
Abstract
Klinefelter syndrome (KS), a disorder of abnormal sexual differentiation, is characterized by the presence of an excess X chromosome in males (47, XXY). KS is associated with various neuropsychiatric manifestations such as anxiety, depression, schizotypy, and frank psychosis. Psychosocial factors including stigma and poor coping or psychobiological comorbidities due to neuroendocrine mechanisms have been posited to explain these symptoms. We report the case of a young male with an anxious temperament who presented with the culture-bound neurosis of Koro, which evolved into schizophrenia. The patient also had gender dysphoria and significant social anxiety. The report highlights the implications of anxious traits leading to developing culture-bound neurosis in the prodromal phase of schizophrenia in a patient with KS and its influence on treatment strategies. Integrated psychopharmacological, psychological, and psychosocial interventions are required to promote recovery in patients with KS.
Introduction
Klinefelter syndrome (KS), a disorder of sex development (DSD), is characterized by the presence of an excess X chromosome in males (47XXY). KS is associated with gynecomastia, small testes, eunuchoid features, sparse body hair, and so on. Its incidence among newborn boys is 1/500 to 1/700. DSDs are associated with various mental health consequences and psychiatric comorbidities. Patients suffer from gender dysphoria, anxiety, and depression.1, 2 The supernumerary X chromosome can predispose to the genesis of psychopathology leading to multiple psychiatric comorbidities: hyperactivity disorder, learning disorders, social phobia, schizotypal personality, and schizophrenia-like psychosis.3–5
We present a case that highlights the implications of anxious traits in developing Koro in the prodromal phase of schizophrenia in a patient with KS. The etiological, diagnostic, and management implications of the clinical presentation and a comprehensive recovery guide are emphasized.
Summary
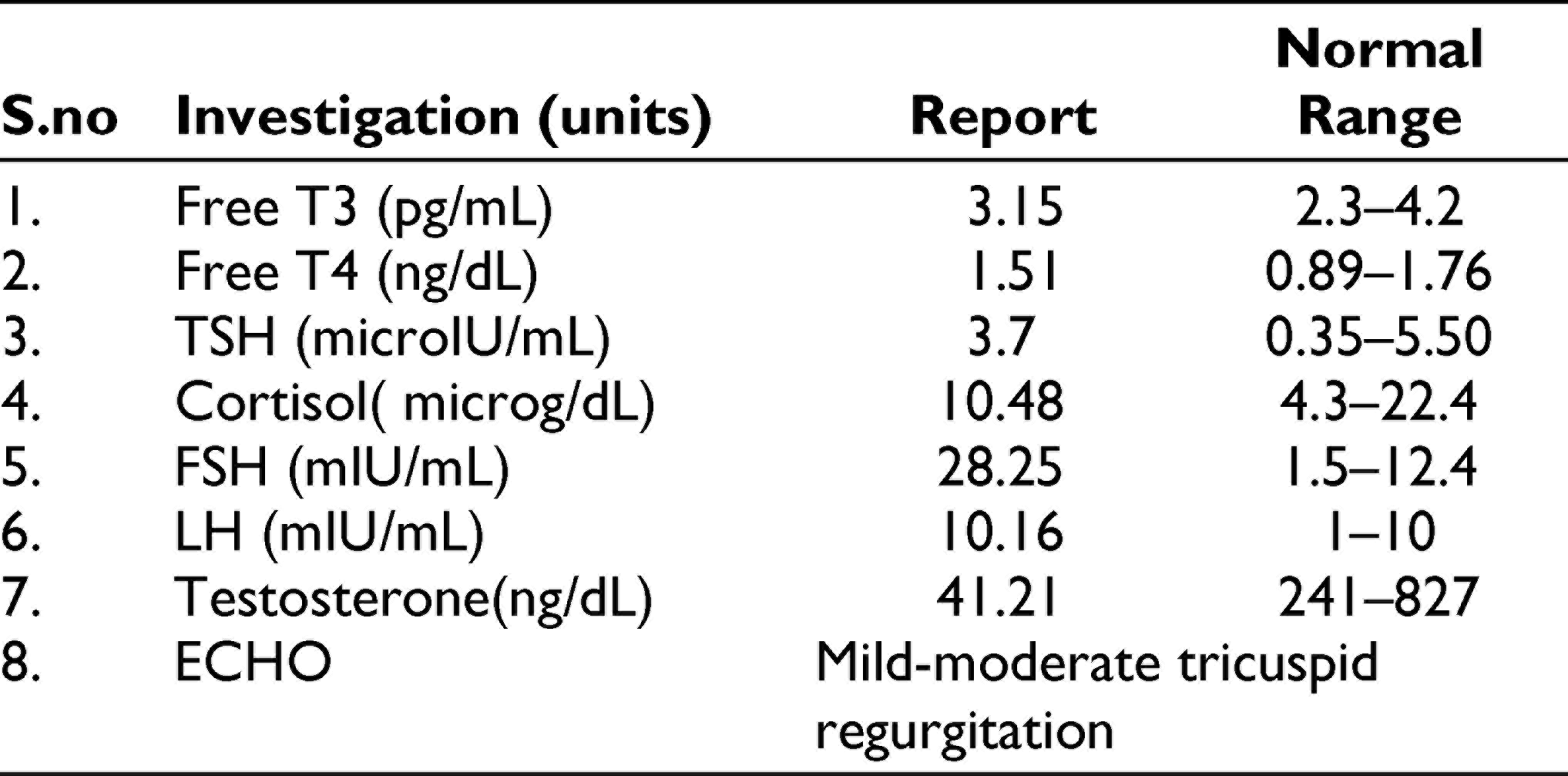
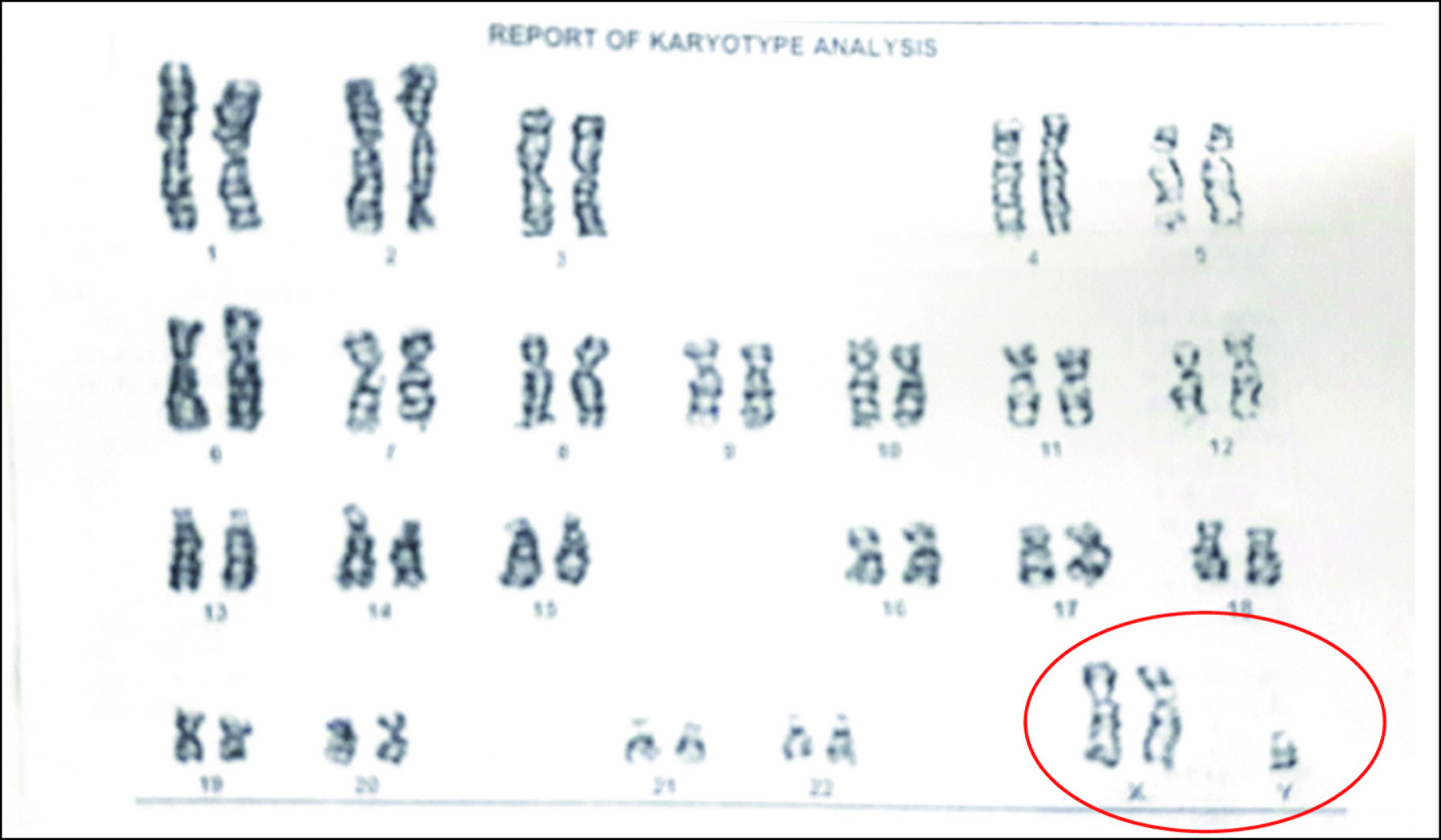
A 24-year-old man from Kerala presented with complaints of mood swings and disturbed biological functions for 5 years. During childhood, he was slow to warm in temperament and had thumb sucking and nail-biting. His adolescence was tormented with feelings of insecurity, negative self-evaluation, and social anxiety. The present illness started with heightened anxiety, irritability, and excessive somatic concerns. He felt that his penis was shrinking and withdrawing itself into his body, with fears of disability and death. His sexual history revealed a bisexual orientation that he had lingered infrequent attractions toward males apart from being sexually aroused by females. He also harbored excessive masturbatory guilt since adolescence. He attributed the cause of the present feminine physical appearance (including his gynecomastia and sparse body hair) to his erratic masturbatory practices and the socially forbidden attraction toward people of the same gender. The anxiety symptoms persisted untreated for 3 years. When his sibling joined work, he felt upset that he was unemployed. Over weeks, he became withdrawn and inactive. There were no depressive cognitions, delusions, or hallucinations at this time. After 3 years of having these symptoms, he reported auditory hallucinations of women calling out to him, console him, and give him simple commands. A year later, he developed visual hallucinations of an angel in a white gown with wings and yellow hair. He suspected that his neighbors posed danger and discussed about him with bad notions. He had developed nicotine dependence (cigarette smoking) in those 2 years. His past and family history were nil contributory. The patient was overweight, had gynecomastia, and sparse facial and axillary hair. He was anxious, expressed delusions of reference, and persecution against neighbors, had overvalued idea of “shrinking penis,” visual, and auditory hallucinations. The endocrine assays and karyotyping (Figure 1) supported the diagnosis of KS (Table 1). Risperidone (4-6 mg/day) and hormonal therapy (testosterone enanthate 50 mg IM once a month) were initiated. His symptoms improved significantly as reflected by Brief Psychiatric Rating Scale scores (Baseline: 43; After 8 weeks: 28). Even after the psychotic symptoms, subsided the sexuality concerns and guilt persisted requiring concurrent individual psychotherapy. Paranoid schizophrenia, prodromal other specified neurotic disorders (Koro syndrome), and anxious avoidant personality disorder were diagnosed as per the International Classification of Diseases 10th edition (ICD-10). 6 Koro syndrome was made as a separate diagnosis since the onset of ideas of his penis shrinking preceded that of his psychotic symptoms by 3.
Summarizes the Results of Blood Investigations and Hormonal Assays
The Karyotyping of the Patient Shows the Presence of an Additional X Chromosome Leading to 47 Chromosomes (47, XXY)
The family was psychoeducated about the genetic disorder, associated psychiatric disturbances, need for medication compliance, and vocational rehabilitation. The patient was followed up for 6 months with sustained improvement. Informed consent was obtained from the patient for this report.
Discussion
A myriad of psychiatric presentations can occur in patients with KS. Studies have reported comorbid occurrences of depression, hyperactivity, autism and schizotypy in KS. 3 However, the present case reveals the association of KS with culture-bound syndrome (CBS) and its subsequent break down into psychosis. The case asserts that, apart from schizotypy, anxious avoidant personality can coexist with KS and predispose to CBSs. 4
Though literature supports the evolution of psychosis from neurotic states, the present case had two unique features: (a) occurrence of CBS in the prodromal phase of psychosis and (b) a distinct diagnostic trajectory from genetic vulnerability of DSD to frank psychosis (KS anxious temperament CBS psychosis). Further systematic research is necessary to explore such associations and to ascertain a common neurobiological or psychological substrate for KS and psychosis. However, in our review of current evidence, we found both Koro and KS cases have been reported to be associated with urogenital pathology, anxiety, and psychosexual dysfunction.7–9
Koro syndrome is a culture-bound syndrome reported in both sporadic and epidemic forms. Several cases have been reported from India in the states of West Bengal, Kerala, and Assam. Our patient is from Kerala. With globalization, boundaries between cultures are blurred resulting in reports of sporadic cases of Koro syndrome from Kerala. 10 Patients with DSD are susceptible to gender dysphoria due to various reasons: belonging to third gender, gender queer, alternating gender roles, or gender expression that differed from the reported gender. Such patients report complex feelings of low self-esteem, anxiety, and depression which require concurrent psychotherapy.1, 8, 11 The maladaptive psychological attitudes in KF can be explained by the additional X chromosome, which induces “catastrophizing” as a coping mechanism. 12 The germination of psychotic symptoms can be explained by the altered differentiation and functioning of grey and white matter in the frontal and temporal lobes leading to an increased propensity for psychotic symptoms. Studies on structural abnormalities of the amygdala, the skewed X-chromosome inactivation pattern, CAG repeat length, and parent-of-origin of X chromosome are inconclusive on the influence of X chromosome on psychiatric manifestations. Hence, further research is required with larger sample size. 2
Multimodal treatment becomes essential in managing KS and associated psychiatric comorbidities. Testosterone treatment from puberty may assist in psychosocial adaption during adolescence. The prodrome before the psychosis highlights that coping skills training and stress management exercises can impede progression to psychosis. Patients with DSD, KS will require early screening and intervention for personality characteristics and maladaptive coping strategies to prevent the emergence of psychosis.8, 13 Further research should elucidate the genetic mechanisms at play resulting in multifarious psychopathology.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.