
Abstract
Sexual functioning is a bio-psycho-social process. Sexuality is at the core of social interactions, couple relationships, intimacy, and reproduction. General medical conditions are commonly associated with sexual problems. Erectile dysfunction (ED), premature ejaculation, hypoactive sexual desire disorder, and dyspareunia are commonly associated with general medical illness. ED precedes the development of chronic coronary artery disease by a minimum of 3 years. Massachusetts Male Aging Study concluded that both type 1 and type 2 diabetics are at 3 times greater risk of ED. Sexual disorders in females involve aspects of desire, arousal, and orgasm. Prevalence of female sexual dysfunction is more common in diabetes which is mainly linked to psychosocial factors. Hypothyroidism, hyperthyroidism, hypogonadism, and hyperprolactinemia are commonly associated with ED. Various medications are also associated with sexual problems.
Sexuality is at the core of social interactions, couple relationships, intimacy, and reproduction. In their classic Textbook of Sexual Medicine, Masters and Johnsons have defined sexual medicine as “that branch of medicine that focuses on the evaluation and treatment of sexual disorders, which have a high prevalence rate.” Sexual functioning is a bio-psycho-social process with involvement of multiple systems of the body. It is coordinated by the vascular, endocrine, and nervous systems with almost each and every system of the body having direct or indirect influence over the sexual functioning of an individual. 1 A misdiagnosis can lead to impaired sexual functioning and quality of life. Hence, a multidisciplinary approach in liaison with other specialties is the key to management of problems related to sexual health.
The Diagnostic and Statistical Manual 5th edition (DSM-5) doesn’t consider a sexual disorder due to a general medical condition, as a psychiatric diagnosis. However, there are many incidences where a general medical illness may interfere with sexual functioning of an individual. For example, a newly diagnosed case of diabetes may develop erectile dysfunction (ED) during the course of illness. Such a patient would require expert psychiatric opinion for management of the problem. Various medical disorders and their treatment, existing sexual beliefs, and other sociocultural factors interact in a complex manner, leading to sexual health issues.
Ageing, medication use, and presence of a single comorbidity increased the risk of arousal disorders (in women) and erection (in men) by 1.5 times. Population-based surveys have concluded that ED, premature ejaculation (PME), hypoactive sexual desire disorder, and dyspareunia are commonly associated with general medical conditions. Around 60% of diabetic men over 50 years of age have some associated erection problems. Diabetic men develop ED 10 to 15 years earlier as compared to nondiabetics.
Psychiatry and Cardiology
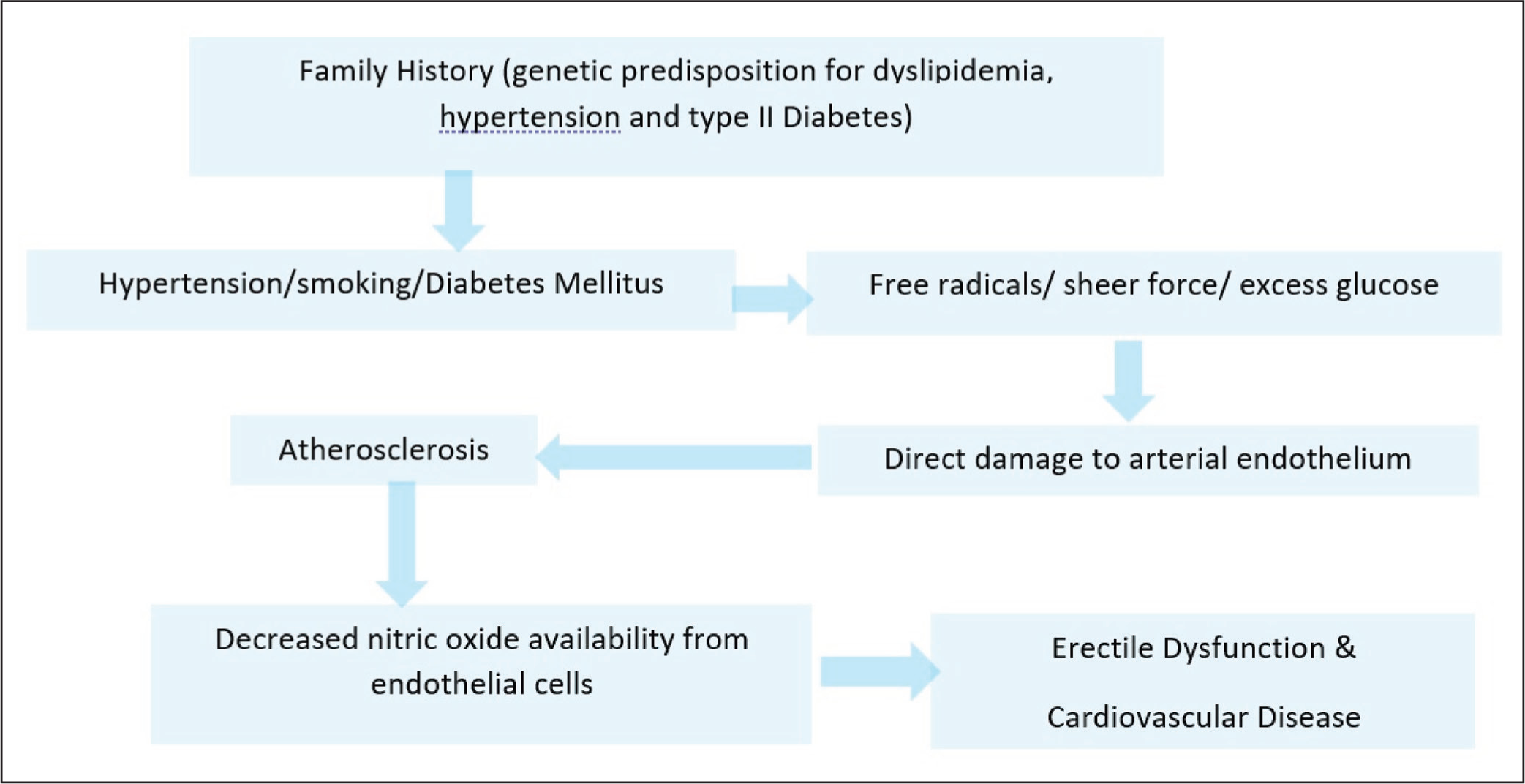
Endothelial injury is the common link between cardiovascular diseases (CVD) and ED. Atherosclerosis affects smaller penile arteries (1-2 mm diameter) much earlier when compared to coronary arteries (3-4 mm diameter). 2 Montorsi and colleagues have concluded that ED precedes the development of chronic CAD by a minimum of 3 years. Mobley has demonstrated that ED can be considered as a future marker of CVS morbidity. 3 Common etiopathogenesis of CVD and ED has been elaborated in Figure 1.
Common Etiopathogenesis of Cardiovascular Disorders (CVD) and Erectile Dysfunction (ED).
Shi and colleagues 4 concluded that among males less than 70 years of age with acute or chronic CAD, 58% presented with decreased sexual frequency, 33.8% with normal sexual life, whereas 8.1% had not resumed their sexual lives. An individual presenting with ED goes on to develop CAD over an average time interval of 33 months.
Sexual disorders in females involves aspects of desire, arousal, and orgasm. Clitoral and vaginal vascular insufficiency syndromes are directly related to the atherosclerotic process and are associated with a decreased genital blood flow in the hypogastric and pudendal arteries.
When followed up for over a period of 6 months, males with CAD developed various sexual problems like difficulty sustaining an erection after penetration in 84%, reduced sexual desire in 76%, difficulty reaching orgasm in 62%, and difficulty having an erection for penetration in 84% cases. Females with CAD developed arousal problems in 87%, decreased lubrication of vagina in 84%, difficulty reaching orgasm in 62%, sexual pain in 50%, and reduced sexual activity in 29% of cases.
The prevalence of ED in individuals with hypertension is approximately double than that in normotensive population. Duration and severity of hypertension, additional CVD risk factors, and aging increase the probability of developing ED. 5 Systolic blood pressure greater than 140 mm Hg doubles the prevalence of ED. Narrowing of any part of iliac-pudendal- penile arterial system could lead to ED. 6
Heart failure is associated with higher prevalence of ED. Among heart failure patients, 60% to 89% may develop ED to some extent. 7 Heart failure is associated with reduced cardiac output and decreased physical activity. Associated medication side effects and endothelial dysfunction can affect any of the phases of sexual response cycle leading to sexual dysfunction (SD).
Myocardial infarction (MI) is associated with significant psychosexual morbidity. Even during the cardiac rehabilitation at 1 year post MI, a meagre 41% of patients and 31% of their partners had been counselled regarding how to resume sexual activity. 8 Among cardiovascular (CVS) drugs, losartan and valsartan have been conclusively proven to have a positive effect on sexual functioning. Nebivolol has a positive effect on erectile function. Beta adrenergic receptor blockers carvedilol and atenolol and thiazide diuretic chlorthalidone have a negative effect on erectile function. Calcium channel antagonists nifedipine and diltiazem and angiotensin-converting enzyme inhibitor lisinopril don’t interfere with sexual functioning.
Exercise ability can be equated to sexual activity while assessing an individual’s CVS risk. Sexual activity is equivalent to (a) briskly climbing 2 flight of stairs in 10 s or (b) walking 1 mile on flat surface in 20 min. Any therapy for ED should be started only after assessing for exercise tolerance. Reassurance and exercise are helpful in disorders of sexual desire and arousal. PDE-5 inhibitors (when not on nitrates) can help patients with ED. Vardenafil has to be avoided with class-IA antiarrhythmics.
Apomorphine (D1/D2 agonist) can be tried when the patient is on nitrates.
Psychiatry and Endocrinology
Massachusetts Male Aging Study concluded that both type 1 and type 2 diabetics are at 3 times greater risk of ED when compared to nondiabetics. 9 Pathophysiology of ED in diabetics includes endothelial dysfunction, microangiopathy, and macroangiopathy leading to diabetic vasculopathy. ED due to diabetes is multifactorial in origin with vascular, neurological, metabolic, hormonal, and psychological factors involved.
Atherosclerosis leads to macrovascular disease-limiting blood flow in vascular beds. Endothelial dysfunction and decreased production of nitric oxide leads to impaired relaxation of smooth muscles. Microvascular complications occur due to ischemia of distal vascular bed and neuropathic changes. Defective axonal transport and impaired nerve conduction leads to irreversible ED. 10 Sensory impulses from penis to spinal and supraspinal centers get impaired associated with parasympathetic inactivity. Reversal of symptoms of ED even after strict glycemic control is not promising. Phosphodiesterase (PDE-5) inhibitors and associated psychosocial factors have to be dealt with. Intracavernosal injections of prostaglandin E1 (PGE1) can be tried in resistant cases. Prevalence of female SD is more common in diabetes which is mainly linked to psychosocial factors. For orgasmic difficulty and ejaculatory problems, vibrostimulation, yohimbine, bupropion, buspirone, and cyproheptadine can be tried.
The human neuroendocrine system has a strong influence on the sexual functioning of an individual. It includes the hypothalamic pituitary adrenal (HPA) axis, hypothalamic pituitary thyroid axis, hypothalamic pituitary gonadal (HPG) axis, and hypothalamic-neurohypophysial system. The HPA axis alteration mediates “hypothalamic” amenorrhea of stress and the hypogonadism of Cushing’s syndrome. Thyroid hormones influence the ejaculatory process and the amount of circulating testosterone levels. Circulating sex hormone levels is influenced by both hypo- and hyperthyroidism.
Hypothyroidism, hyperthyroidism, hypogonadism, and hyperprolactinemia are commonly associated with ED. A total of 2% to 33% of men with ED may have associated androgen deficiency. The prevalence of SD in males with hypothyroidism varies from 59% to 63% whereas in males with hyperthyroidism it varies from 48% to 77%. Hypothyroidism in males is associated with impaired libido, erectile and ejaculatory dysfunction (delayed ejaculation) whereas hyperthyroidism is associated with erectile and ejaculatory dysfunction (PME) or impaired libido. In females, prevalence of SD varies from 22% to 46% in hypothyroidism and 44% to 60% in hyperthyroidism. Both hypothyroidism and hyperthyroidism in females can lead to decreased libido, impaired desire, arousal/lubrication, orgasm, satisfaction, and pain during intercourse. 11
Any HPG axis alteration can lead to hypogonadism which can be primary or secondary. It can be treated effectively with testosterone replacement therapy (TRT). TRT has a 2 pronged effects: improving sex drive on one hand and enhancing phosphodiesterase (PDE-5) inhibitor effectiveness on the other.
The level of testosterone in blood is inversely related to time required for ejaculation. Higher testosterone levels can lead to PME and vice versa. 12 Prolactin level is considered as a proxy indicator for serotonin activity. Higher levels of prolactin inhibit ejaculation. During orgasm and climax, dopamine peaks and prolactin is suppressed. After orgasm dopamine decreases and prolactin peaks, prolactin is partially responsible for the refractory period seen in males after orgasm. 13 Both microprolactinomas and macroprolactinomas may be associated with either reduced sexual desire or ED. Hyperprolactinemia in women can lead to reduced arousal, lubrication, orgasm, and satisfaction. Increase in prolactin (both short term and long term) can alter sexual functioning in both men and women through receptors present in the brain.
Psychiatry and Neurology
Dementia can affect the existing relationships because of its impact on the psychosocial functioning of an individual. This can be due to increased dependence, caregiver burden, financial problems, and social isolation. There may be a decline in intimacy with age, loss of self-concept, and disappointment with oneself or the partner. During old age, people prefer nonsexual forms of intimacy like cuddling or kissing. 14 With advancing age, the act of sexual intercourse may get affected by vision or hearing disturbances and delayed arousal or lack of sexual desire. Dementia is associated with ED (40%-55%) in men and decreased desire (~60%) in women. Treatment options for dementia include hormone replacement, PDE-5 inhibitors, and vaginal creams. Sexual assistive devices can be helpful. Intimacy is important in these individuals to enjoy sexual activity. Avoiding understimulation and activity scheduling is important. The patient should be given comfortable clothing and soft toys as appropriate. Pharmacological treatment depends upon the presenting symptoms and may involve use of antidepressants (selective serotonin reuptake inhibitors [SSRIs], mirtazapine, or trazodone), antipsychotics (haloperidol, risperidone, and quetiapine), anticonvulsants (benzodiazepines, carbamazepine, valproate), and anti-dementia drugs like donepezil, galantamine, or memantine. Antiandrogens may be required for hypersexual behavior.
Parkinson’s disease (PD) is a neurodegenerative disorder characterized by tremors, bradykinesia and rigidity, and loss of fine motor skills. 15 These can lead to one’s inability to participate in sexual activity. Moreover, tremors increase during sexual arousal making the act more difficult. It can have a negative impact and affect an individual’s sexuality. Symptoms increase during night due to preferential daytime dosing of drugs easing day-to-day activities. Associated anxiety, depression, and cognitive symptoms associated with autonomic disturbances involving bowel and bladder contribute to sexual problems. Decreased dopamine levels in the brains contribute to decreased libido, anhedonia, and diminished sexual motivation. Poor premorbid sexual functioning, associated illnesses, medications, and advanced stage of PD contribute to SD. 16 Women with PD report difficulties associated with arousal (87.5%), orgasm (75%), low sexual desire (46.9%), and sexual dissatisfaction (37.5%). 16
Females also report vaginal tightness, painful sexual contact, problems with lubrication, and involuntary urination. Men with PD develop ED (68.4%), PME (40.6%), sexual dissatisfaction (65.1%), and difficulty reaching orgasm (39.5%). 16 Men also suffer from low sexual desire and ejaculatory problems. Age, severity of the disease, and associated depression are major determinants affecting sexual satisfaction. These patients may also present at times with hypersexual behavior.
Management should focus on improving motor symptoms, sialorrhea, and orthostatic hypotension (OH). Ephedrine may be helpful in OH. Certain medications like sildenafil, apomorphine, and PGE1 are helpful in ED. Vaginal lubricants and topical creams may be useful. Deep brain stimulation (DBS) of the subthalamic nucleus for ED is one of the emerging options. Apart from treatment of symptoms of PD, sexual dysfunctioning can be managed by use of sildenafil, apomorphine, and PGE1 for ED, vaginal lubricants, and topical creams. DBS of subthalamic nucleus is sometimes helpful in ED.
Cerebrovascular diseases include stroke which can have a significant sexual morbidity. A biopsychosocial model best explains the SD associated with stroke. 17 Sexual activity may be impacted by muscular weakness, paraesthesias, incontinence, immobility, fatigue, and pain. Post stroke depression and cognitive symptoms add to the sexual morbidity. Patients may also avoid sexual activity for fear of precipitating another stroke. Lesions in the nondominant hemisphere are more likely to be associated with decreased desire, decreased libido, and decreased frequency of intercourse. Lesions in the right cerebellum are linked to ejaculation problems. Depending upon the severity of stroke physiotherapy, rehabilitative aids, speech therapy, and management of incontinence may be required. Cognitive enhancers can be useful. Sildenafil for ED, baclofen, and tizanidine for spasticity are helpful.
Epilepsy is often accompanied by SD as a result of complex interaction between neurological, endocrinal, and psychosocial factors. Approximately, one-half of men and women with epilepsy suffer from SD. 18 Epileptiform discharges may disrupt connections in the limbic system which can have a negative impact on sexual behavior. There may be associated fear of provoking a seizure during sexual activity, which is accompanied by hyperventilation. Temporal lobe epilepsy can be associated with ictal orgasms, sexual automatisms, and hyposexuality which may have a larger impact on sexual functioning. Chronic use of antiepileptics may lead to sexual problems. During the seizure, deviant sexual behavior may be seen. Antiepileptics with lesser sexual side effects should be preferred.
SD may be due to a physiological dysfunction (primary dysfunction) or as a result of general physical disabilities (secondary dysfunction) or psychological and emotional issues (tertiary dysfunction). 19 In multiple sclerosis (MS), efferent nerves to the sexual organs may get damaged affecting arousal and orgasm. MS symptoms like fatigue or spasticity, bowel, and bladder incontinence may add to sexual problems. Psychological factors, cognitive impairment, and mood changes may affect the sex life negatively. Among men affected by MS who are ambulatory 60% develop ED and 40% to 50% have ejaculatory or orgasmic dysfunction and reduced desire. In women with MS, SD, assessed by Female Sexual Functioning Index, was present in 34.9% of females as compared to 21.3% in healthy controls. ED in MS can be managed with sildenafil and spasticity with baclofen or tizanidine.
Traumatic brain injury (TBI) can lead to personality changes, depression, and physical disability which can lead to sexual problems. Frontal and temporal lobe lesions are commonly associated with sexual problems. Lesions in the basal frontal and limbic areas can lead to hypersexual behavior. Anterior temporal lesions may result in Kluver-Bucy syndrome which is associated with hypersexual behavior. Sexual difficulty is reported in 36% to 54% of patients with severe TBI. Men usually suffer from erectile and ejaculatory dysfunction whereas women report reduced lubrication and dyspareunia. A spinal cord injury may lead to disruption in autonomic innervation resulting in sexual impairment. 20 Spasticity occurring post head injury can be managed with baclofen, tizanidine, botulinum toxin, or sclerosing agents. Dopamine agonists such as bromocriptine are helpful in improving motivation. Sexually inappropriate behavior can be managed with atypical antipsychotic medication, antiandrogens, clobazam, and SSRIs. Sex therapy and behavioral approaches such as time out and self-monitoring for sexual urges may be employed for inappropriate sexual behavior.
In spinal cord injury, sildenafil is particularly helpful in ED and for improving lubrication. Tadalafil, vardenafil, and midodrine can be helpful for improving ejaculatory problems. Spasticity can be managed as mentioned for head injury. Audio visual stimulation, nonsexual forms of intimacy, and manual stimulation can be helpful as and when required.
Sexual Disorders and Oncology
The prevalence of cancer has been increasing consistently with approximately 10 million deaths (~1 in 6 deaths) occurring globally in 2020. The most common cancers include those of breast, lung, colon, rectum, and prostate. Human papillomavirus and hepatitis are responsible for around 30% of cancer cases in low- and middle-income countries. Cancer affects the individual, as well as the family, and puts a strain on the health-care system. It impacts interpersonal relationships and leads to poor intimacy and poor sexual health. 21 Most oncologists don’t give adequate importance to the sexual health of the individual. Cancer survivors usually have a very strong negative impact on their psyche. Surgery, chemotherapy, and radiotherapy can result in poor body image issues, emotional changes, depression, and poor sexual health. SD in newly diagnosed cases and post cancer survivors is an important aspect to be dealt with by the oncologist in liaison with the psychiatrist.
Psychiatry and Other Specialties
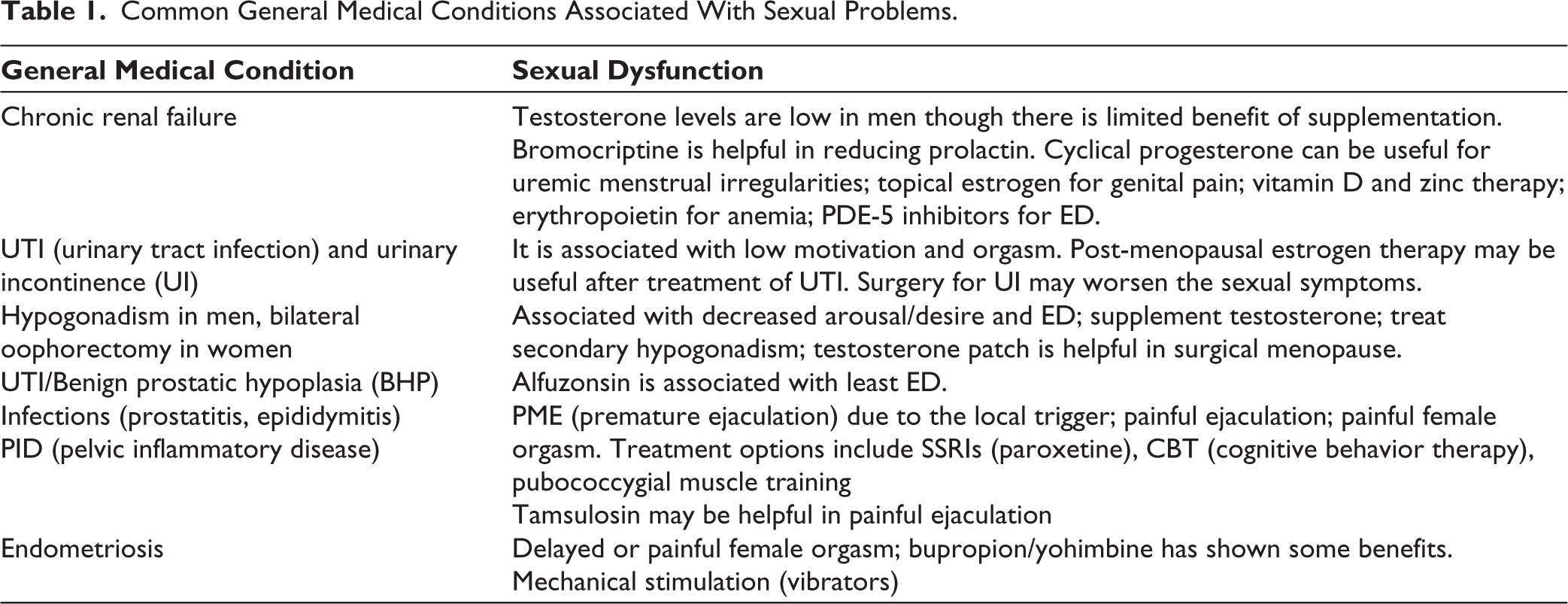
SD can be associated with a number of other physical conditions like chronic kidney disease, autoimmune conditions, or connective tissue disorders. Chronic pain associated with musculoskeletal disorders can lead to decreased libido and arousal, ED, and dyspareunia. Greater pain levels is associated with more SD. 22 Sexually transmitted infections, urinary tract infections, and chronic respiratory diseases may be associated with SD. Chronic inflammatory conditions like rheumatoid arthritis and inflammatory bowel disease are associated with decreased libido, reduced mobility, ED, and difficulties with arousal. Other common general medical conditions associated with sexual problems have been briefed in Table 1. 23
Common General Medical Conditions Associated With Sexual Problems.
Medication and Sexual Dysfunction
Various nonpsychotropic medications may lead to SD. Some of the general principles of management of drug-induced SD include:
Addressing the patient expectations, lifestyle, and any fears or misconceptions that may be present. Decreasing the dose or changing to a drug associated with lesser or no sexual side effects. Giving drug holidays. Giving cognitive behavioral therapy, supportive therapy, or sex therapy. Lifestyle modifications. Using PDE-5 inhibitors as and when indicated. Use of mechanical interventions such as vacuum pumps or vibrators. PDE-5 inhibitors can be combined with most antihypertensives but need to be avoided with nitrates to avoid risk of hypotension.
Sexual side effects related to certain medications are mentioned in Table 2. 23
Sexual Side Effects Related to Medications.
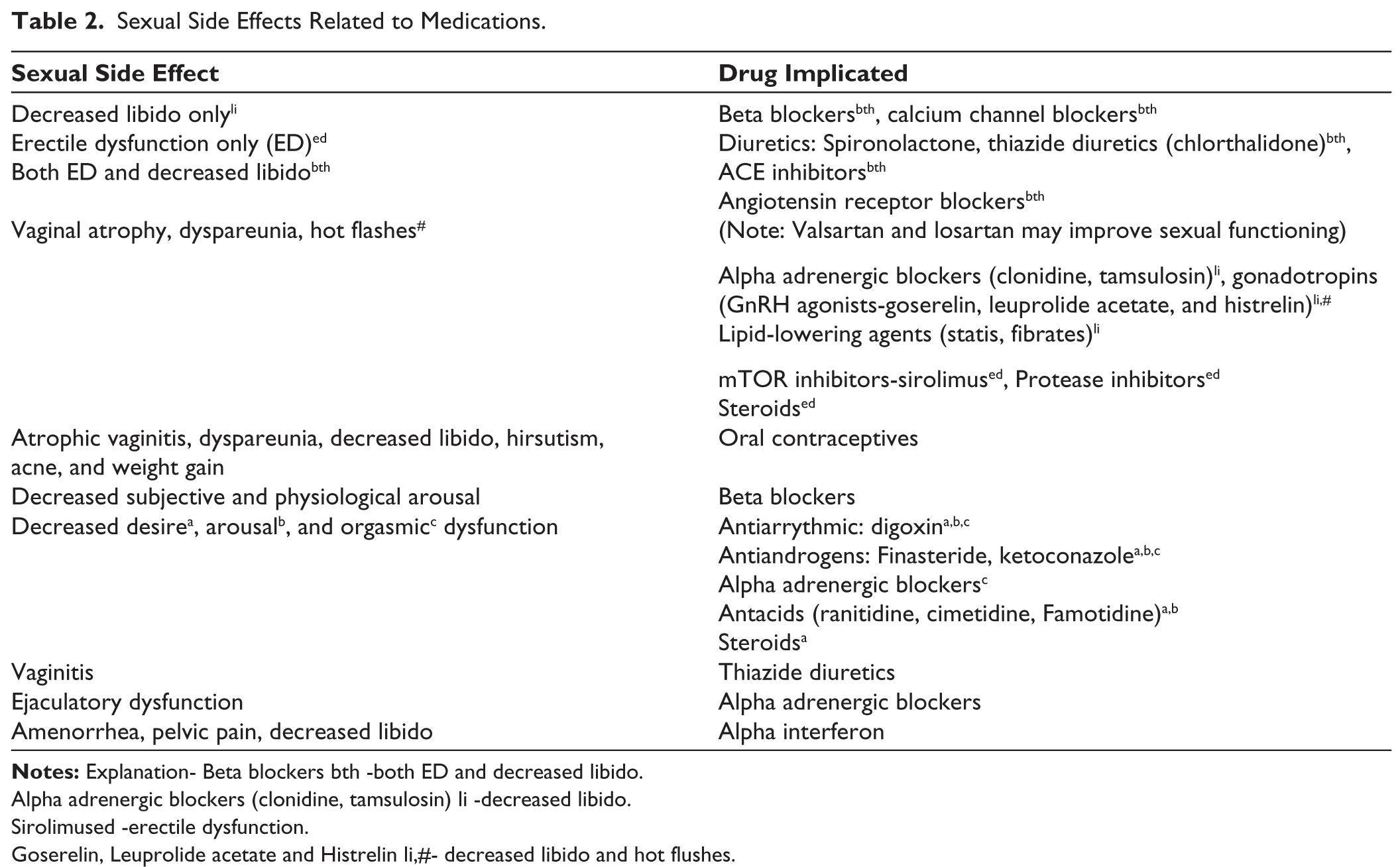
Alpha adrenergic blockers (clonidine, tamsulosin) li -decreased libido.
Sirolimused -erectile dysfunction.
Goserelin, Leuprolide acetate and Histrelin li,#- decreased libido and hot flushes.
Evaluation and General Principles of Management
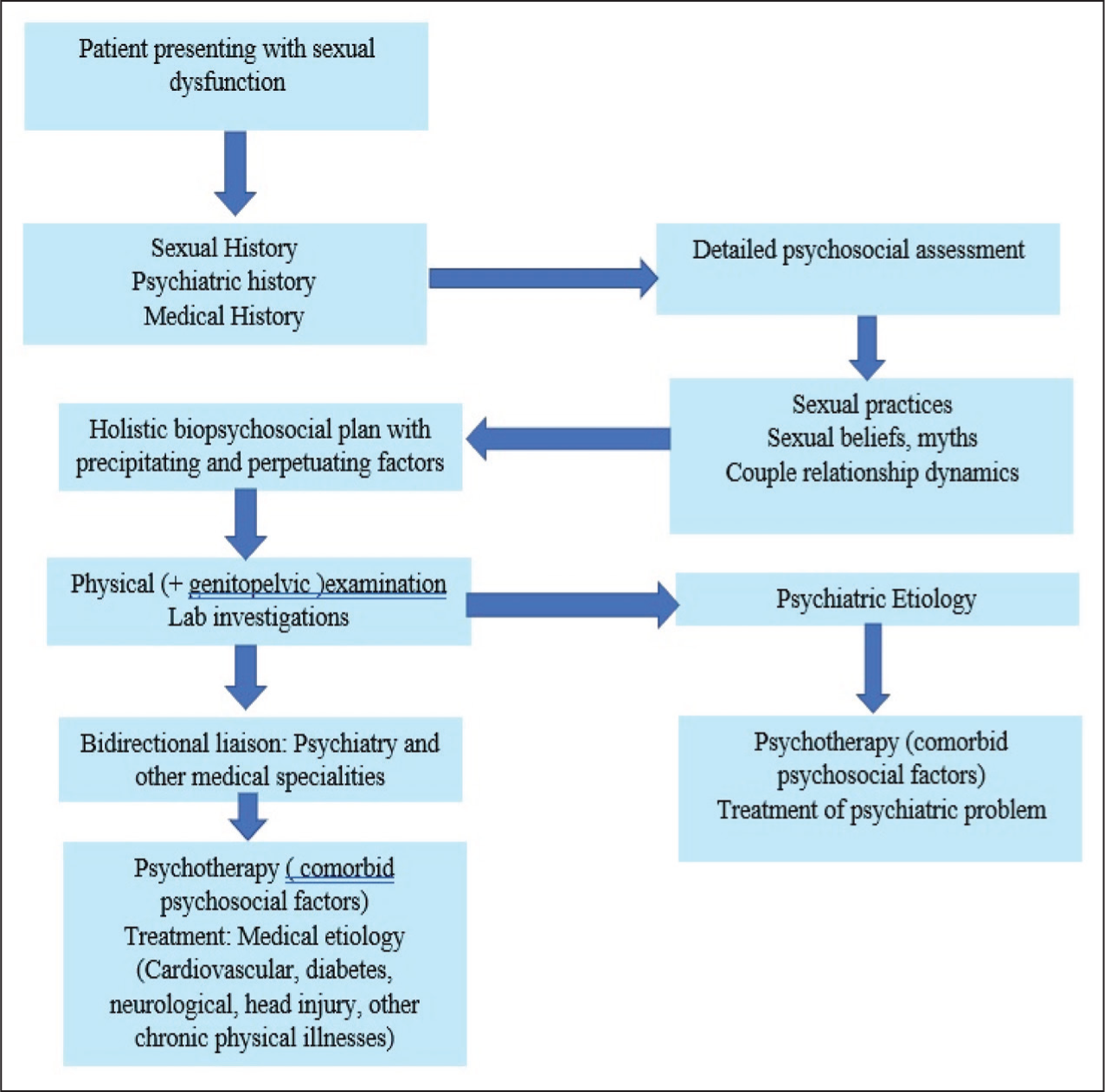
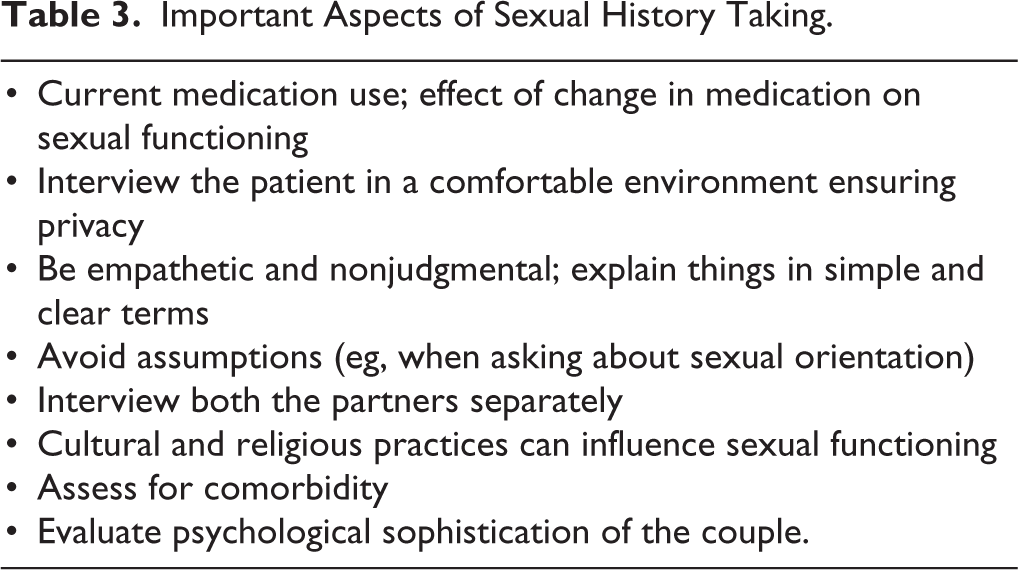
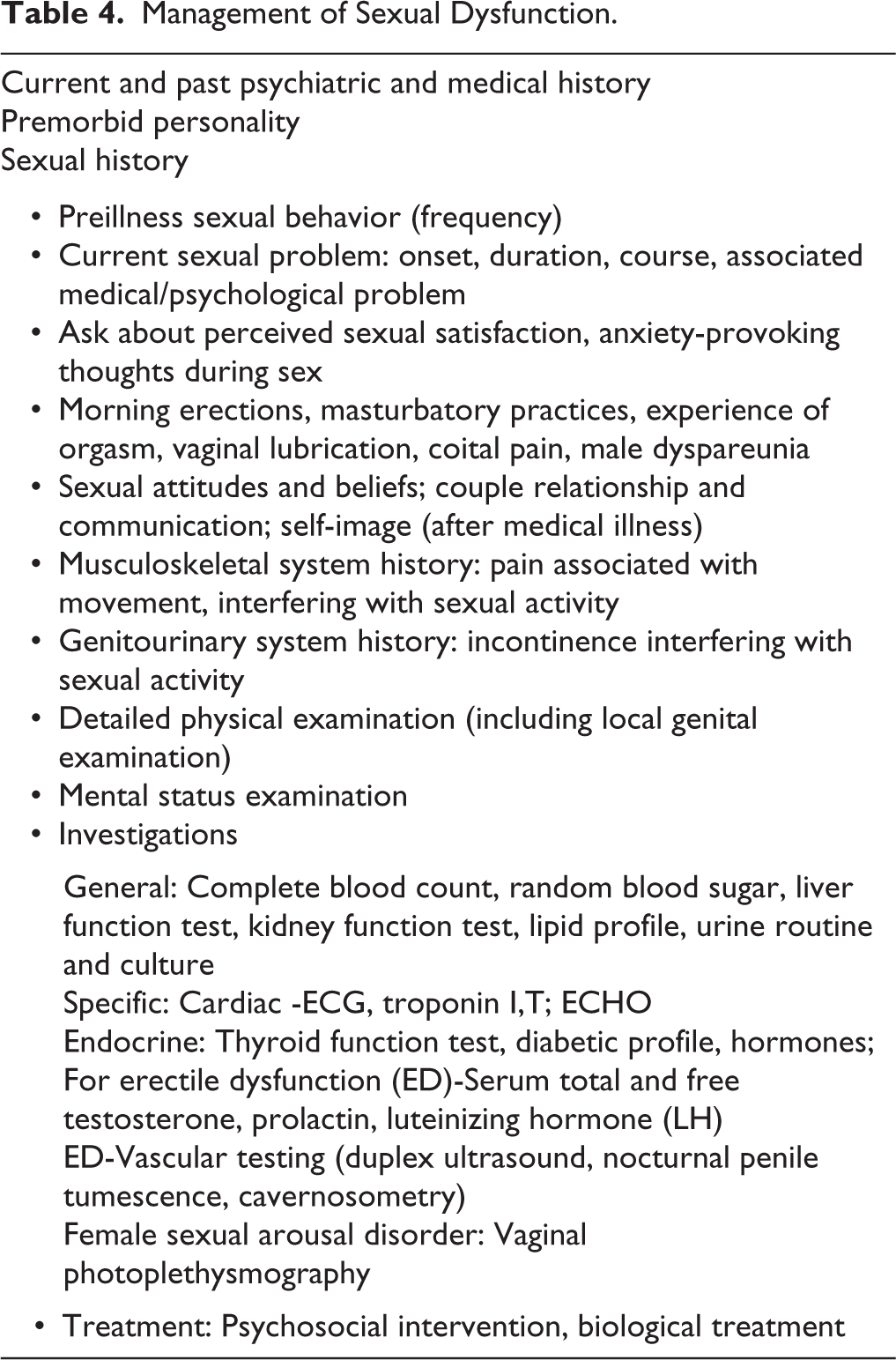
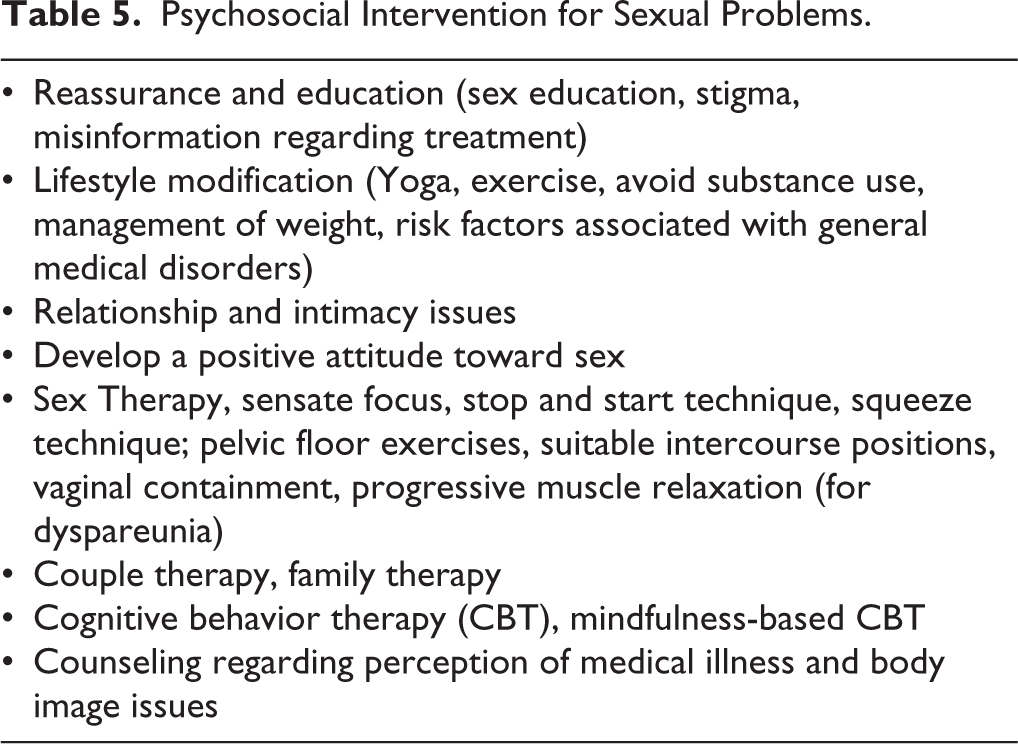
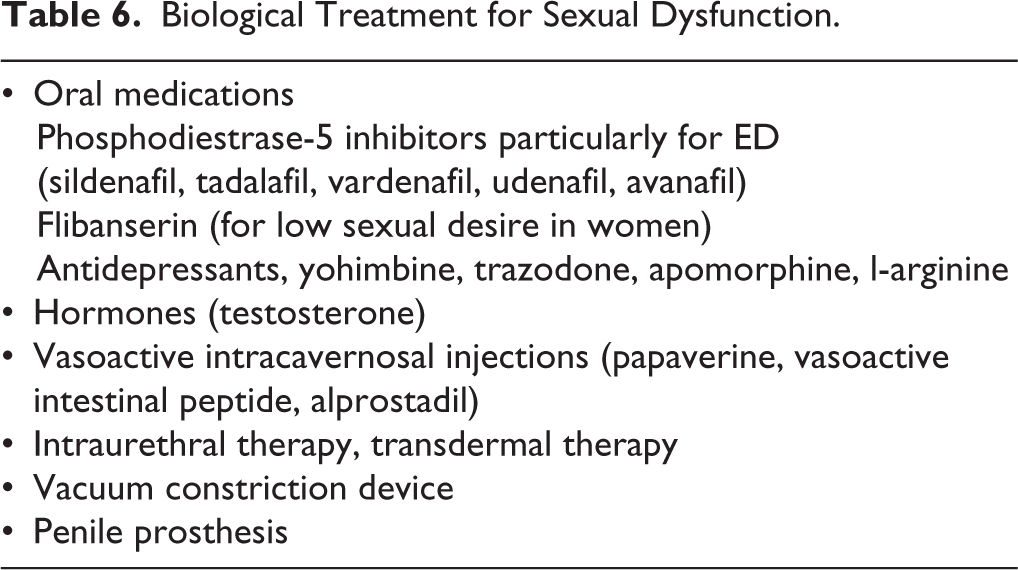
As per DSM-5 before making a SD diagnosis, the treating clinician needs to rule out a psychiatric disorder, SD, due to the effect of a specific substance of abuse or due to a general medical condition, or by marked interpersonal and psychosocial stress. The general principles of management have been outlined in Figure 2.24,25 Detailed current and medical history, psychiatric history, and sexual history should be taken. Important aspects of sexual history taking are mentioned in Table 3. Management of SD has been briefed in Table 4. Psychosocial interventions and biological treatment have been briefed in Tables 5 and 6, respectively. It is important here to note that there is no optimal level of sexual functioning for a couple. The perception and needs of the couple is taken as a guide for making treatment decisions.23,25
Management of Patient Presenting with Sexual Dysfunction.
Important Aspects of Sexual History Taking.
Management of Sexual Dysfunction.
Psychosocial Intervention for Sexual Problems.
Biological Treatment for Sexual Dysfunction.
It is imperative that the general medical condition be taken care of first. This may include treatment of endocrinal abnormalities involving the thyroid, low testosterone, diabetes, CVS morbidity, and arthritis. Very often, the burden of the chronic illness leads to adjustment problems and poor self-perception impairing the sexual relationship. A change of medication may be required if it is interfering with sexual functioning which is the most definitive treatment in some cases.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Not applicable.