
Abstract
Background:
Many patients and health literature, in general, allege that psychotropic agents cause sexual side effects.
Objective:
We intended to investigate this issue in a Nepalese clinical setting by estimating the prevalence of psychosexual problems among remitted psychiatric outpatients (on psychotropic medication) and by comparing it with that of a nonpsychiatric patient group (on nonpsychotropic medication).
Methodology:
In this hospital-based cross-sectional comparison study with purposive sampling, we collected the responses to a self-response questionnaire called “Arizona Sexual Experience Scale” from a total of 400 subjects: 100 male and 100 female consecutive consenting remitted psychiatric and dermatological outpatients, each with sex and marital status matching. We recorded pertinent information in the proforma and screened psychosexual problems with the Arizona Sexual Experience Scale after informed written consent. The problems in psychiatric and dermatological groups were compared.
Results:
We have more subjects of reproductive ages in both the psychiatric and dermatological groups. Depression, anxiety, and bipolar affective disorder were the most common diagnoses in the psychiatric patients, whereas eczema, fungal, immunologic, and allergic skin lesions/diseases were common in the dermatological patients. Both groups had comparable sexual dysfunction rates, both by overall and the criteria of ≥3 items with scores ≥4, whereas dermatological patients had more problems with criteria of ≥1 item with a score ≥5.
Conclusions:
Psychosexual dysfunction was more or less similar in frequency among both the psychiatric patients on psychotropic medication and dermatological patients on topical agents.
Keywords
Introduction
Sexual complaints are one of the symptoms of mental illness,1, 2 though many patients and their family members do not readily express it in the first instance. Psychotropic medications are, in general, alleged to cause a variety of adverse sexual effects.3–5 In many psychiatric disorders, people may have different residual symptoms including sexual complaints even after the improvement of core symptoms.2, 6 Many factors including cultural, societal, educational, etc, play a role in the manifestation, expression, and help seeking for these psychosexual problems. 7 In Nepal, many people hesitate to take psychiatric help even for psychiatric illness, and a few people may express the underlying sexual symptoms. 8 We lack data regarding what extent the clients have psychosexual dysfunctions in clinical practice. It would have been much of use in highlighting this aspect of health if we had data.
This hospital-based comparative study targeted to measure the prevalence of psychosexual problems or sexual dysfunction (SD) among remitted psychiatric patients with the application of a standard and valid instrument called the “Arizona Sexual Experience Scale” (ASEX) 9 and to compare it with sexual problems among nonpsychiatric patients (dermatological patients not requiring psychotropic and systemic medication and with significantly improved skin lesions). This would give an idea about to what extent the psychotropic agents in general (likely) cause sexual symptoms in practical sense. Overarching the project will be to intensively look into the effect of a particular factor and a particular psychotropic medication for psychosexual complaints.
Materials and Methods
Design
This is a cross-sectional study conducted in a hospital (B. P. Koirala Institute of Health Sciences, BPKIHS) among remitted psychiatric outpatients and improved dermatological outpatients (both in nonacute phase).
Subjects
We enrolled 400 subjects which consisted of 200 psychiatric patients (100 males and 100 females) who had remitted from acute phase and with continued psychotropic medications, and as the comparison group, 200 dermatological patients (100 males and 100 females) who were on some topical (not systemic) medication and with significantly improved skin lesions and no past history of diagnosed mental illness. The subjects were consecutively enrolled as they came in the contact of the investigating team for the service during 1 year of study period, giving informed written consent.
Operational definition of “remitted psychiatric patients”: Those psychiatric patients who have been asymptomatic (by history and in clinical assessment) and functional for at least 2 months during the study.
We included all categories of psychiatric disorders if they were asymptomatic and functional for at least 2 months, and were not physically unstable. For dermatological patients, the subjects not on any systemic medication (but only on some topical and/or symptomatic medication) and who had significantly improved in skin lesions were enrolled.
Subject Enrolment
Research staff/enumerator explained about the study to a subject. After the consent, they collected sociodemographic data using semi-structured proforma. They also collected the responses from the subjects about psychosexual dysfunction using a self-response questionnaire known as ”ASEX.” 9 The questions were self-responded by literate and were read by an enumerator or research staff to illiterate and needy subjects. The responses were analyzed by following the instructions of the instrument.
Arizona Sexual Experience Scale (ASEX)
ASEX, a tool developed by the Department of Psychiatry and Psychology, University of Arizona and the Department of Psychiatry and Behavioral Sciences, Stanford University, measures by rating 5 core elements of sexual function (sexual drive, arousal, penile erection/vaginal lubrication, ability to reach orgasm, and satisfaction from orgasm) on a 6-point Likert scale ranging from 1 (hyperfunction) to 6 (hypofunction). The scale has two versions, each for males and females, with a difference in question 3 that references penile erection versus vaginal lubrication. The scale is useful in clinical trials to evaluate potential dysfunction caused by medications. This tool has shown an excellent internal consistency, reliability, and validity also for psychiatric patients.4, 10 A total score of more than 18 or a score of 5 (very difficult) or greater on any 1 item on the ASEX is taken as clinical SD. 9 This self-rated scale application takes about 5 to 10 min. The scale was translated to and back translated from the Nepali language. The Nepali version was pretested among 40 subjects who were excluded from the study. It may be completed/rated by the interviewer.
Data Processing
Regular meetings and interactions were held to sort out difficulties. The coded proformas were collected at the end of a week by research staffs. On receiving proformas, the information was entered into a computer and data were analyzed using the “statistical package for social sciences” version 17 (SPSS-17). Its output provided the data on the prevalence of sexual problems and on the comparison of the sexual problems between remitted psychiatric patients on psychotropic medication and healed nonpsychiatric patients on topical medication for skin lesions. The prevalence rate was calculated as the mean, and the comparison of prevalence of psychosexual problems between remitted patients on psychotropic and nonpsychotropic medications was done with statistical tests such as chi-square test, P value, etc.
Ethical Consideration
This study received the approval of the “Ethical Review Board” of BPKIHS (IERB Ref. Acd 76 and IRC Ref. Acd 165/067/068). Informed written consent was taken from all the subjects. Strict confidentiality of information was maintained.
Results
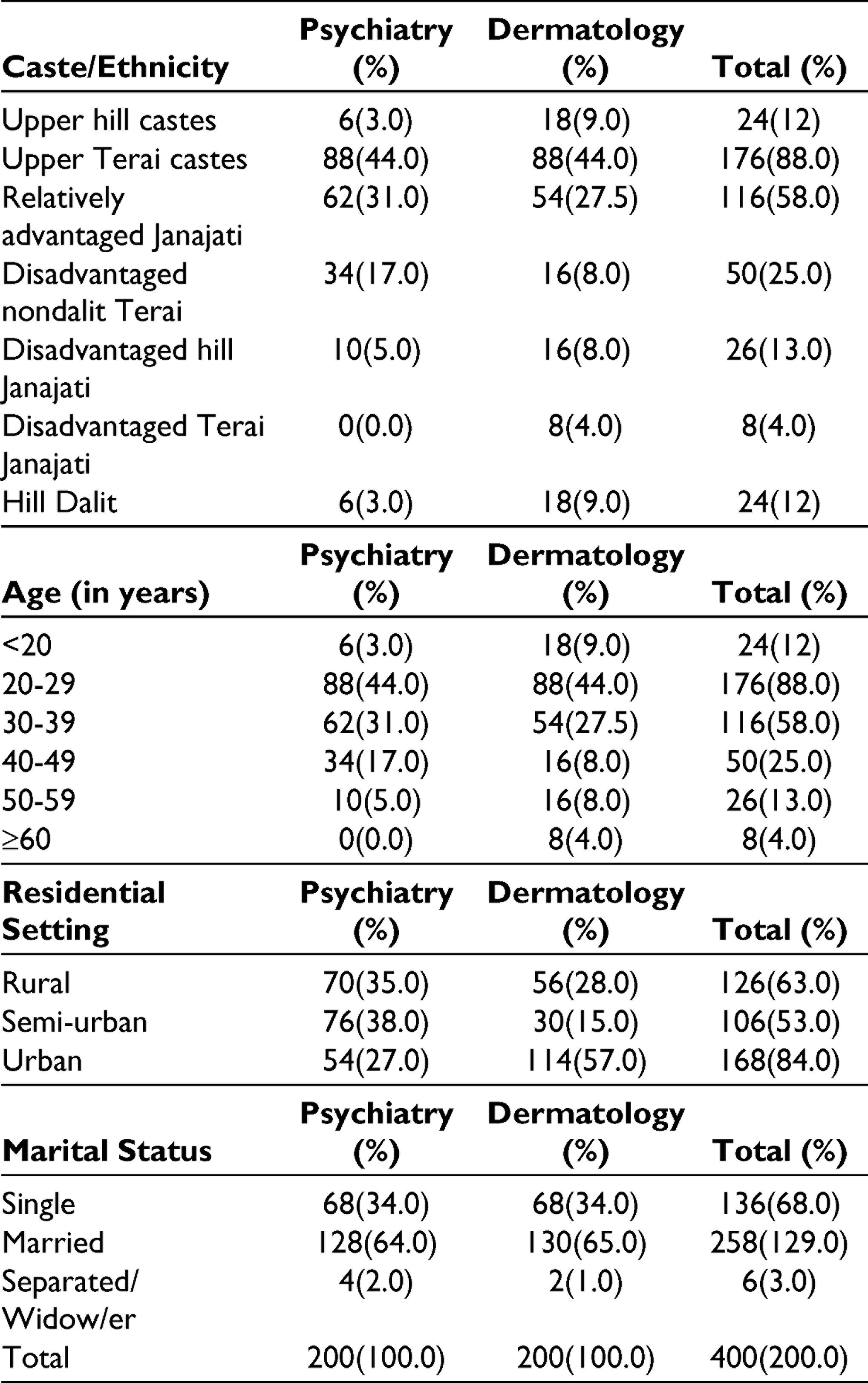
Among the total enrolled 400 subjects, 200 were from psychiatry and dermatology out patient department (OPD)each, with 100 males and females each in both the departments.
Both the departments have disadvantaged hill Janajatis (eg, Rai, Tamang, Limbu, etc) and upper hill castes (eg, Brahmins, Chhetri, etc) as the most common caste/ethnicity groups; P = .118 (Not significant).
The average age was 32.235±4.0620 SD and 31.54±11.4429 SD (16 and 16 minimum, 60 and 65 maximum) years in psychiatry and in dermatology OPD, respectively. The largest proportion of the patients were of the age groups (20-29) and (30-39) years. Dermatology patients were more distributed in various age groups than psychiatry; P = .000 (Significant).
They came from different residential settings; more semi-urban and rural in psychiatry and urban in dermatology groups; P < .001 (Significant).
From Table 1, we can see that the majority of these clients are married in both the groups (matched); P = .706 (Not significant).
Caste/Ethnicity, Age, Residential Settings, and Marital Status
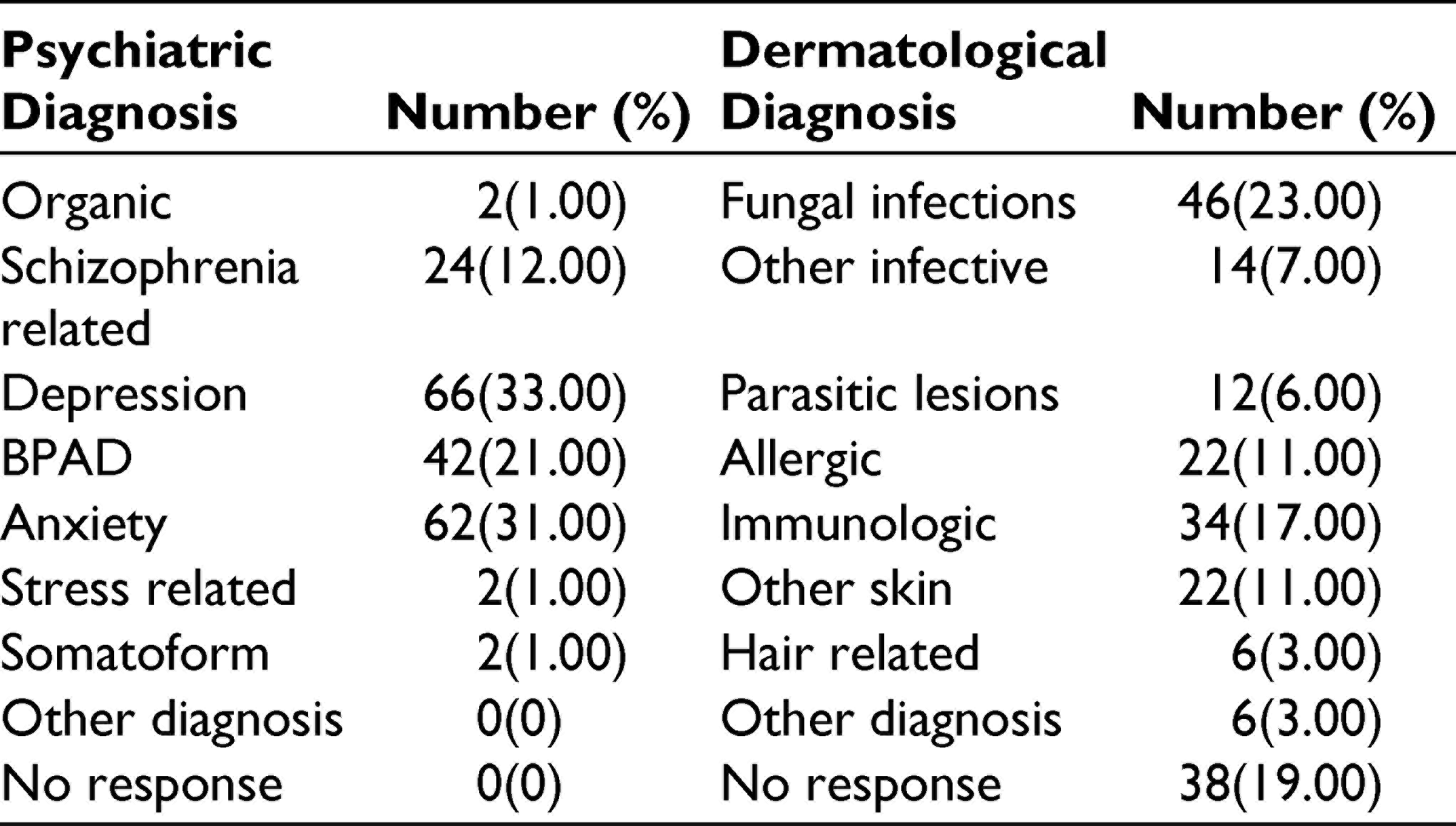
In psychiatry OPD, the common mental disorders were depression, anxiety disorders, and bipolar affective disorder (BPAD). In dermatology OPD, the common skin disorders were fungal and immunologic disorders (Table 2).
Psychiatric and Dermatological Diagnosis in Psychiatry and Dermatology Outpatient Clinic
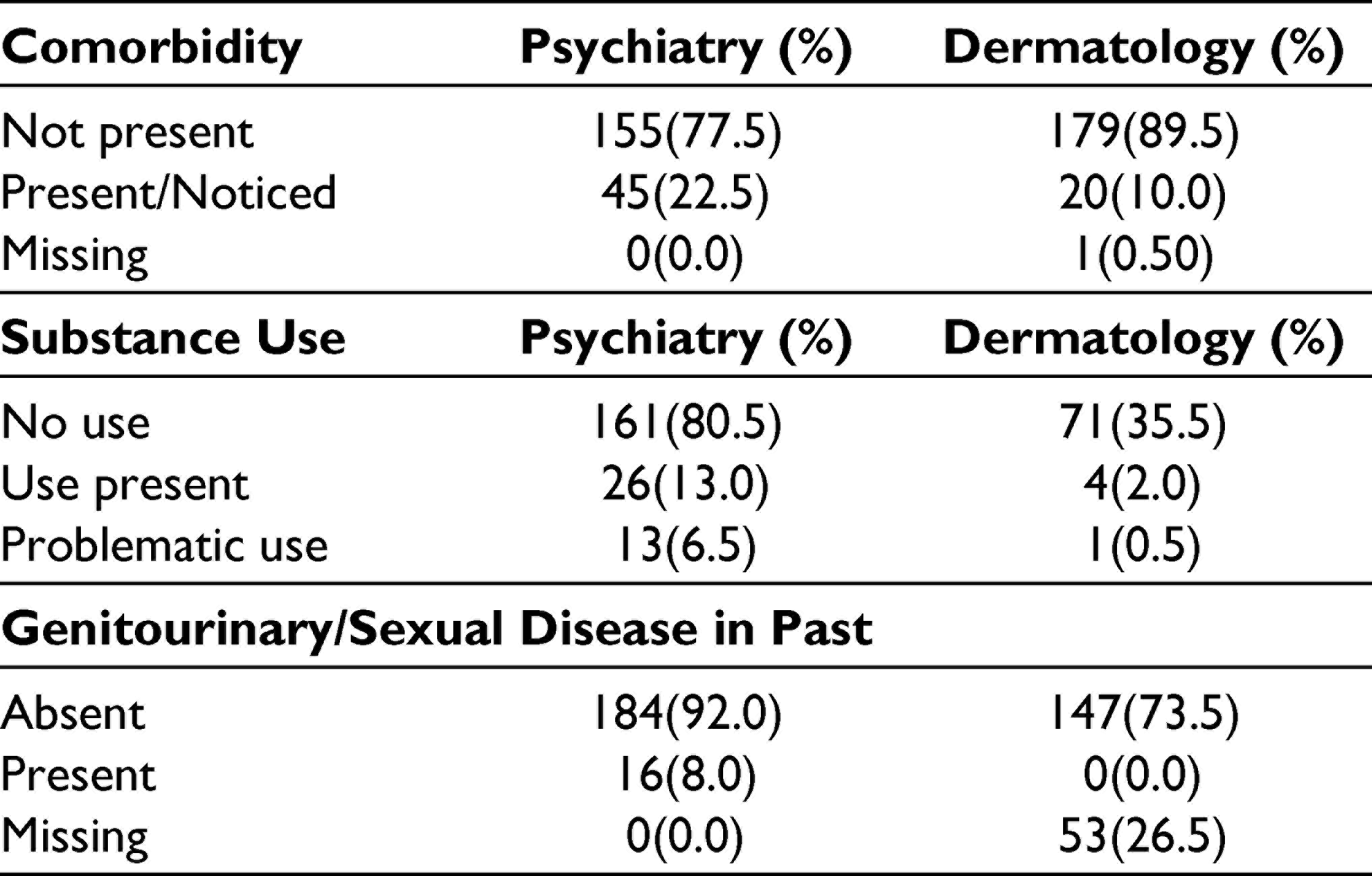
Comorbidity was reported more among psychiatric patients; P = .001 (S).
Psychiatric patients reported substance use more and dermatology patients did not respond more about genitourinary/sexual diseases. P < .001 for both variables (Table 3).
Comorbidity Status, Substance Use, and Genitourinary Problem
None of the ASEX questionnaire item is statistically different in the 2 diagnostic groups on respective medications on mean scores, though there were more subjects in the psychiatry group on sex drive, sexual arousal, and orgasm items than the dermatology group with the scores ≥4 (Table 4).
ASEX Items

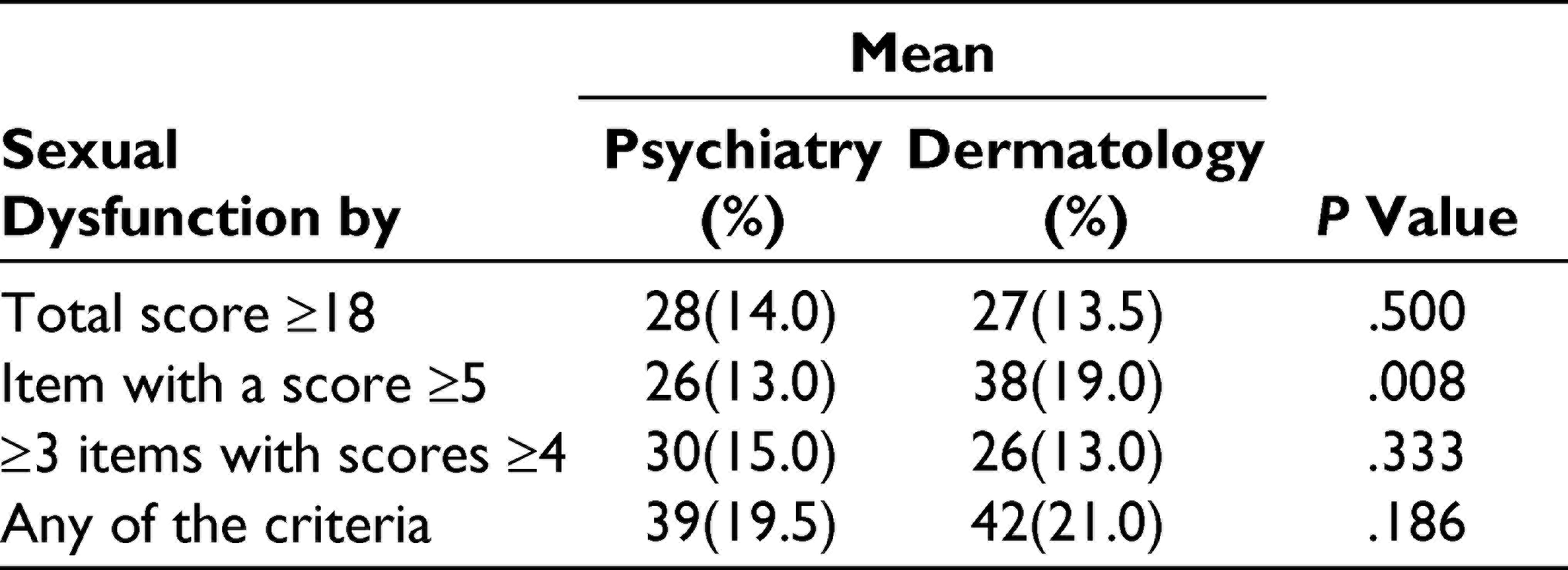
There was a statistically significant difference between remitted psychiatric and dermatology patients on respective medications with regard to SD by the criteria of at least 1 item with a score ≥5 (P = .008, S), whereas no difference was noticed by the criteria of an overall score of ≥18 and ≥3 items with scores ≥4 and by any of the 3 criteria (P = .500, .333, .186, all NS; Table 5).
Sexual Dysfunction by the ASEX Questionnaire
Discussion
Sexual disturbances are symptoms in many psychiatric disorders, eg, decreased libido/desire in depression, premature ejaculation or erectile dysfunction in anxiety, increased libido, and disinhibited behavior in mania and loss of sexual interest in schizophrenia. Primary sexual disorders have a variety of symptom profiles. Not only during acute phase but also in nonacute phase, sexual disturbances may occur as residual symptoms.1, 2, 6 Psychotropic medications are, in general, alleged for sexual problems, eg, serotonin reuptake inhibitors,3, 4 and antipsychotics, especially prolactin-raising ones, are reported with higher rates of sexual problems.3, 5
Many factors including cultural, societal, and educational factors play a role in sexual health/problems, their manifestation, expression, and help seeking for them. 7 The prevalence of SD exhibits a great range of rates both in community and clinical settings. Laumann et al reported its prevalence to be 31% in males and 43% in females, which are strikingly high rates of SD, and also described physical and emotional health as important predictors of sexual health in the United States. 11 Perlman et al reported the prevalence of SD to be 17% in psychiatric inpatients, and depression, antidepressant use, and cardiopulmonary conditions as its important predictors. 12 A study of psychiatric outpatients in Calabar reported it with a great range of 16% to 66%. 13 Another psychiatric outpatient study among nonacute psychotic and affective disorder patients compared with healthy controls found a significant difference in these 3 groups with the prevalence of 49%, 36%, and 13%, respectively. 6 A study conducted in Mumbai, India with the ASEX in psychiatry outpatients with some psychosexual complaints reported premature ejaculation in 55%, erectile dysfunction in 27%, and both in 18%. 7
In this study, the mean scores of the 5 ASEX items were slightly higher in our psychiatric group than the dermatology group, with both groups lying in between 2 and 3, ie, normal function. The differences in mean scores were not statistically significant in any items. The clinical SD was more among dermatology patients than psychiatric patients by the criteria of the total ASEX score ≥18 and by ≥ 1 item with a score ≥5, latter of which was statistically significant. Dermatology patients also had higher overall prevalence by any of the 3 criteria (21% versus 19.5%), which was, however, not statistically different. We found higher prevalence of clinical SD among psychiatric patients by the criteria of ≥3 items with scores ≥4, which was, however, not statistically significant.
This study showed the prevalence of SD to be 13% to 20% among remitted psychiatric patients that is most likely attributable to the use of psychotropic medication. This is consistent with the observation that in practical sense, even if SDs occur, they are mostly mild and the patients may not appreciate as significant and not report and are transient. 5 Our report is based on the responses of subjects who were asymptomatic and remitted. The rate of prevalence among our psychiatric outpatients is relatively lower, although it falls in a great range of the prevalence reported in similar studies abroad.5, 6, 11–13
With this finding, we understand that while attaining remission in therapeutic doses, the therapeutic effect of psychotropics outweighs side effects, including sexual disturbances. We can safely infer that clients benefit with the judicious use of psychotropic agents. However, it is noteworthy that the effects differ with the agents than the psychotropic group in general. Owing to inherent drawbacks and limitations of this study, further investigation is warranted for its confirmation and comprehensive understanding.
Findings of one sociocultural background may not be applicable to other, especially for such problems as SD. Nepalese patients hesitate to visit psychiatric clinics and even fewer people express the underlying sexual symptoms. 8 In this pretext, even less information is available regarding the sexual problems of mentally ill people. Many psychiatric patients complain about the sexual side effects of psychotropic medications as they hear from others or they generally think so, although the prescribing doctor largely appreciates their benefits to the mental conditions. This study, hence, served into this issue in our setup showing that sexual problems are comparable among patients taking psychotropic medicine and those on dermatological topical medicine.
Our SD rate in dermatology outpatients (13%-21%) was less in comparison to a similar Indian study. 14 As this study was carried out among heterogeneous groups of subjects, in terms of many respects like disorders, duration of disorder remission, medications, and other variables, this is a kind of preliminary study in this direction and is expected to open avenues for further in-depth, ie, genetic variability 15 and psychotropic medicine-specific studies. 16
As we mean to determine sexual disturbances which most likely reflect the extent of occurrence as the effect of psychotropic medication and to compare with a control, we chose dermatology outpatients with significant improvement in their dermatological lesions but still continuing with topical medication and at most other symptomatic medicine (but not on any psychotropic/systemic agent). By choosing patients on topical/symptomatic medication and with similar attributes as far as possible, we mean to minimize confounders but still owing to the nature of study and topic, there are some limitations on part of the subject selection. For example, the skin lesions, the resulting disfigurement, and the varying duration of remission of illness might have at least some bearing on sexual health. The Nepalese society is hesitant to talk about sexual issues. 8 We had missing responses on some variables, especially from dermatology patients, mainly on substance use, past genitourinary problems, and other comorbid conditions. The information that was collected from the subjects in this study, is more available among psychiatric patients in all the variables. It should be paid due consideration in later studies.
Our diagnostic groups—psychiatric and dermatological—did match in some variables, eg, ethnicity, marital status, etc, latter of which was an important determinant for sexual problems. There were differences in some demographic variables, eg, in age especially because the psychiatry group did not have subjects above 60 years of age (similar distribution, minimum, maximum, and average age, most common age groups) and in the residential settings most likely because of the nature of diagnosis itself (more psychiatric patients from semi-urban and rural, and more dermatological patients from city areas). dermatological outpatients were more distributed in various age groups. The distributions of ethnicity, age, and residential settings of psychiatric patients were consistent with other previous studies from the department of psychiatry. 17
The diagnostic profile among psychiatric patients with preponderance of depression, anxiety, and BPAD is consistent with that found in a previous study 17 and the dermatological diagnostic profile with observations made in the dermatology OPD of a teaching hospital in Kathmandu. 18 The dermatological diagnostic profile differs in different setups. 19 Keeping with the psychiatric diagnostic profile in this study, the most commonly prescribed psychotropic medications in psychiatric OPD of BPKIHS were: serotonin reuptake inhibitors (females 67, males 47), other antidepressants (females 21, males 18), lithium (females 14, males 18), antiepileptics (females 2, males 12), prolactin-raising antipsychotics (females 6, males 22), prolactin-sparing antipsychotics (females 6, males 2), hypnotics/sedatives (females 4, males 5), trihexyphenidyl (both 4), thyroid supplement (female 1, male 1), nutritional/vitamin (female 1, male 2), and other medications (both 10).
It would be useful to have information about disorder-specific sexual disturbance both for psychiatric and dermatological illnesses. Not only in mental illness but also in various skin diseases, sexual health is reported to be significantly disturbed.14, 18, 20, 21
Conclusions
Psychosexual problems were reported both by remitted psychiatric (13%-20%) and dermatology patients (13%-21%), which are comparable in both the groups. Overall, remitted psychiatric outpatients on medications have comparable SD with respect to dermatological outpatients on some topical medications.
Footnotes
Acknowledgements
Professor Dr P. M. Shyangwa, Department of Psychiatry and Professor Dr S. Agrawal, Department of Dermatology and Venereology, Mr D. D. Baral and Mr S. Bhattarai- for assistance in statistical analysis and Dr Goma Pun, Department colleagues, students and staff, BPKIHS.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received funding for the research from BPKIHS research.