
Abstract
Background:
Virtually all aspects of the human sexual response are affected by alcohol. Chronic and persistent alcohol use has been seen to impair erectile, orgasmic and ejaculatory capacities, which leads to marked distress and interpersonal difficulty.
Aims and Objectives:
To study the prevalence and types of sexual dysfunction and to study the impact of the severity of alcohol dependence on sexual dysfunctions in male patients with alcohol dependence syndrome.
Methodology:
A cross-sectional study was done at the outpatient Department of Psychiatry of a tertiary teaching hospital. Socio-demographic details of the patient and alcohol-related clinical variables were collected using the study proforma. The severity of alcohol dependence was assessed using the Alcohol Dependence Scale (ADS). To assess the presence of sexual dysfunction, the Arizona Sexual Experience Scale (ASEX) was used and the type of sexual dysfunction was decided by the Sexual Dysfunction Checklist (SDC) based on ICD 10, and the data was analysed.
Results:
170 male patients with alcohol dependence, with a mean age of 35.84 years, participated in the study. The prevalence of sexual dysfunction was 67.06%. Loss or lack of sexual desire was the most common sexual dysfunction, followed by failure of genital response (erectile dysfunction), frequency dissatisfaction and premature ejaculation. The majority of the sample studied had one or more sexual dysfunctions. The ADS score positively correlated with the ASEX score, and this correlation was statistically significant.
Conclusion:
Alcohol use was found to be associated with sexual dysfunctions, and lack of sexual desire was the most common sexual dysfunction.
Introduction
Sex and psyche are closely related to each other. Various studies have found that 60%–90% of patients with sexual dys- functions have a psychogenic basis, and in every psychologi- cal problem, a host of sexual problems prevail.1–2 Alcohol dependence is a cluster of physiological, behavioural and cognitive phenomena in which the use of alcohol takes on a much higher priority for a given individual than other behaviors that once had greater value.
Alcohol use disorders and sexual functioning are known to have a complex relationship. 3 It has been suggested that alcohol use enhances the desire of sexual activity. 4 However, the association between long-term and high amounts of alcohol consumption and sexual dysfunction has been widely reported, 5 and men with sexual dysfunction are frequently noted to be chronically alcohol dependent. 6
The rates of sexual dysfunction in the alcohol- dependent population have ranged from 40% to 95.2%, with rates being consistently much higher in the alcohol- dependent population than in the healthy controls or social drinkers. Virtually all aspects of the human sexual response are affected by alcohol: libido is reduced, performance is impeded and dissatisfaction ensues. The common dysfunctions reported have been erectile dysfunction, premature ejaculation, retarded ejaculation and decreased sexual desire. Chronic and persistent alcohol use impairs erectile, orgasmic and ejaculatory capacities, which leads to marked distress and interpersonal difficulty.
It has been observed that in spite of such a wide prevalence, sexual dysfunctions are given low priority and physicians either show no interest or tend to ignore patients’ psychosexual complaints. 7 Also, most patients are reluctant to seek help due to feelings of embarrassment. Hence, it is very important to train the faculty and staff about the relationship between alcohol abuse and psychosexual dysfunctions. 8
There are some studies that have looked into sexual dysfunction due to alcohol, but there are only a few studies reported from India, and hardly any of them have assessed the impact of the severity of alcohol dependence on sexual dysfunction. Hence, this study was undertaken.
Aims and Objectives
To study the prevalence and types of sexual dysfunction in male patients with alcohol dependence syndrome.
To study the impact of the severity of alcohol dependence on sexual dysfunctions in male patients with alcohol dependence syndrome.
Materials
Study Proforma
It consisted of questions regarding socio-demographic factors such as age, education level, occupation and socioeconomic status of the patient. It was also used to record relevant details of the illness, namely the type and duration of alcohol and the results of Alcohol Dependence Scale (ADS), Arizona Sexual Experience (ASEX) and Sexual Dysfunction Checklist (SDC).
Clinical Descriptions and Diagnostic Guidelines Based on ICD 10 Classification of Mental and Behavioural Disorders 9 by WHO
A diagnosis of alcohol dependence was made using the ICD 10 criteria.
Measurement Tools
Alcohol Dependence Scale
It is a reliable and valid quantitative measure of the severity of alcohol dependence, which covers alcohol withdrawal symptoms, impaired control over drinking, awareness of a compulsion to drink and increased tolerance to alcohol. Total scores can range from 0 to 47. 10 Scores between 1 and 13 indicate a “low” level of alcohol dependence; scores between 14 and 21 indicate an “intermediate” level of alcohol dependence; scores between 22 and 30 indicate a “substantial” level of alcohol dependence and scores between 31 and 47 indicate a “severe” level of alcohol dependence.
Arizona Sexual Experience Scale
The ASEX scale is used to quantify sexual functioning in the domains of sexual drive, arousal, penile erection, ability to reach orgasm and satisfaction from orgasm over the past week. Each item is rated from 1 to 6. A total score of more than or equal to 19 or a score of 5 or more on any one item or a score of 4 or more on any three items of ASEX is associated with clinical sexual dysfunction. Reliability coefficients for internal consistency and test–retest reliability for ASEX are considered to be excellent. 11
Sexual Dysfunction Checklist
It contains items corresponding to 12 areas of sexual dysfunction described in the Diagnostic Criteria for Research, ICD-10 Classification of Mental and Behavioural Disorders, 11 to assess the presence and type of sexual dysfunction.
Methods
Study area: The study was conducted at the outpatient Department of Psychiatry at K. J. Somaiya Medical College, Hospital and Research Centre, Sion, Mumbai.
Study population: 170 male patients with alcohol dependence syndrome attending the outpatient Department of Psychiatry were recruited.
Sampling method: Simple random sampling.
Study design: Single interview cross-sectional study.
Sample size: Total 170 patients with alcohol dependence.
Sample size was calculated by the statistical formula for quantitative data, that is., N = 4pq/L 2
p = proportion = 72%
q = 100, p = 28
L = allowable error = 10%, p = 7.2
Sample size n = 155 + 15 = 170
(at 95% confidence interval and 80% power of study)
Inclusion Criteria
Patients with an ICD-10 diagnosis of alcohol dependence syndrome
Male patients
Age: 20–50 years
Married or having a regular sexual partner
Those who were willing to give written informed consent
Exclusion Criteria
Patients with a clinically assessed history of primary sexual dysfunction (prior to the initiation of alcohol use)
Patients with co-morbid medical, surgical or psychiatric disorders or on drugs affecting sexual dysfunction
Patients with substance dependence other than nicotine.
Methodology
A sampling frame of all possible eligible participants was prepared. The random numbers were generated for the selection of the required number of eligible participants using a computer. These participants were enrolled in the study, and a sample size was achieved.
All the patients were informed about the nature of the study and its applications, and valid informed consent was taken.
Socio-demographic details of the patient and alcohol-related clinical variables were collected using the study proforma.
The severity of alcohol dependence was assessed using ADS.
To assess the presence of sexual dysfunction, the ASEC was used.
The type of sexual dysfunction was decided by the SDC based on ICD 10.
Statistical Analysis
The data obtained was entered using a Microsoft Excel Sheet and was analysed using Statistical Package for Social Sciences (SPSS) software version 17.
Results obtained were presented using tables and figures.
The chi-square test was used as a test of significance.
Results
In the present study, 170 patients fulfilling the inclusion and exclusion criteria were assessed.
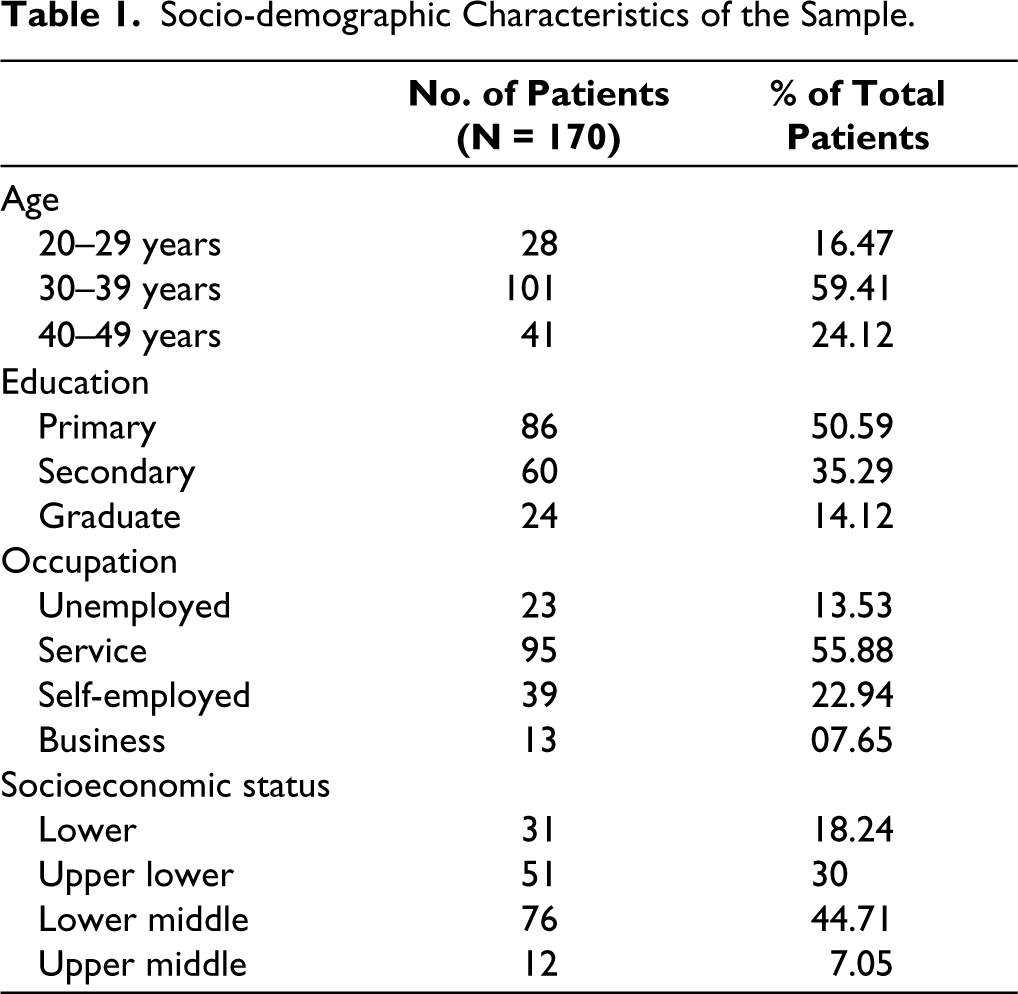
As seen in Table 1:
Socio-demographic Characteristics of the Sample.
The majority of the patients (87%) with alcohol dependence also had nicotine consumption in the form of tobacco chewing and/or smoking bidis or cigarettes, as seen in Table 2.
Nicotine Consumption with Alcohol Dependence.

Table 3 shows the duration of alcohol dependence. One-third (67.06%) of the patients had 6–10 years of alcohol dependence, 11.76% had 1–5 years of alcohol dependence and 21.18% had more than 10 years of alcohol dependence. The mean duration of alcohol dependence in this study was 8.3 (±3.12) years.
Duration of Alcohol Dependence.

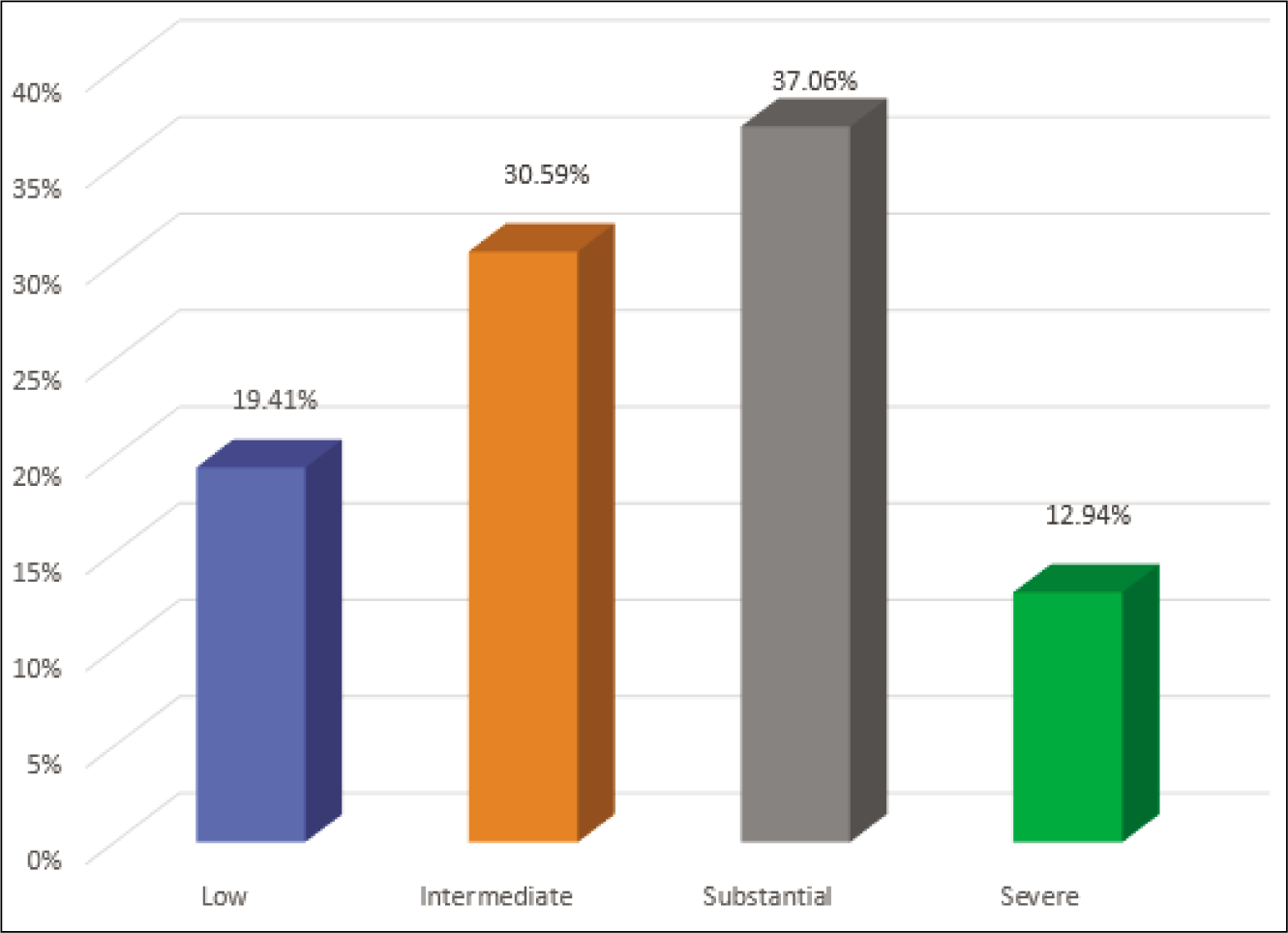
As seen in Figure 1, a majority of the patients (37.06%) had “substantial” level of alcohol dependence (score between 22 and 30), 30.59% had “intermediate” level (score between 14 and 21), 19.41 % had “low” level (score between 1 and 13) and 12.94% had “severe” level (score between 31 and 47) of alcohol dependence.
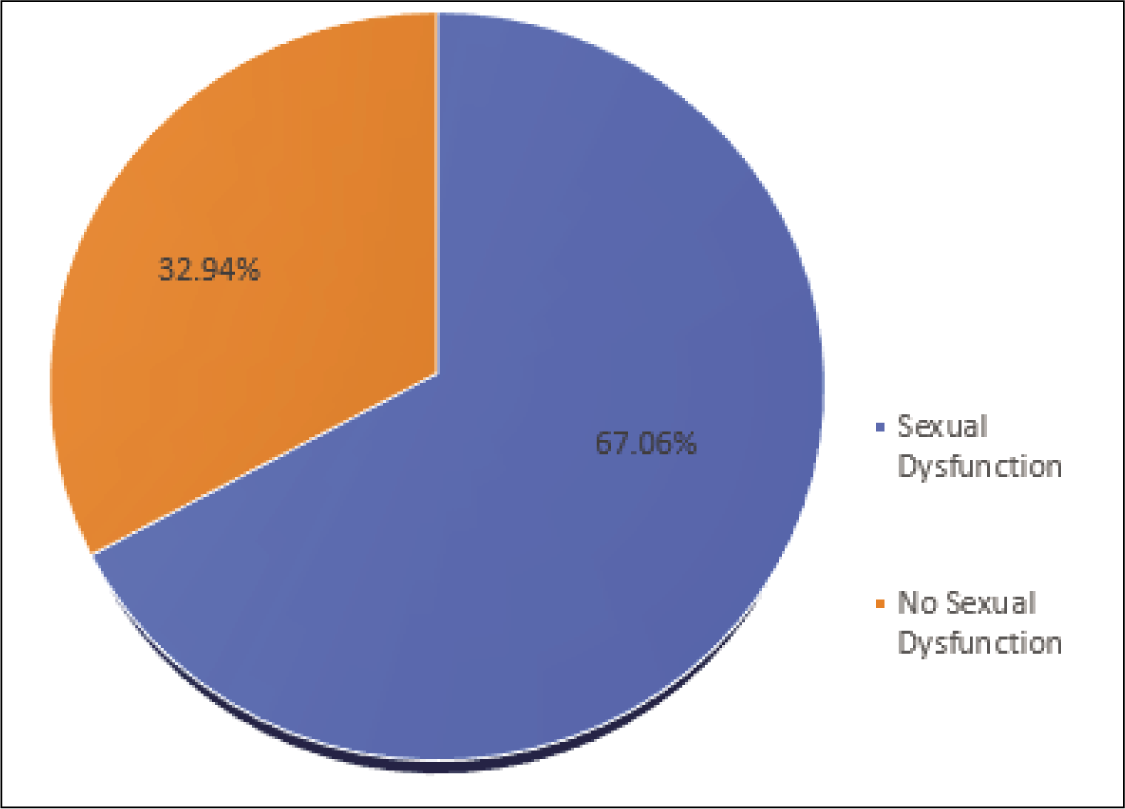
In this study, 114 out of 170 (67%) patients with alcohol dependence had sexual dysfunction. Of the 114 patients with sexual dysfunction, 26 patients had only one type of sexual dysfunction (Figure 2).
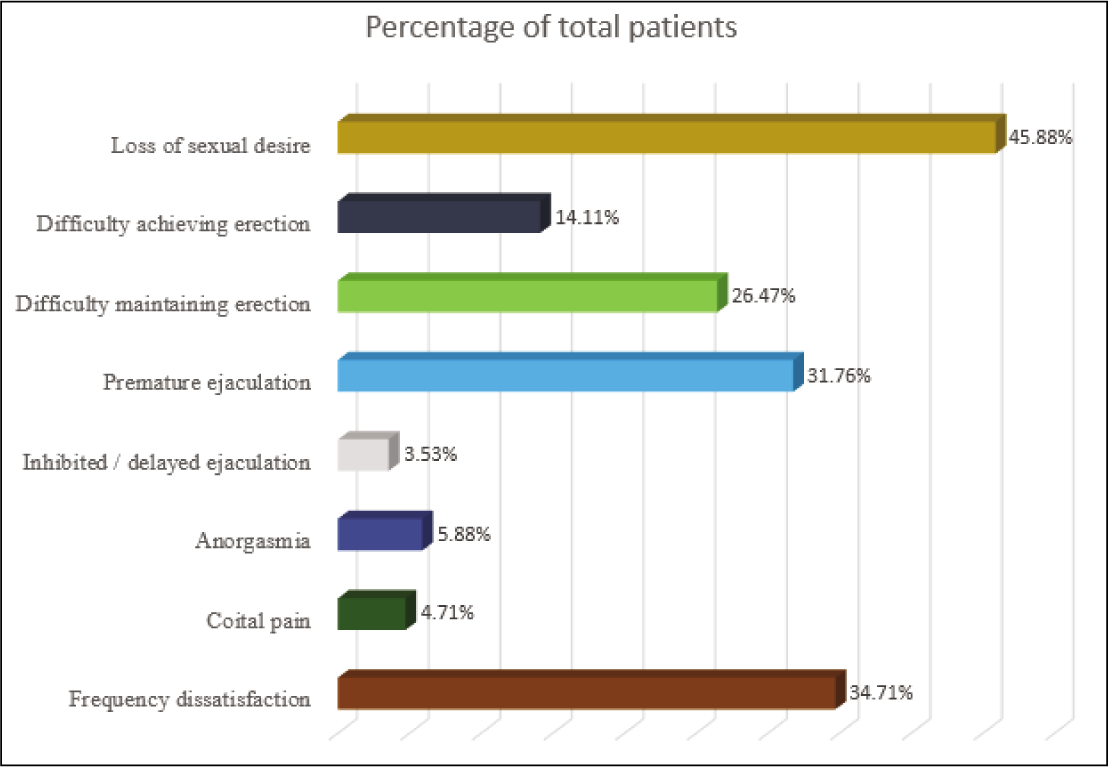
As seen in Figure 3, amongst sexual dysfunctions, loss or lack of sexual desire had the highest prevalence (45.88%), closely followed by failure of genital response (erectile dysfunction), which was approximately 40%. The prevalence of premature ejaculation was 31.76%. Out of 170 patients studied, 34.71% had frequency dissatisfaction, 23% were dissatisfied with their own sexual function, while 10% were dissatisfied with their sexual relationship with their partner. The prevalence of anorgasmia, coital pain and delayed ejaculation was 5.88%, 4.71% and 3.53%, respectively. None of the patients had an aversion to sex or orgasm with a flaccid penis.
The ADS score positively correlated with the ASEX score. This correlation was statistically significant, as seen in Figure 4.
Correlation Between ADS Score and ASEX Score.
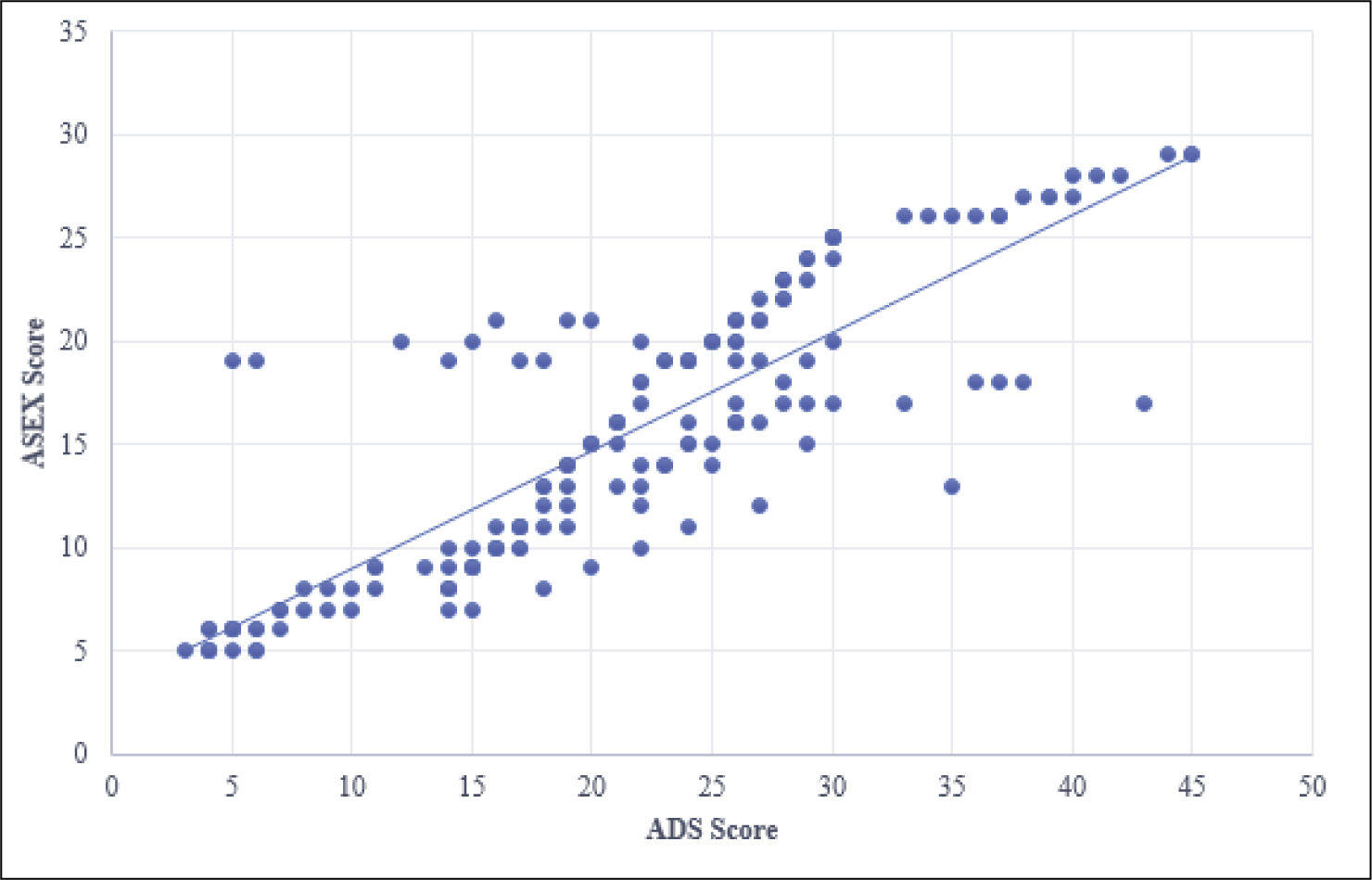
Table 4 shows the impact of the severity of alcohol use on sexual dysfunction. The proportion of sexual dysfunction was 54.5%, 67.3%, 68.3% and 81.8% among the low, intermediate, substantial and severe ADS categories, respectively. However, this observation was not statistically significant.
Impact of Severity on Sexual Dysfunctions.

Also, there was no statistically significant relationship between the severity of alcohol dependence and the type of sexual dysfunction.
Discussion
This study was conducted to assess the prevalence and type of sexual dysfunction in patients with alcohol dependence. A total of 170 patients were included in this study.
Socio-demographic Profile
In this study, a majority of the patients (85%) were more than 30 years old. The mean age of the sample was 35.84 ± 5.96 years, with a range of 22–49 years.
A similar finding was seen in a study conducted by Kishor et al in 2013, where the mean age of the sample was 39 ± 7 years with a sample range of 24–55 years. 12
In another study conducted by Pandey et al, the mean age of alcohol dependence was 37.5 years. 13 A study by Benegal et al in 2005 on alcohol use in India showed that the mean age of the population was 42.6 years. 14
Multiple researchers have consistently demonstrated an association between poor academic achievement and substance use.15–16
Fothergill et al in 2008 found that the risk for substance use disorders increased three- to fourfold if a person had obtained less than a high school education. 17
A prospective study done by Crum et al showed an inverse correlation between the number of years of formal education and alcohol use disorders. It found an association between poor educational achievement and increased risk for alcohol use disorders. 18
Similar findings were seen in the present study, where the majority of the patients (50.59%) had primary education and almost 35% were educated up to the secondary level. There were no post-graduates in the sample studied. The low rate of alcohol dependence in highly educated persons may be due to greater awareness of the harmful effects and inhibitions.
In this study, a majority of the patients (56%) were employed in the service sector, while approximately 14% were unemployed.
This is similar to the findings in a study done by Hazarika et al, where a majority (53%) of the patients were employed in the service sector and 22% were unemployed. 19
A study done by Ghulam et al also showed that a majority (45%) of the population was employed in the service sector. 20
One possible reason why the service class population carries a high risk of substance abuse compared to other occupations is that perhaps persons in these groups need to maintain social relations, and substance use acts as a medium for interaction.
A prospective cohort study assessing the relationship between unemployment and substance use found that the men who had experienced more than 3 years of accumulated unemployment between the ages of 16 and 33 years were more likely to engage in problem drinking than were the men who had never before unemployed. 21
In a study done by Ray et al in 2004, 22 it was seen that significantly higher use of substances was recorded among tribal, rural and lower socioeconomic sections in India.
In the present study, three-fourths (75%) of the patients belonged to the lower middle and upper lower classes.
A study by Aswal et al has also shown that the majority of the alcohol-dependent patients belonged to the upper lower and lower middle classes in terms of the socioeconomic status. 23
Similar findings were seen in a study done by Huckle et al in 2010, in which the lower-to-average socioeconomic status groups were at a greater risk of drinking heavier quantities compared to other socioeconomic status groups in the population. 24
Duration of Illness
In the present study, the duration of alcohol dependence ranged from 1 year to 16 years, and the mean duration was 8.3 ± 3.12 years.
Similarly, in a study done by Arackal et al in 2007, the mean duration of alcohol dependence was 8.59 ± 6.64 years. 25 However, in a study done by Hazarika et al, the mean duration of alcohol use was 17.4 ± 6.3 years. 22
Nicotine Dependence
In a study done by Kumar et al in 2014, it appeared that alcohol and alcohol with tobacco were found to be the most commonly abused substances. 26
In this study, 149 out of 170 patients (89%) had concomitant nicotine consumption along with alcohol dependence. Similar findings were seen in a study conducted at NIMHANS, where the prevalence of tobacco consumption along with alcohol was found to be 87%. 28
Also, in a study done by Pandey et al, it was seen that nicotine (64%) was the most common other substance of use after alcohol. 15
Alcohol Dependence and Sexual Dysfunctions
Sexual dysfunction appears common among male subjects with alcohol dependence.
In this study, 114 out of 170 patients (67%) with alcohol dependence syndrome had sexual dysfunctions, and the most common sexual dysfunction was lack or loss of sexual desire (45%), followed by failure of genital response (40%), frequency dissatisfaction (35%) and premature ejaculation (31%).
Several studies have shown a significant relationship between alcohol dependence and sexual dysfunction. A study done by Benegal and Arackal found that 72% of alcohol-dependent men had one or more sexual dysfunctions, the most common being premature ejaculation followed by low sexual desire and erectile dysfunction. 28
Vijayasenan found that 71% of the patients with alcohol dependence suffered from one or another sexual dysfunction, and the common dysfunctions noted were diminished sexual desire (58%), ejaculatory incompetence (22%), erectile dysfunction (16%) and premature ejaculation (4%). 27
In another study done by Mandell et al, it was found that during heavy drinking, 84.4% of patients had experienced at least one kind of sexual dysfunction; the most common was erectile dysfunction (59%), followed by premature ejaculation (48%). 28
A study conducted by Fahrner reported that approximately 75% of patients who had alcohol addiction had sexual dysfunctions in the form of erectile dysfunction, loss of libido and premature or delayed ejaculation. 29
A study of young married alcohol dependence patients done by Jensen found that 63% of the men reported sexual dysfunction, mainly erectile dysfunction and libido disorders. 30
A case-control study done by Aswal et al in 2012 showed a significantly higher prevalence of sexual disorders among alcohol dependents in comparison to a healthy matched control group. The most common diagnosis was erectile dysfunction (28%), followed by loss of libido (26%), delayed ejaculation (10%), excessive libido (8%) and premature ejaculation (4%). 26
However, a study done by Kisore et al has shown a very low prevalence of sexual dysfunction (30.8%) amongst patients with alcohol dependence. 31
Beutel et al suggested that the wide range of prevalence rate estimates is likely due to different definitions and criteria of sexual dysfunctions. 32
In this study, the ADS score was positively correlated to the ASEX score, and this correlation was statistically significant. It was also seen that the prevalence of sexual dysfunction increased with the severity of alcohol dependence. However, this was not statistically significant. Also, there was no statistically significant relationship between the severity of alcohol dependence and the type of sexual dysfunction.
It appears that the severity of alcohol dependence is associated with sexual dysfunction. A study done by Gümüş et al has shown that chronic heavy use of alcohol significantly alters the gonadal hormones, causing sexual dysfunction. 33 This study highlights the need to identify, assess and treat male sexual dysfunctions in patients with alcohol dependence for a better quality of life.
Conclusion
A majority of patients were more than 30 years old, educated up to the primary level, employed, married and belonging to lower socioeconomic status.
The prevalence of sexual dysfunction was 67.06%. A majority of the sample studied had one or more sexual dysfunctions.
Loss or lack of sexual desire was the most common sexual dysfunction at 45.88%, followed by failure of genital response (erectile dysfunction) at 40.58%, frequency dissatisfaction at 34.71% and premature ejaculation at 31.76%.
The ADS score positively correlated with the ASEX score, and this correlation was statistically significant.
Though the prevalence of sexual dysfunction increased with the severity of alcohol dependence, this was not statistically significant.
Recommendations
A strong physician–patient relationship and thorough history-taking may help to identify patients at risk for the adverse psychological effects of sexual dysfunction.
There is a need for clinicians to routinely assess the sexual dysfunctions in their patients with alcohol dependence, as well as for sexual medicine specialists to consider the effects of heavy alcohol use on sexual functioning so that appropriate treatment can be initiated.
Improving the training of undergraduate medical students in sexuality related issues is required.
Providing sex education to the general population using media and merging sexual health care with primary care can play a significant role in addressing the increasing sexual health morbidity.
Evidence that alcohol-induced sexual dysfunction may be reversible with the cessation for alcohol can be used in motivational counselling of heavy drinkers to provide impetus for change.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
The research conducted in this study was in accordance with ethical standards and guidelines. The approval of ethics committee and scientific committee of K. J. Somaiya Medical College and Hospital, Mumbai, was taken prior to the start of the study.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent
Prior to participating in the study, all participants were provided with detailed information about the research objectives, procedures, potential risks and benefits. Informed consent was obtained from each participant. Participants were presented with the form, which outlined the study’s purpose and the voluntary nature of their participation. They were given the opportunity to ask questions and seek clarification on any aspects of the study. Participants were assured that their personal information would be kept confidential and their anonymity would be maintained. Only after obtaining written informed consent from each participant were data collection procedures initiated.