the activation of which has been shown to reduce sperm mitochondrial transmembrane potential. 67 Whenever applied to sperm in vitro, THC caused an immediate decline in sperm mitochondrial oxygen consumption. 68 Thus, activation of CB1 receptors on the sperm also affects sperm motility, contributing to reproductive problems.
Opioids (Morphine and Heroin)
Morphine and heroin are illicit recreational substances that belong to the opioid class of drugs. These act on specific receptors in the brain and body, known as opioid receptors. They are primarily used for their pain-relieving properties but can also produce feelings of euphoria and relaxation.
Morphine is a natural opioid alkaloid derived from the opium poppy plant, scientifically known as Papaver somniferum. 69 It is typically administered in medical settings to manage severe pain, such as that experienced after surgery, trauma or in individuals with certain medical conditions like cancer. Morphine is considered the gold standard for pain relief and is an essential medication in healthcare settings. However, it also has a high potential for addiction and abuse, leading to strict regulation and control. Heroin on the other hand is a semi-synthetic opioid derived from morphine. 70 It was originally synthesized in the late 19th century as a modification of morphine and marketed as a cough suppressant. However, it was later discovered to be highly addictive and dangerous.
Morphine and heroin can both have significant negative effects on sexual health. Long-term use of opioids has been linked with suppression of the HPG axis, leading to an occurrence of opioid-associated endocrinopathy known as ‘Opioid-associated androgen deficiency (OPIAD)’. 71 Opioids decrease the secretion of GnRH from the hypothalamus.72,73 Consequently, there is a decrease in the secretion of gonadotropins (LH and FSH) from the pituitary, ultimately leading to decreased production of sex hormones (testosterone and oestrogen). 73 Apart from hypogonadism that is caused centrally, increased catabolism of testosterone peripherally is also an important factor responsible for lower testosterone levels in males. In a study carried out by Aloisi et al., 74 it was demonstrated that even a single subcutaneous injection of morphine significantly altered the levels of 5-alpha reductase type 1 and/or P450 aromatase expression in different body regions. 5-Alpha reductase is responsible for the peripheral conversion of testosterone to dihydrotestosterone, and the aromatase enzyme is responsible for the conversion of testosterone to oestrogen. An increase in the levels of these hormones after morphine administration also highlights the catabolic effect of opioids on testosterone. 74 It can therefore be said that following chronic opioid use, testosterone is not only produced in lesser quantities due to central suppression, but it is also metabolized to a greater extent, thereby leading to significantly reduced blood and brain testosterone levels. This leads to hypogonadism, decreased libido in males with fewer spontaneous erections, infertility due to low sperm count and even ED if the levels of testosterone are too low for a long period of time. Opioid antagonists like naltrexone have been shown to improve the symptoms of hypogonadism and ED. 75 Another source of androgen production is the adrenal glands. Serum dehydroepiandrosterone (DHEAS) levels are indicative of adrenal androgen production. Chronic opioid use has been associated with decreased DHEAS levels, indicating a reduction in adrenal androgen production. 76 In female opioid abusers as well, OPIAD is responsible for the majority of sexual problems. Decreased levels of LH and FSH are associated with menstrual abnormalities and infertility. 77 Furthermore, reduced levels of testosterone in females also affect their libido. A decrease in levels of sex hormones can delay or inhibit orgasm in both men and women, making it more difficult to achieve sexual satisfaction. Additionally, opioids can decrease sensitivity to physical sensations, potentially leading to less intense or satisfying sexual experiences. Finally, individuals addicted to heroin or morphine may engage in risky sexual behaviours, including unprotected sex, which can increase the risk of sexually transmitted infections and unintended pregnancies. 78
Cocaine and Ecstasy (MDMA)
Cocaine and ecstasy (also known as MDMA) are both psychoactive substances with distinct effects on the central nervous system. Although they have different mechanisms of action, the final outcome of their action brings about an increase in the levels of monoamine neurotransmitters in the synapses. Hence most of the effects of cocaine and ecstasy on the human body are similar, especially when it comes to their effects on sexual health.
Cocaine is one of the most common illicit psychostimulant drugs abused throughout the world. It is a naturally occurring sympathomimetic alkaloid derived from the leaves of the plant, Erythroxylon coca. 79 It is either available as a white powder, viz. cocaine hydrochloride, which is commonly either snorted or injected intravenously; or it is available in its solid free base form, viz. crack-cocaine, which is abused via inhalation of its fumes (smoking). 79 Cocaine primarily works by blocking the reuptake of neurotransmitters, such as dopamine, norepinephrine and serotonin, in the brain. This leads to an accumulation of these neurotransmitters in the synaptic cleft, thereby enhancing their sympathetic effects and producing feelings of euphoria and increased energy. 80
Cocaine can have various effects on sexual health, and although some individuals may initially perceive increased arousal or pleasure, the overall impact on sexual function can be negative. While cocaine has been known to increase libido in both males and females, 81 certain studies have found no effects of cocaine on sexual interest and activity.82,83 Speedball, which is the combined use of cocaine and alcohol, is also known to increase sexual desire and activity in humans. This is because, in the presence of alcohol, cocaine undergoes a process of transesterification, forming a psychoactive metabolite, cocaethylene, with a biological activity like that of cocaine, which prolongs euphoria and other effects of cocaine.81,84 This variable effect of cocaine has also been observed on erectile function and ejaculation in males. While some studies have demonstrated ED to the point of even impotence, others have shown that spontaneous erections can occur, especially after intravenous injections of cocaine. 83 Similar effect is also observed in ejaculation. Certain studies have demonstrated pre-mature ejaculations after cocaine use, whereas some have implicated cocaine to cause impaired ejaculation or inhibition of ejaculation. 83 This variation can be explained by the fact that dopamine promotes seminal emission and ejaculation through the D2 dopaminergic receptors, whereas serotonin has an inhibitory effect on orgasm and ejaculation through the serotonin (5-HT) receptors. 85 Cocaine brings about an increase in the levels of both serotonin and dopamine by blocking their reuptake. But overall, chronic cocaine use has been found to cause not only decreased libido and ED but also delayed orgasm/ejaculation probably due to lower levels of monoamine neurotransmitters owing to exhaustion. 86 Furthermore, dissatisfaction with sexual activity and decreased libido have been reported in females with chronic cocaine use disorder. 83
As far as fertility is concerned, cocaine is especially known to cause serious implications, among the common illicit drugs of abuse. Animal studies have demonstrated that DNA isolated from the testis of rats administered with cocaine showed a time- and dose-dependent fragmentation pattern, typical of apoptosis. 87 Another study conducted by Li et al. 88 has shown germ cell apoptosis in rat testes as early as 15 days following cocaine injection, suggesting chronic cocaine administration as a cause of increased apoptosis. Thus, low sperm count and lower sperm motility are serious adverse effects of chronic cocaine use. 89 Another interesting concept came to light in a study carried out by Yazigi and Polakoski, 90 in which sexually mature mice were injected with titrated cocaine hydrochloride and radioactivity was detected in all organs. It was found that kidneys and sperms within the epididymis contained the highest concentration of cocaine per milligram of tissue. These findings may explain the mechanism of ‘Male-mediated teratogenesis’ by considering the possibility that sperm can transport cocaine into the oocyte during fertilization. 90 In females, even though the data are limited, it has shown cocaine to cause a delay in puberty when abused at pre-pubertal age and ovulation failure in sexually mature females. 84
MDMA
MDMA, also commonly known as ecstasy or molly, is a powerful psychoactive drug that produces feelings of heightened energy and euphoria, to the point of even hallucination. It is an indirect monoaminergic agonist that stimulates the release and inhibits the reuptake of monoamine neurotransmitters in the brain, especially serotonin and dopamine. 91 Like cocaine, its effects on sexual health can be complex and may vary among individuals. MDMA is also called a love drug as it brings about an increase in sexual desire, sensory perceptions and empathy. This is probably a result of activation of the dopaminergic system.92,93 On the contrary, due to the simultaneous activation of the serotonergic system, MDMA users have also reported difficulty in achieving and maintaining erections, lubrication and delayed orgasm.92,94 In fact, a survey carried out in San Francisco among MDMA users reported decreased erectile ability in about 46% of its male participants. 95 Several surveys and interviews have also demonstrated high-risk sexual behaviour among MDMA users. One such questionnaire-based survey carried out by May and Parrott 96 reported that both male and female MDMA users exhibited more risky sexual behaviours than non-users. This was in the form of higher rates of casual sex, multiple sexual partners, non-condom use during sex and penetrative sexual risk.
LSD
LSD is among the most powerful hallucinogenic drugs that alters a person’s thoughts, perceptions and feelings. It primarily affects the serotoninergic system in the brain via the 5-HT1A and 5-HT2A receptors. Like all hallucinogens (e.g., mescaline and psilocybin), it acts as an agonist at 5-HT2A receptors.97,98 Even though hallucinogens do not bind exclusively to 5-HT2A receptors, it has been evident in both animal and human studies that activation of 5-HT2A receptors is a prerequisite for the generation of hallucinogenesis.99,100 Apart from the serotonergic system, LSD is also a partial agonist of dopamine at the D2 receptor and potentiates dopamine inhibition of prolactin secretion from the anterior pituitary gland. 101
Although LSD is a popular ‘party drug’, research data on this psychedelic is limited owing to a number of reasons. Research on psychedelics was first gravely affected after US President Richard Nixon’s effort to curb the usage of illicit drugs via his campaign, viz. ‘War on Drugs’ in 1971. 102 This was followed by tighter regulations in pharmaceutical research, which led to the decreased interest in sponsors and pharmaceutical companies to fund clinical trials. 102 These reasons together with the social stigma on psychedelics, including LSD, have been a barrier to conducting research. The societal perceptions of LSD as being an illicit drug have hindered objective scientific investigation. Therefore, limited evidence of LSD’s effect on sexual health exists today.
Although both positive and negative effects of LSD have been reported on sexual health, such evidence comes mostly from animal studies and clinical reports on a few people. LSD can enhance sensory perception, leading to more intense and vivid sensory experiences. In a clinical report published in The Journal of Sexual Research, Dr Alpert states that LSD can provide experiential richness, freshness and inter-relatedness. 103 This may induce heightened sensations and enhance sexual pleasure. LSD can also distort the sense of time, making one feel time moves slower. 104 This altered perception might affect sexual experiences, making them feel intense and more prolonged. On the other hand, results from animal studies suggest contradictory findings. Studies done on rats have shown ovariectomized female rats injected with LSD to exhibit a lesser frequency of lordotic behaviour as a response to the mounting of male rats, as well as prolonged latency of copulation and reduced frequency of copulation of male rats injected with LSD.105-107
Conclusion
In conclusion, while the use of recreational drugs may provide temporary pleasure or escape, it is imperative to recognize and understand the intricate relationship between recreational drug use and sexual health. There is a critical need to educate people, especially the younger population, regarding the potential risks and adverse effects of recreational drugs on physical, sexual and mental well-being. Ultimately, cultivating a lifestyle that promotes overall well-being, free from the harmful consequences of substance abuse, contributes to a more fulfilling and sustainable approach to sexual health.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.