
Abstract
Background:
Engaging in regular healthy sexual intercourse activities is good for human health and well-being. Greater sexual intercourse frequency (SIF) for people in relationships is often associated with well-being, greater relationship satisfaction, reduced mortality, increased life expectancy, positive emotions and happiness, while lack of sexual activity is usually associated with depression and marital disharmony.
Aim:
The primary purpose of this study is to identify the factors associated with SIF among women in South Africa.
Data and Methods:
The South African Demographic and Health Survey 2016 data were used, and the negative binomial regression model (NBRM) was employed for analysis.
Results:
Age was significantly associated with high SIF (IRR = 1.02; p < .001). African women had significantly higher SIF than Indian/Asian women (IRR = 1.28; p = .049). Married women had a significantly higher SIF than women who were never married (IRR = 1.42; p < .001). Women who resided in urban areas were significantly associated with higher SIF than women who resided in rural areas (IRR = 1.14; p < .001).
Conclusion:
Being young, being Indian/Asian, being unmarried, and residing in rural areas is associated with low SIF, whereas being older, being African, being married, and staying in urban areas is associated with high SIF. Generally, without violating cultural, religious and societal beliefs, married women should be taught about the benefits of sexual intercourse activity (SIA) and be encouraged not to be ashamed of entering into sexual intercourse activities.
Keywords
Introduction
Engaging in regular healthy sexual intercourse activities is good for human health and well-being.1,2 Greater sexual intercourse frequency (SIF) for people in relationships is often associated with well-being, greater relationship satisfaction, reduced mortality, increased life expectancy, positive emotions and happiness, while lack of sexual intercourse activity (SIA) is usually associated with depression and marital disharmony.2,3-5 SIA reduces stress by increasing the release of oxytocin, and people who are sexually active have better cognitive function. 5 Improved mental health is positively associated with sexual intercourse and sexual pleasure. 6 SIA increases the heart rate and lowers hypertension.1-5
SIA assists in preventing some infections by bolstering the immune function. 5 Vaginal–cervical stimulation cause sensory information to be transported by the vagus nerve to the brain, bypassing the spinal cord and allowing even women with complete spinal cord transection to orgasm from vaginal–cervical stimulation, and not through clitoral stimulation. 7 Vaginal stimulation by a penis delivers substantial major stimulation of the nucleus accumbens. 7 During sexual intercourse, the penis touches the cervix, vaginal–cervical stimulation is activated, vagus connection takes place and, as a result, heart rate variability increases, hypertension lowers and stress reactivity occurs. 7
On the other hand, there are risks associated with engaging in sexual intercourse, especially if protection is not used. Some life-threatening diseases and viruses like the human immunodeficiency virus and the acquired immunodeficiency syndrome (HIV/AIDS) and sexually transmitted infections (STIs) are associated with sexual intercourse because they are likely to be transmitted through sexual activity. 8 These viruses are likely to be transmitted as a result of irresponsible sexual behaviour, like having unprotected sex, and unintended pregnancies may also occur, but not necessarily because of SIF.8,9 A study conducted in the United States of America revealed that above 50% of 20 million new sexually transmitted diseases reported in 2020 were among young people aged 15–24 years. 10
Offspring can result from a single SIA. However, highly irresponsible SIF increases fertility.11-14 High SIF without utilisation of condoms and birth control measures increases the probability of conception and rate and population growth because young women are at the peak of their fertility.11-14 The growth of the population might aggravate problems related to food security, health, biodiversity, climate and energy. 14
It was against this background that this study aimed to identify the factors associated with SIF among South African women.
Problem Statement
Little is known about the factors associated with SIF among South African women. If there are no control measures, high SIF might lead to increased fertility rates that, in turn, might increase the population, which has the potential of further burdening the under-resourced South African government in its attempts to meet the basic human needs such as water, energy. health, education, shelter and the payment of social grants. 14 Due to its continuous population growth, South Africa has a shortage of energy and is unable to meet the country’s electricity demands, and there is a scarcity of schools in Gauteng province.15,16 High instances of irresponsible sexual behaviour may increase the prevalence of HIV and unintended pregnancies. 8 At the time of conducting this study, there was little or no evidence of previous research conducted to examine the factors related to SIF among women in South Africa aged 15–49.
It is envisaged that the findings of this study will benefit the South African government and other countries to come up with policies and control measures to control the high SIF that has the potential to increase population growth.
Theoretical Considerations
Schneidewind-Skibbe et al. reviewed published studies on SIF and associated factors reported by women. 17 Evidence showed that there was a reduction of SIF from the age of 50 years among European and United States women. 17 Among Asian women, the rate of SIF was reported to be high in the 20–30 years age group and was followed by a decline. 17 Brody reviewed previous studies that had examined the possible physiological and psychological health benefits associated with various sexual activities and found that SIF was a significant predictor of both men’s and women’s greater gratification with their mental health. 7 Results also revealed that women who had experienced vaginal orgasms exclusively through the movement of the penis in the vagina were more gratified with their mental health than women who had only experienced orgasms directly through clitoral manipulation. 7
Huber et al. compared the SIF reported by women aged 18–40 years by using two data collection methods. 18 For the prospective method, women were given diaries which they had to complete daily to record whether they had vaginal sexual intercourse. 18 For the retrospective method, information was collected at 3-month intervals for 15 months, whereby women recalled and checked or wrote their answers on postcards and mailed them back to those who were conducting the study. 18 The SIF values of the two methods were converted to weekly averages and a paired t-test was used to test whether the averages of the reported SIF values in the prospective and retrospective methods were different. 18 Linear mixed models were used to test for variation in the responses within demographic categories and other variables. 18 The results of the paired t-test revealed that the average was significantly different, with the mean number of days women had sexual intercourse per week being higher for the 3-month retrospective recall of using postcards than the prospective method of using daily diaries. 8
Smith et al. investigated the associations between sexual activity, problems, and concerns with experienced well-being, measured as enjoyment of life in adults aged 50 years and older, using the English Longitudinal Study of Ageing data, which were representative of the population. 4 One-way independent analysis of variance was used to evaluate the degree to which sexual activities, problems, concerns, and satisfaction were associated with enjoyment of life. 4 It was found that men and women who reported any sexual activity in the past year had substantially higher mean enjoyment of life scores compared with those who were not sexually active. 4
Eisenberg et al. investigated the factors associated with SIF among Americans aged 25–45 years. 2 Negative binomial regression model (NBRM) was used to test for associations between SIF and demographic, socioeconomic, and anthropometric variables. 2 The findings revealed that, among women, being married significantly increased SIF, and current pregnancy significantly lowered SIF. 2 Although not significant, each 5-year increase in age was inversely associated with SIF. 2
Arafat et al. examined and compared SIF among married residents of Bangladesh, India and Nepal. 19 Information regarding weekly and monthly frequency of sexual intercourse was collected. 19 The mean SIFs of weekly and monthly were computed and compared among Bangladeshis, Indians and Nepalese married individuals. 19 The results revealed that Indians had the lowest mean weekly and mean monthly SIF among the three groups compared. 19 Agarwal, Kaur and Kumar studied SIF among Indian women and found that their SIF declined with increasing age. 20 The median SIF for women aged 21–30 years was 2/week, for 31–40 years was 1.4/week and for 41–50 years was 0.5/week. 20 For many decades, the SIF of Indian women has been reported to be low as compared to other ethnic groups.19,20 Nag compared the SIF of Indian and United States women and found that Indian women of different age groups had lower SIF than American White women. 21 The low SIF among Indian women could be attributed to traditional values about moderation of sexual activity, lack of privacy to conduct sexual activity and abstinence due to rituals.20-22 The SIF is low among Indian women as their men do not indulge too much in sexual activity because of a general belief among Hindus that semen is a great source of strength for men, and so men are very much concerned about loss of their strength through coitus. 21 They belief that by conserving their semen they gain strength. 21 In some households, the practice of husbands and wives sharing a room with their children leads to a lack of privacy and prohibits them from engaging in sexual activities. 22
Gupta and Lynn studied sexual behaviour among married Bengalee women. 23 Information on socio-sexual and sexual behaviour was used in this study to understand the sexual behaviours of women. 23 The results revealed that the average coital frequency of all women was 1.4 per week. 23 The average weekly coital frequency was highest among women aged 55–59 years (2.9 per week) followed by women aged 25–29 years (2.0 per week) and was lowest among women aged 50–54 years (0.6 per week). 23 Large families deprived married women of having sex with their husbands as often as they wanted due to a lack of privacy and women fatigued by the household from these big families. 24 Motherhood was found to be the major factor which diminished sex urge in married life. 23
George et al. investigated coital frequency of African women residing in KwaZulu-Natal province in South Africa. 25 Coital frequency was assessed by asking women how many times they had sexual intercourse in the past 12 months before the survey date. 25 Logistic regression model was used to analyse the association between coital frequency and age-disparate partnerships. 25 Approximately 42% of the women had sex 10 times or more with age-similar partners and about 49% had sex 10 times or more with age-disparate partners in the 12 months prior to the survey date. 25 Age-disparate partnerships were associated with a high coital frequency and with sexual intercourse on more than 10 occasions compared with age-similar partnerships. 25
Data and Methods
Data
The South African Demographic and Health Survey (SADHS) 2016 data were used for analysis. 26 The SAHDS 2016 was a national cross-sectional survey that collected information on 8514 women aged 15–49 years old from 11,083 households. 26 The primary objective of the SADHS 2016 was to provide up-to-date estimates of basic demographic and health indicators to assist policymakers and programme managers in evaluating and designing programmes and strategies for improving the health of the country’s population. 26 Among others; the SADHS 2016 contains information about the age of the respondent, marital status, education level, occupation, place of residence and wealth index. 26 The survey protocol was reviewed and approved by the South African Medical Research Council Ethics Committee and the ICF Institutional Review Board. 26
Measures of Covariates and Data Cleaning
Women who did not give information about the number of times they had sexual intercourse in the last 12 months before the interview date were dropped from the analysis. Also, women who had never engaged in SIA did not form part of the analysis. The highest number of times they had sexual intercourse was recorded as 95+ in the SADHS 2016 data. The 95 in the analysis of this study therefore means they had sexual intercourse 95 times or more. The covariates considered for analysis are the age of the respondent, age at first sexual intercourse, ethnicity, marital status, education level, and the respondent’s occupation, wealth and place of residence. The age of the respondent and age at first sexual intercourse are recorded in years with no decimals.
Outcome Variable
SIF in the last 12 months is the outcome variable. The outcome variable is a quantitative discrete type of data and is recorded as the count of the times the respondent had sexual intercourse in the last 12 months before the date of interview. 25
Statistical Models
Poisson Regression Model and the Evaluation of the Model
Poisson regression analysis is a regression technique that can be used to model the counts or occurrence rates of a dependent variable.
27
One of the assumptions of a Poisson regression model (PRM) is that the mean and variance must be equal.28,29 The observed variance of the data may be larger or smaller than the corresponding mean, causing over-dispersion or under-dispersion, respectively.
29
An over-dispersion occurs when the variance is much greater than the mean.
27
The reverse is under-dispersion and this will produce severe underestimates of the standard errors and thus overestimates the p values (making them more likely to be p < .05).
27
This assumption was evaluated using STATA 14 (statistical software package) using the procedure proposed by Cameron and Trivedi as described by Fávero et al.
30
At the initial stage of assessing over-dispersion, it was found that the variance of the dependent variable, SIF, was much greater than the mean (mean = 52.16; variance = 1508.90). The PRM with all covariates was run, followed by generating the predicted number of events (n̂) and then creating the variable y*:
where
NBRM and the Evaluation of the Model
The NBRM was implemented since the assumption of equidispersion for PRM was violated. The NBRM is a more flexible extension of the Poisson distribution that does not assume an equal mean and variance; instead, it corrects for over-dispersion in the data and is appropriate where the variance is larger than the mean.31-33 In the negative binomial distribution, the response variable Y is assumed to follow a Poisson distribution with a mean λ, but the dispersion α is assumed to follow a gamma distribution, so it is also called the Poisson-Gamma distribution. 34 The Poisson distribution is made up of one parameter, its mean λ but the negative binomial distribution is a function of both λ and α where λ is the mean and α is the negative binomial dispersion/shape parameter.31,35 If α = 0, the negative binomial distribution reduces to Poisson distribution. 35
The negative binomial distribution can be derived from applying the general form of the binomial theorem with a negative exponent; hence the term negative binomial.
34
For example:

The x-th term in the series above is:

where Y is negative binomial with probability of success π and shape parameter α.
33
Alternatively, negative binomial distribution can be derived by joining the Poisson and Gamma distributions together.31,33 The negative binomial distribution with mean λ (λ > 0) and shape parameter α (α > 0) is given by:
and can be re-written as:

where
The model fit of the NBRM can be assessed by calculating the dispersion ratio, which is Pearson Chi – Square value/df or Deviance/df and, if the dispersion ratio is equal to 1, the PRM would be adequate. 36 However, if the dispersion ratio is much greater than 1, the NBRM would be the adequate model to fit.36,37 Alternatively, the dispersion parameter α can be utilised to determine whether the NBRM is the appropriate model to fit.37,38 If the dispersion parameter is α = 0 or is close to 0, the PRM would be the suitable model to fit; otherwise, if the dispersion parameter is different from 0, the NBRM is the suitable model to fit.37,38
The dispersion ratios of Pearson Chi – Square value/df and the dispersion ratio of Deviance/df were much greater than 1 (respectively 28.14 and 31.95), supporting the relevance of the NBRM. In addition, the dispersion parameter α = 0.901 with a 95% confidence interval of (0.8725; 0.9313) indicated the appropriateness of the NBRM. The likelihood ratio test which tests whether the shape parameter α is zero, (H0 = α = 0), showed that α was significantly different from zero (p < .001), implying that the NBRM was appropriate to be used for data analysis in this study. The standard errors and the z-scores were lower in the NBRM than those in the PRM.
The NBRM is used to analyse count data and was chosen over the Poisson distribution as the Poisson distribution would not give accurate estimates because it failed to meet some of the theoretical assumptions. The dependent variable was not categorised into binary outcomes. Therefore, the logistic distribution was not used. From the literature, Eisenberg used NBRM to investigate the association between SIF and explanatory variables. 2
Results
The results in Table 1 show that analysis was carried out on 6 489 women aged between 15 and 49 years with an average age of 31.3 years. On average, women engaged in SIAs 52.2 times a year, with a minimum and maximum of one (1) and more than 95 times, respectively. The results in Table 2 show, under ethnicity, most women were Africans (5 656; 87.2%) followed by Coloureds (606; 9.3%) and Whites (166; 2.6%), and Indian/Asian women were the minority (61; 9.4%). Regarding marital status, the majority were women who were never married (3415; 52.6%), followed by married women (2728; 42.0%) and divorced/separated women (231; 3.6%), and the fewest were widowed women (115; 1.8%). With regard to education level, the majority of the women had secondary education (4964; 76.5%), followed by women who had higher education (746; 11.5%) and women with only primary education (632; 9.7%), and last were women who had no education (147; 2.3%). In terms of occupation, most women were unskilled and held unskilled jobs (4148; 63.9%). They were followed by those who held jobs that required medium skills (905; 14.0%) and those who were not working (836; 12.9%). The women who held professional jobs were in the minority (600; 9.3%). Regarding wealth, most women were poor (2791; 43.0%), followed by rich women (2164; 33.4%) and those who were neither rich nor poor (1534; 23.6%). More women lived in urban areas (3661; 56.4%) than in rural areas (2828; 43.6%).
Summary Statistics of the Quantitative Continuous Variables.

Summary Statistics of the Categorical Variables and the SIF Averages for Each Category.
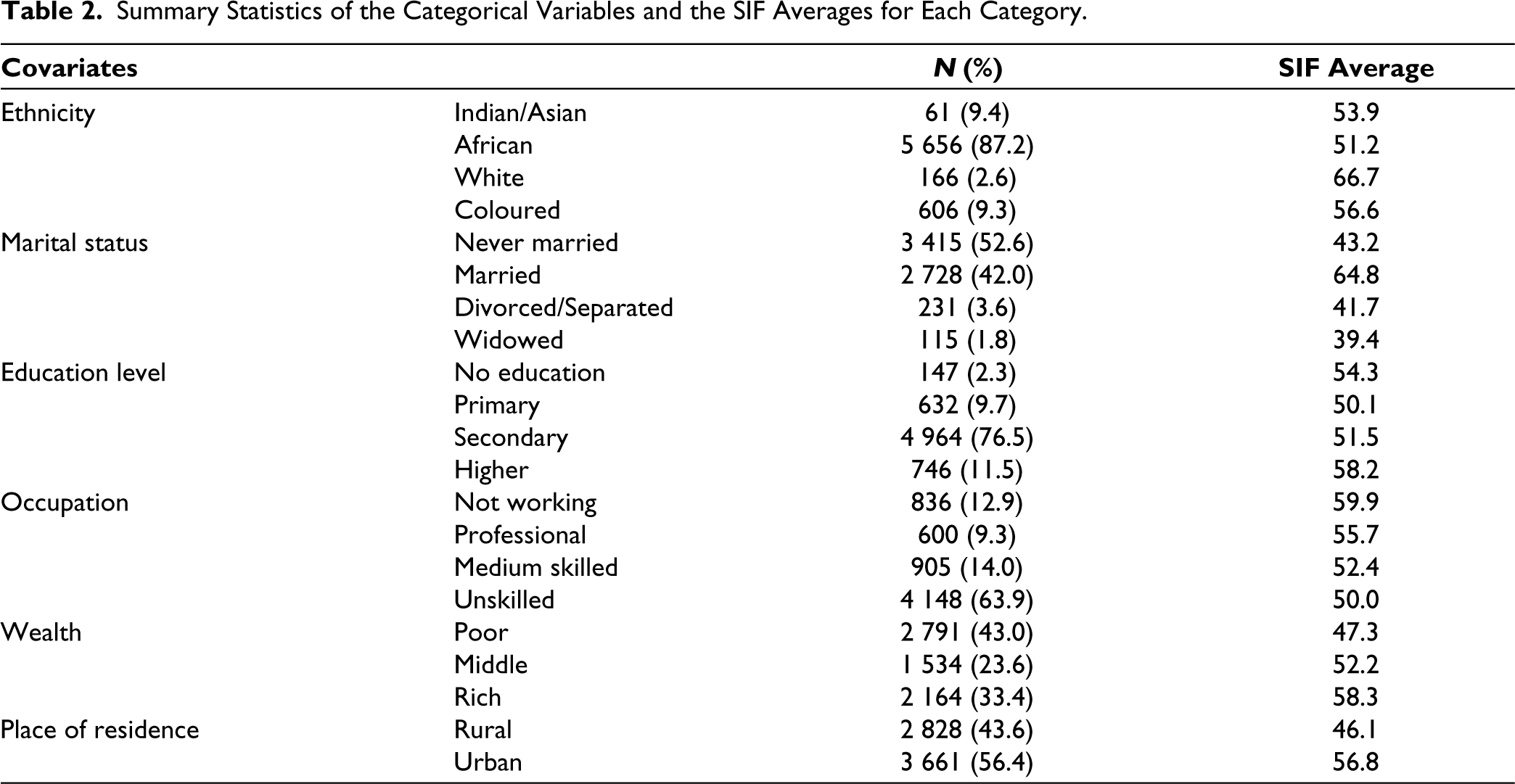
On average, the highest SIF was found among white women who performed it 66.7 times a year, followed by married women with an average SIF of 64.8 times a year. On average, the lowest SIF was found among widowed women who performed it 39.4 times a year, followed by divorced/separated women with an average SIF of 41.7 times a year.
The results of the multivariate NBRM are presented in Table 3 and are reported in incidence rate ratios (IRRs) to estimate the relationships between SIF and the selected independent variables. The results of each variable are reported after controlling for all other variables in the model. Age was significantly associated with high SIF (IRR = 1.02; p < .001). For every 1-year increase in the ages of the women, the SIF increased by 2%. Age at first sexual intercourse was not significantly associated with high SIF (IRR = 1.001; p = .793). African women had significantly higher SIF than Indian/Asian women (IRR = 1.28; p = .049). The SIF of African women was 28% significantly higher than that of Indian/Asian women. White women had a slightly higher SIF than Indian/Asian women (IRR = 1.25; p = .126). Coloured women had a slightly higher SIF than Indian/Asian women (IRR = 1.18; p = .204).
Results of the Multivariate Negative Binomial Regression Model.
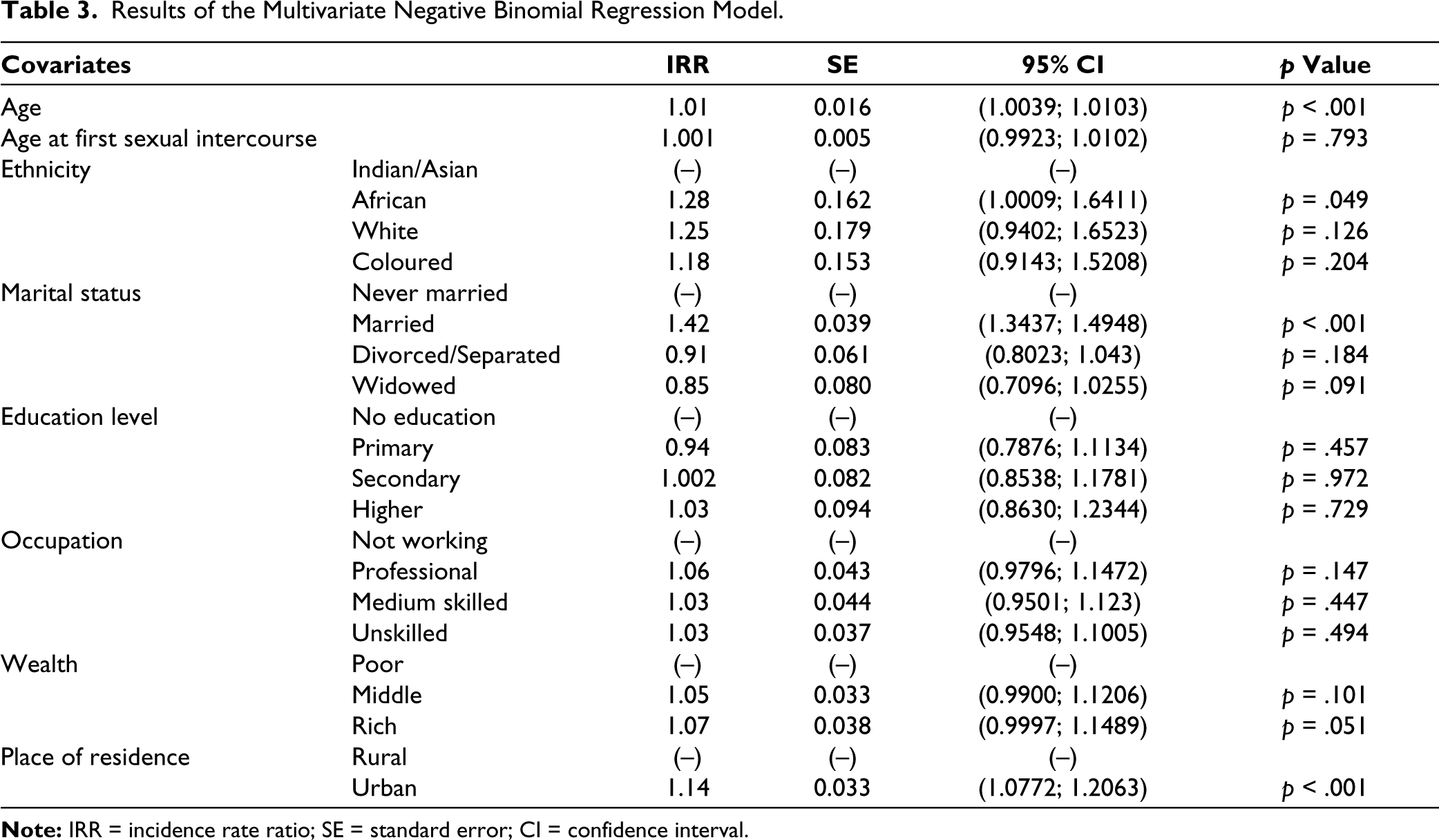
Married women had a significantly higher SIF than women who were never married (IRR = 1.42; p < .001). They had a SIF that was 42% significantly higher than that of women who were never married. Divorced/separated women had a slightly lower SIF than women who were never married (IRR = 0.91; p = .184). Likewise, widowed women had a slightly lower SIF than women who were never married (IRR = 0.85; p = .091).
Women who had primary education had a slightly lower SIF than women with no education (IRR = 0.94; p = .457). However, women with secondary education had slightly higher SIF than women with no education (IRR = 1.003; p = .972). Likewise, women who had higher education had a slightly higher SIF than women with no education (IRR = 1.03; p = .729).
Women who held professional jobs (IRR = 1.06; p = .147), women who held medium-skilled jobs (IRR = 1.03; p = .447) and unskilled women (IRR = 1.03; p = .494) had higher SIF than women who were not working, but the differences were not statistically significant. Women who were neither poor nor rich (IRR = 1.05; p = .101) and rich women (IRR = 1.07; p = .051) had higher SIF than poor women, but the differences were not statistically significant. Place of residence was significantly associated with SIF. Women who resided in urban areas were more significantly associated with high SIF than women in rural areas (IRR = 1.14; p < .001): The SIF of urban women was 14% significantly higher than that of rural women.
Discussion
The study helped to identify the factors associated with SIF among women in South Africa. Age, ethnicity, marital status and place of residence were identified as significant predictors of SIF among South African women. The revelation that the rate of SIF increased with the age of the women is in line with the findings by Schneidewind-Skibbe et al., who reported that SIF was high among women aged 20–30 years. 17 SIF is likely to be low among women younger than 20 years because they attend school and stay with their parents, which makes their chances of having high SIF low. It is not good for women of school-going age to engage in sexual intercourse. They might fall pregnant and be infected with sexually transmittable diseases like HIV/AIDS and STI. A South African study in 2017 revealed that the highest new HIV infections were found in women aged between 15 and 24 years. 39
Sexual activity varies across religious, cultural, and ethnic groups, reflecting diverse beliefs, values, and practices regarding intimacy and relationships. 25 Indians/Asians had lower SIF than other ethnic groups. The rationale could be that, in the Indian community, sex is not conducted for the purpose of pleasure and enjoyment.21,24 The members of this community believe that sex is an essential activity appropriate only after marriage and is a way of reproduction.22,26 Abstinence from sex is considered a virtue in Hindu religious scriptures. 24 The women are submissive to their husbands and do not complain when they are not sexually satisfied. 22 In the African, White and Coloured communities of South Africa, there is no evidence of a culture that prohibits coital frequency, whether before, during or after marriage. This could be the reason of why their SIFs were higher than those of Indians/Asians.
Married women were significantly associated with higher SIF than unmarried women and the finding agrees with the finding by Eisenberg et al. 2 The rationality for this finding could be that married women stay with their husbands and do not have to abstain from sex. Most women get married when they are more than 18 years old and start to engage more in SIAs. These results are also consistent with the results of the current study which indicate that SIF increases with age. SIF increases with age because most women enter into their marriages as they exit their teenage ages.
The place of residence was associated with SIF. Rural women see sex as for the pleasure and enjoyment of their men (husbands or boyfriends) only and not for both of them. In a study conducted by Younis, Ibrahim and Radwa, it was reported that higher percentages of urban women than of rural women stated that the purpose of sexual intercourse was to obtain pleasure for both them and their husbands. 40 Rural women saw sexual intercourse as a duty that they must render to their husbands. 40 Their husbands and boyfriends spend the majority of their time in the cities where they work and only visit their wives and girlfriends fortnightly or once a month, hence their SIF is low. Many rural women do hard labour and come back home very tired and so cannot enter into SIAs as often as they would love to. 41 Many of the urban-based women do not do hard labour and can afford to hire someone to help them with household chores so, in the evening, they are not so tired and can engage in SIAs.
Conclusion
The purpose of this study was to identify the factors associated with SIF among women in South Africa. The results reveal that age, ethnicity, marital status and place of residence are significant factors associated with SIF. The findings are that SIF increases substantially as women age. African women are more significantly associated with high SIF than Indian/Asian women. In addition, married women are more significantly associated with high SIF than women who are not married. Furthermore, urban women are more significantly associated with high SIF than rural women. No significant associations were found between age at first sexual intercourse, education level, occupation, or wealth. Being young, being Indian/Asian, being unmarried, and residing in rural areas is associated with low SIF, whereas being older, being African, being married, and living in urban areas is associated with high SIF. Generally, without violating cultural, religious and societal beliefs, married women should be taught about the benefits of SIA and be encouraged not to be ashamed of entering into sexual intercourse activities.
High SIF is linked to stronger relationship quality, longer relationship duration, and reduced desire for additional sexual partners. 42 This decrease in multiple partnerships could potentially lower the transmission rates of STIs and HIV/AIDS. Consequently, this can alleviate the financial burden on governments associated with healthcare costs related to these diseases. Therefore, policymakers should prioritise developing educational programmes and policies to promote safe sex practices and emphasise the benefits of maintaining intimacy. Policymakers can implement health education programmes with focus on communication skills, consent, mutual respect, healthy sex, condom use, and negotiation within relationships to empower women to make informed choices about their sexual lives. The study revealed that rural women were not associated with high SIF. Generally, traditional leaders are based in rural areas. People respect them and listen to them. The government can arrange training for traditional leaders to learn about the good of sexual intercourse. In turn, these traditional leaders should teach or facilitate workshops where their people can be taught about the goodness and benefits of sexual intercourse. There is a limitation of studies that compare SIF by ethnicity. There is a need for future research to focus on comparing SIF by ethnicity.
Limitations
The type of sexual intercourse was not defined or described to the respondents in the SADHS 2016. The term sexual intercourse is generally understood to mean vaginal intercourse wherein the penis of a man is inserted inside the vagina of a woman, whereas some people perform other types of sex.43,44 It is possible some respondents could have reported the frequencies of other types of sex instead of sexual intercourse. Sex is sensitive to some people. Some women might have not felt comfortable providing accurate information about their SIF, leading to underreporting or misreporting, which could affect the results of this study. This could be due to various reasons such as cultural norms, personal beliefs, or past experiences. SIF data collected in SADHS 2016 rely on self-reporting, which can introduce inaccuracies due to recall bias or social desirability bias.
Footnotes
Acknowledgements
The author thanks the government of South Africa for collecting the data used in this study and for making them available to the public. Also, the author expresses gratitude to Mantshweng Phiniciah Masemola for explaining why rural women do not often engage in sexual intercourse activities.
Declaration of Conflicting Interests
The author declares no potential conflict of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable
Funding
The author received no financial support for this research, authorship, and/or publication of this article.
Informed Consent
Not applicable