
Abstract
Koro, a culture-bound syndrome originating from Southeast Asia is characterized by a perception of acute retraction of the penis, accompanied by an acute panic-like reaction of impending danger or death. Koro-like symptoms are considered variants of classical Koro syndrome and differ from it phenomenologically.
We described here a case series of secondary Koro, presenting as a delusional disorder who remitted on treatment with antipsychotics and maintained the improvement on follow-up.
It is important to differentiate between classical Koro with Koro-like syndrome, with exploration of any delusional core during clinical assessment for better categorization and management.
Introduction
Koro is a culture-bound syndrome originating from Southeast Asia. It is characterized by a perception of the retraction of the penis, accompanied by an anxiety symptom. 1 The classical culture-bound Koro syndrome is acute in onset and resolves within minutes to hours. If the symptom of penile retraction is long-standing, it is a Koro-like symptom can be a part of psychotic, affective, or substance use disorders. 2 These are considered variants of the classical Koro syndrome. In the literature, only a few cases have been described where Koro-like symptoms were part of psychosis3,4; however, no case has been described where Koro-like symptom is presented as the sole delusion. We described a case series of secondary Koro, presenting as a delusional disorder. Written informed consent has been obtained from the patients to furnish their information for publication.
Case 1
A 34-year-old married male developed a sudden onset of a belief that the whole length of his penis was missing; gradually over the next 6 months, he assumed it would have invaginated into his abdomen. Initially, he secretly visited a local physician with the request for abdominal imaging. After all the investigations and clinical examinations, while the physician conveyed a different opinion regarding his penile length, he ended in rising up a quarrel with him. He also started to develop distance in his intimate relationship with his wife, stating various excuses each time. He had no history of psychoactive substance use, past history, or family history. He was then accompanied by his wife and visited a nearby psychiatrist for the reason of sexual disinterest, where he was diagnosed with anxiety NOS and given fluoxetine, and then an adequate dose of paroxetine given for a specific duration. When no improvement was noticed, his wife brought him to our health facility. On the first day, he was not ready to tell us anything and denied every treatment. On mental status examination (MSE), we found him evasive and suggested Flupenthixol 0.5 mg twice daily; after 10 days, on the second visit to us, he opened up to us about the reason behind his sexual absenteeism. On MSE, this time we found that his affect was anxious regarding his penile length. He was holding a delusion that the missing portion of his penis was retracted into his abdomen. He had no perceptual abnormalities, like hallucinations or illusions, other than body image perception regarding penis size; higher cognitive function was unremarkable; and he had grade II insight. We then prescribed him Flupenthixol 1.5 mg twice daily. After 3 weeks, he became completely well, as reported by his wife. The patient is doing well with Flupenthixol 3 mg and is symptom-free for more than 1 year now.
Case 2
A wife brought her 36-year-old husband to our psychiatric facility for abnormal behavior of checking and measuring his penis once daily for the last 7 months. He was treated by an outside psychiatrist with 60 mg of fluoxetine for 3 months, but no improvement occurred. He was reluctantly brought by his wife to us. In the interview, he said, “No doctor and medicine can cure him, it is his ultimate fate of dying; it is because of changes in earth’s magnetic field that his penis had been repelling into his abdomen.” He also revealed that he checks it daily to count the number of days left for him to reach the ultimate day of his demise. His wife assured him several times that his penis size was the same as before, but he used to become irritable and often abused his wife verbally. He had no history of psychoactive substance use or family history. On MSE, he had a delusion of penile retraction in the abdomen and anxious affect regarding upcoming death, and higher cognitive function was unremarkable. We started him on Flupenthixol 1.5 mg daily, and after the third week of treatment, he agreed that the earth’s magnetic field was no longer acting on him for the last week as his penis is maintained at the same size. We increased Flupenthixol up to 3 mg/day, and after 1 month of treatment, the same patient thanked us that his penis had regained its usual size. The patient is symptom free for 6 months now, with the same treatment.
Case 3
A 33-year-old unmarried male was referred to us from general OPD with an absurd complaint. According to the patient, from the last 3 months, his penis had been pulled inside the abdomen. He feared that it would ultimately merge with his abdomen or there may be a creation of a gap in its place; in turn, he shall lose his gender. He first disclosed it to his friend, but he refused it on its plausibility; for this reason, there is an initial altercation followed by a fight attempted by the patient himself. Subsequently, all of his friends started avoiding him. He had no history of psychoactive substance use, past history, or family history. On MSE, there was a delusion regarding the reduction of the penis inside the abdomen and affect was anxious related to the same, while higher cognitive function was unremarkable. We suggested him Flupenthixol 1.5 mg daily for 1 month, and on the next visit, he denied any abnormalities regarding his penis. The patient is in full remission for almost 9 months with the continuation of treatment.
Case 4
A 43-year-old married person, who was previously sober and nice as per the informant (wife), accompanied by his wife, presented to us with a complaint that his penis was shrinking inside his abdomen. He then stopped going outside, always remaining confined to home, holding his penis in one hand so that it does not pull into his abdomen. He also remained awake in the night and asked his wife to hold it or tie it to a window if he was asleep. His wife tried to console him of nothingness, but the patient became verbally and physically abusive. He was also not ready to accept any treatment and believed all of his problems were because of weather changes, and once this weather goes off, he would be fit and fine. He had no history of psychoactive substance use or family history. On MSE, his affect was anxious related to shrinkage of the penis and delusional belief regarding the same in thought content, and higher cognitive function was unremarkable. He was suggested Quetiapine gradually up to a dose of 300 mg, and after receiving the same for 3 weeks, the patient’s condition improved. The patient currently has had no delusions for the last 5 months with the same treatment.
Discussion
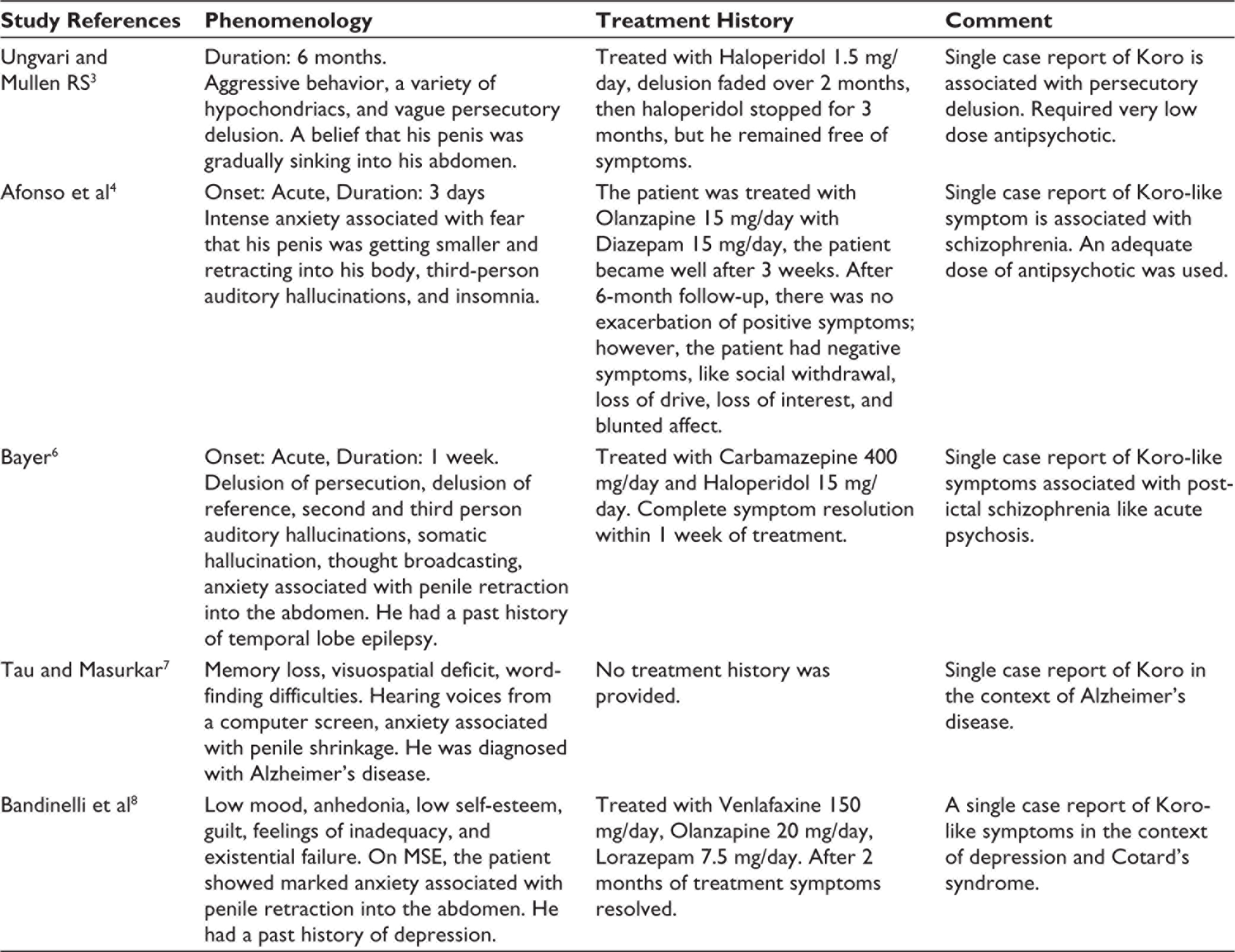
All of our patients held the belief of penile shrinkage into the abdomen for a long duration and were preoccupied with anxiety or fear related to penile shortening. That places them under the umbrella of Koro or Koro-like syndrome. 1 Their belief is often implausible in content, knitted with some apparently scientific logic, held extraordinarily strong and not amendable by different arguments or assurance; it is associated with a conspicuous behavioral component, affecting their sexual and social life and attributed to external circumstances, like weather change or the earth’s magnetic field, which stands with their delusional nature. 5 Our cases differ from previously reported cases, where delusion of penile retraction was present with hypochondriac and persecutory delusions, 3 as a part post-ictal psychosis with schizophrenia-like symptoms, 6 as a part of schizophrenia, 4 along with other psychotic symptoms in Alzheimer’s disease, 7 and as a part of depression and Cotard’s syndrome 8 Table 1.
Brief Description of Koro and Koro-Like Symptom in Literature
Conclusion
It is important to differentiate Koro-like symptoms from classical Koro for suitable pharmacological management. Antipsychotics have their place in the treatment of Koro with a delusional core. Further studies need to be done to get a better understanding of the variants of classical Koro syndrome and their management.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.