
Abstract
Introduction: Koro is a culture-bound syndrome, common in India, characterized by the belief that one’s genitals are shrinking followed by the fear of impending death. Significant social stressors can precipitate this syndrome in vulnerable populations. One such factor is migration which is associated with increased vulnerability to neurosis and poor coping. It has been a less studied factor in the genesis of Koro and the same has been an interesting association in this study.
Methods: There was an outbreak of Koro (13 cases: 8 males and 5 females) among a population (n = 52) from east and middle India who had migrated to the south for manual work. These cases presented in clusters to our psychiatry outpatient department within a span of 2 weeks. We did an observational study to explore the sociodemographic and clinical correlates of these patients. Their perceptions and attributions to the illness were also reported.
Results: Most patients were married men with lower socioeconomic status and no formal education. More females were however affected than earlier reported data. Most patients knew about the illness and believed that it was contagious. Death anxiety, loss of libido, and insomnia were common associated complaints. Males feared impotence, whereas females feared of “loss of child-bearing” abilities. The major attributing factors to the illness were migration, the stigma of working near a “mental hospital,” and sharing shelter with the affected. Pharmacotherapy and single-session cognitive behavioral therapy were used for treatment.
Conclusions: Our study revealed unique clinical correlates and belief-systems of patients affected with Koro. It is time we stop seeing it just as “culture-bound syndrome” and begin seeing it also as a social disorder caused by distortion of body-related beliefs. Migration being a significant environmental stressor can often precipitate such culture-bound syndromes. Further mixed-method studies are warranted.
Introduction
It is established that culture plays a crucial role in the generation of psychopathology. “Culture-bound syndrome” is a broad-term encompassing location or culture-specific repetitive abnormal behavior or cognition, which causes significant distress. These problems need to be understood within the specific cultural purview to make sense. They are characterized by a strong familiarity within cultures, being considered as a “disease” and amenability to traditional medicine. 1 Koro is one such culture-bound syndrome characterized by the belief of one’s genitals or breasts retracting into the abdomen and fear of impending death due to the same. 2 Though claimed to be prevalent in the Southeast Asia, there have been reports of Koro outbreaks in Africa, 3 America, 4 and England 5 as well. Known by different names such as “Suoyang” in China and “Jhinjhinia” in Assam, 6 Koro is marked by significant distress in relation to the remedial measures adopted by patients to prevent the perceived genital retraction and death. 7 Most common of which are immersing the genitals in cold water or attaching weights around them. 8 The beliefs and perceptions around this disorder have shown to influence the pathogenesis, attributions, symptoms, and time to recovery.
Literature mentions sporadic cases of Koro, as well as outbreaks in clusters, commonly due to shared beliefs. Correlates studied are male gender, poor education, poor sexual knowledge, anxiety, high neuroticism, and dependent personality. 10 One of the major factors, however, which causes “forced acculturation” and increases “neurotic vulnerability” is an age-old anthropological phenomenon, 11 when a person shifts his residence from one political or administrative boundary to another, known as “migration.” 12 A universal phenomenon, migration has existed since human beings started exploring the world. When a group of individuals change geographic areas, they not only retain their lifestyle, but they also retain their beliefs. Migration has shown to influence quality of life, standards of living, and overall wellbeing all of which can eventually alter the risk of psychosexual disorders. As culture-bound syndromes are often conceptualized as “idioms of cultural distress” in response to trauma, 13 they can be viewed through socially traumatic experiences like migration. There is evidence that migration increases the risk to culture-bound syndromes. 14 Here, we present the details of outbreak of Koro among both males and females in a migrant population in South India. As the first case and the subsequent clusters presented separately, we describe them in separate sections. Appropriate informed consent has been taken from each of the study participants in their own language for the study.
The Migrant Population
A total of 52 (40 males and 12 females) people were involved in a construction work near our tertiary mental health facility. They had migrated from the states of Bihar, West Bengal, Orissa, Tripura, and Madhya Pradesh. A total of 8 of them had freshly migrated for the present job, while others were working earlier at other sites in different parts of Karnataka. They were daily-wage laborers and semi-skilled workers. They had been staying in 3 small colonies in a nearby slum in temporary shelter homes, together for the last 8 months. Due to necessities of work, they had started residing near the worksite in recent past. The first case had reported to us 2 weeks after their stay at the present worksite.
The First Presentation
A 29 years old, single mason, who had consulted our psychiatry department earlier for headache, presented to the outpatient department (OPD) with significant weakness as he believed that his penis has shrunk deep into his abdomen. He attributed it to the fact that he had shared meal with another patient from this hospital with similar complaints and was intensely distressed because of the same. He believed that he has turned infertile, has lost his “purpose” in life, and is going to die shortly. He had decreased sleep and anxious ruminations about his symptoms. There were no physical abnormalities, substance use, or any other premorbid illness. Family history was negative and blood biochemistry was normal. No syndromal depression was elicited. He had been pouring cold water repeatedly on his genital multiple times a day and on being asked by others in the colony had shared his symptoms in detail and his “attributions” behind them. According to him, 5 of his colleagues in the colony reported having similar symptoms that they had not disclosed to others. On hearing from them, they also practiced the same “cold water” treatment to get relief from their symptoms.
The Subsequent Cases
Over the next 2 weeks, 12 more patients (7 males and 5 females) presented with similar complaints. The males claimed “penile and scrotal retraction,” while the females believed that their breasts and vagina were shortening and disappearing within the body. The women had an additional fear of losing the “ability to bear a child” or “breast-feed.” The belief was widespread that it was a contagious and serious illness, with threat to life. Of the healthy migrant workers, 5 more came to OPD to seek help in preventing such symptoms from appearing. Detailed clinical interviews were conducted with the patients to understand their beliefs, practices, and perceptions about the symptoms of the illness. Associated comorbidity was diagnosed using International Classification of Diseases, Tenth Revision (ICD-10).
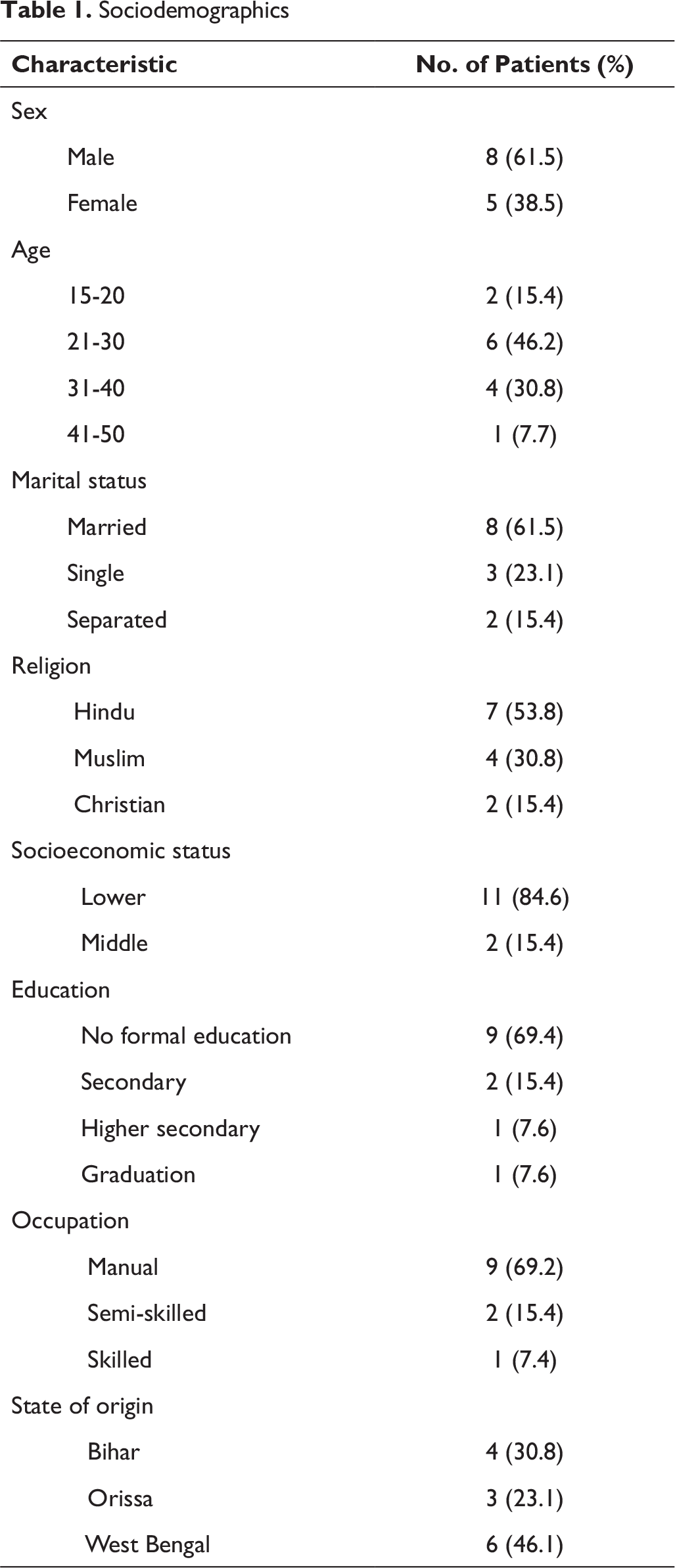
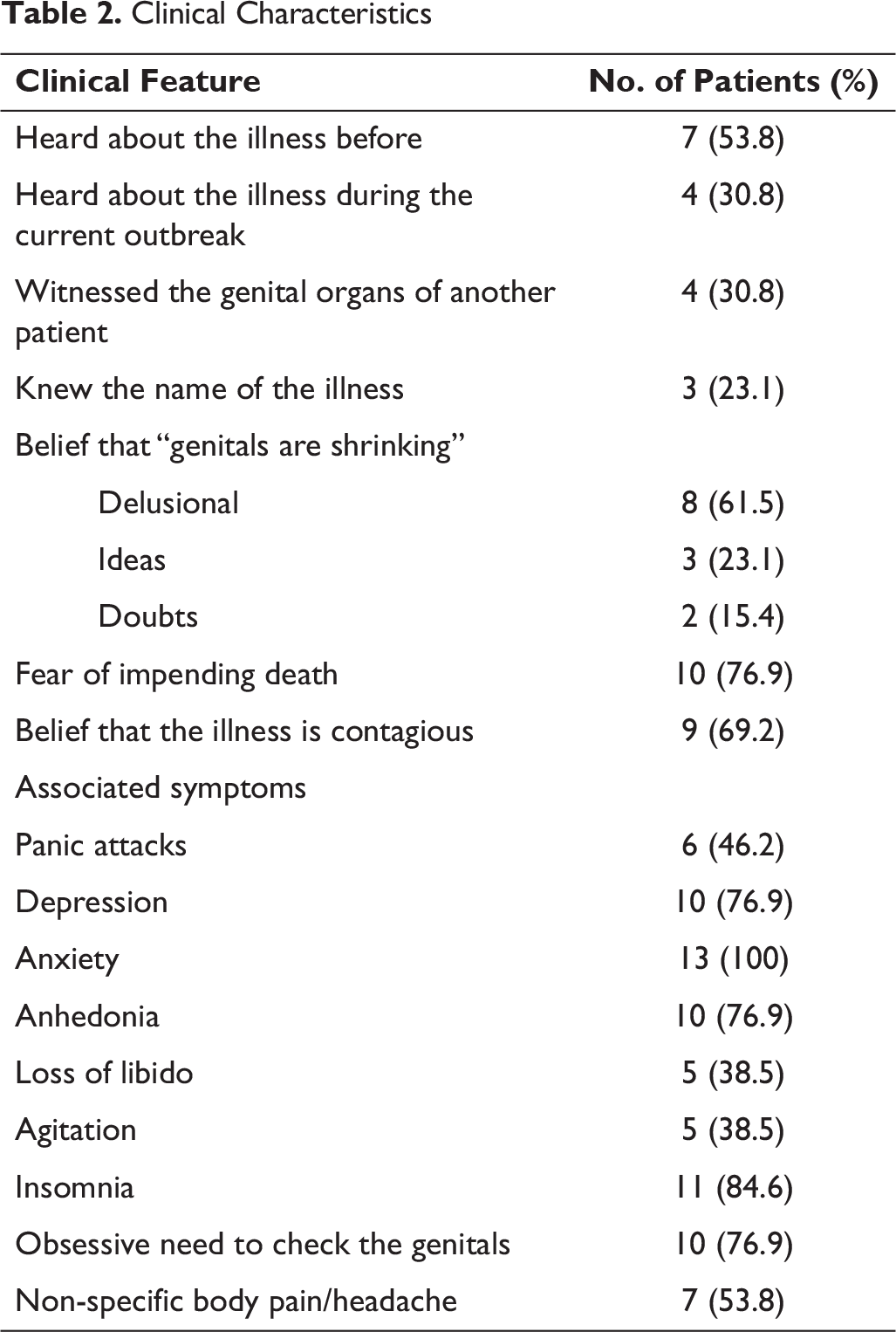
The sociodemographic and clinical characteristics are described in tables 1 and 2, respectively.
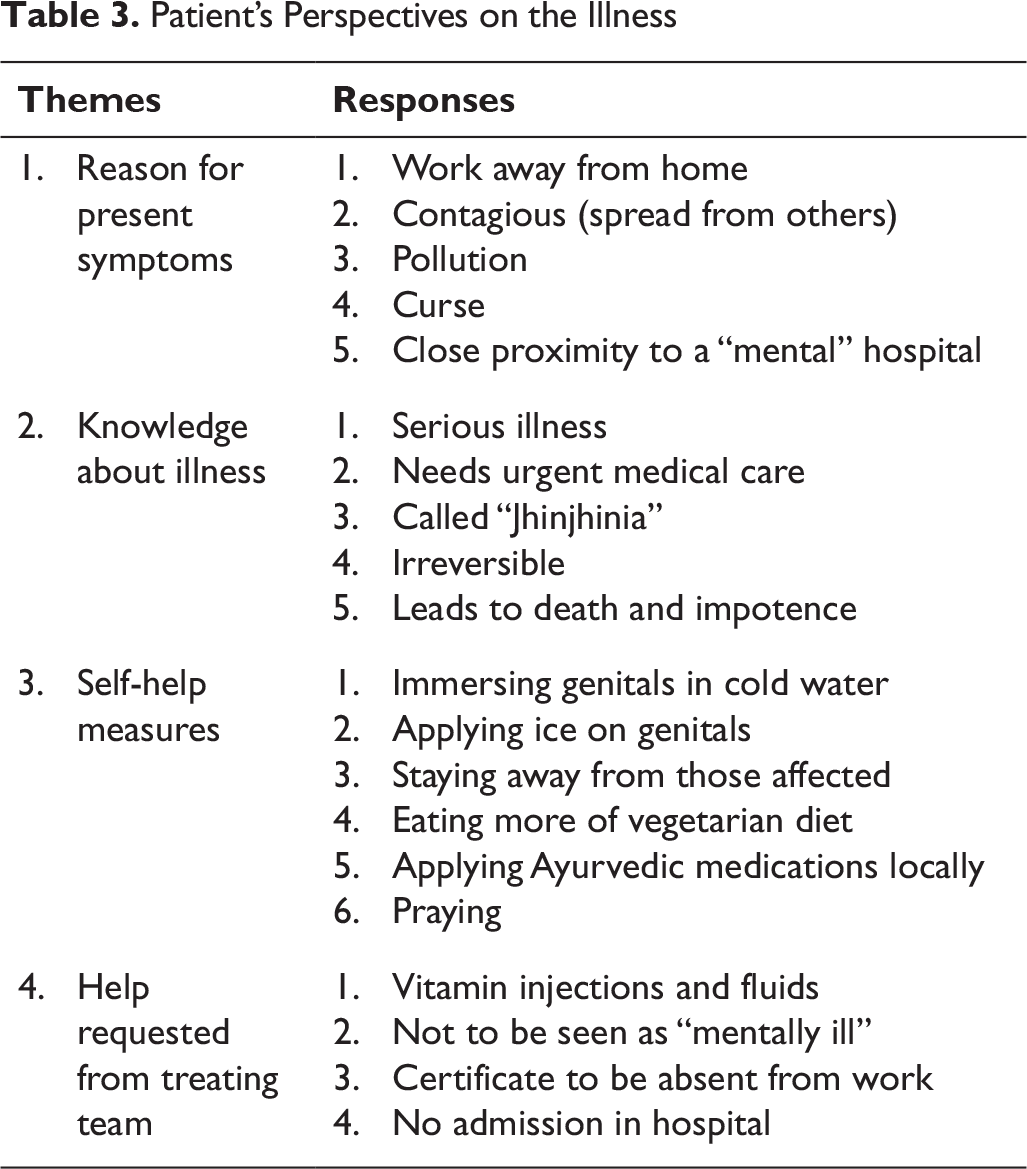
The perspectives, beliefs, and attributions of the patients were noted while clinical interviewing. Brief thematic analysis was done of their thought and perceptions under the respective headings of mental status examination. Leading but open-ended questions were asked about their attributions towards the illness. They are grouped under relevant headings and summarized in Table 3.
Management
Sociodemographics
Clinical Characteristics
Patient’s Perspectives on the Illness
Discussion
Culture-bound syndromes such as Koro often occur in clusters, with similar psychopathology among the affected. While in 2011, a study undertaken by Chakraborty and Sanyal reported an outbreak of Koro in jute-mill workers in East India, 15 Kumar et al. studied an epidemic of Koro in Northeast India in 2014. 9 Political unrest in the specific region and financial instability of the occupational setup were the respective stressors in the mentioned populations. The affected were mostly males having excessive preoccupation with masturbatory practices. Though our study population was fewer in number than these earlier studies, this outbreak had higher females and more married patients, which was different from the previous studies, and the domains of associated symptoms were varied. Most of them had known about the symptoms earlier and related them to their body. These case-clusters of Koro presented within 2 weeks of time after the index case, which is common for culture-bound syndromes. The fear of death, risk of impotence, and irreversibility of the condition were major fears of our patients. Females also had worry about further childbirth, which is of interest in psychopathology. Genital retraction in females has been mentioned in literature; 16 however, their symptoms and perceptions have never been detailed elsewhere. Traditionally, Koro has been mentioned as a “male” illness, 17 which might not be true. Also, the cultural context is important here. India, being a socioculturally diverse and populous population, separate areas and ethnic groups might have distinctive living habits, which form part of their identity. The north–south distinction is marked in India with respect to food, dietary habits, language, dressing, rituals, and customs. Difficulty in social “integration” and cultural acceptance in the migrated community might actually be important stressors in the genesis of “symptoms” as “expression of distress.” In terms of management, we tried escitalopram and benzodiazepines mainly for the short term to decrease the anxiety and normalize sleep, and patients benefited from the same. Also, the single-session CBT using reattribution principles was accepted well by the patients, though few continued the treatment. We are trying to formalize it into modules and validate it on a larger sample to use it systematically.
One other interesting feature of our cross-sectional study is the exploration of the perceptions of the patients. “Fear of working near a mental hospital” and “hearing about sexual symptoms from other patients” were their major attributions to the illness, along with “the distance of work from home.” Here is where the factor of migration pitches in and we propose that the “forced acculturation” needed for work along with the “fear of being rejected by a hostile environment” serve as significant triggers for developing such a neurotic state. As mentioned before, feeling “isolated” and “out of the place” can affect self-esteem, autonomy, identity, and perceptions about bodily symptoms. Literature mentions increased incidence of Koro and Dhat syndrome in migrant laborers. 9 India being known for its constant internal migration also serves as a fertile ground for a wide range of culture-bound syndromes. 18 In fact, Koro has been considered by some as a “cognitive amplification” of the body-related beliefs which just present to the forefront following a witness or discussion of the similar symptoms. 19 This can be well conceptualized in our patient population where they shared common shelter and “occupational ties,” witnessed other’s symptoms and even the affected parts, also involving in extensive discussion about the same, which could have perpetrated the outbreak. Migration is known to cause vulnerability to a wide range of mental disorders, along with poor coping strategies and somatization. 20 Cultural beliefs often get “amplified” to distort bodily perceptions creating an illness like Koro when a migrant work environment is perceived as “stigmatic” (“being near to a mental hospital”) and “hostile,” especially when the first case has heard similar symptoms of sexual dysfunction from a treated patient. Stigma related to “working near a mental hospital” in this case was a perceived “social stressor.” Self-doubts and self-blame in a migrant population further accelerate the symptoms. 21 We hypothesize that the stress of working in a “perceived alienated environment” together with attributional bias of the reported symptoms of the first case and inner genesis of fear have precipitated the trauma that could have led to the outbreak. This fits into the usual biopsychosocial perspective when applied to a culture-bound disorder. 22 In fact, Koro has been categorized as a functional somatic syndrome, the social hypothesis being the sociosomatic model. 23 Definitely, this is just an observational study and we cannot conclude that migration itself has been the sole stressing factor. The authors would also like to stress on the fact that the impact of migration as a social factor might be unique to the genesis of all culture-bound syndromes and not just Koro.
There are, however, many questions unanswered in this study. The pre-existing knowledge and attitude related to this illness have not yet been studied in depth. We need to follow up and find out the symptom remission in patients who left for the native land versus those who stayed at the present location. Also, their opinions about the single-session CBT as a form of treatment is worth exploring. The qualitative exploration is currently being conducted more systematically and in depth, the findings of which we are hopeful to study soon. There are thousands of migrants working in similar situations elsewhere. It might be interesting to understand the specific correlates of these migrant workers who were vulnerable to the Koro outbreak. The role of local media (digital and print) in influencing the symptoms was also not considered, though the media coverage happened only after the outbreak occurred. How it influenced the subsequent symptomatology is worth understanding. This also raises questions whether it is specific to certain sociocultural groups or any form of migration can increase the risk for culture-bound syndromes. While our small sample and observational nature of the study cannot comment on the causative link, a putative association between migration and the expression of “acculturated trauma” as psychosexual symptoms and finally the attributional patterns are interesting and generate interest for larger studies.
Conclusion
Koro is a well-known culture-bound syndrome which is often debated in its diagnostic positioning. 24 It might be more related to “body-specific beliefs” in certain regions, exemplified by social stressors rather than being “culture-related” per se. This debate will continue for days to come. Traditionally, culture-bound syndromes are usually localized to a particular area and not well understood by people outside that cultural context. This cross-sectional study highlights the importance of understanding “illness in a localized population” beyond their own “geographical boundaries.” Migration is not always traumatic. Internal migration within India sustains the socioeconomic stability of the country and is a dynamic process. However, adjustment to a “different” location is also associated with a whole range of customs, traditions, values, and rituals. Here is where the “migration stress” plays a part. Inability to express distress in “socially” appropriate norms can manifest it into symptoms that are congruent to the native culture. Thus, the role of migration and the impact of its consequent stress on the psychopathology of culture-specific illnesses cannot be neglected. Our study just provides a brief insight into the same. Mixed-method studies are further warranted to explore the phenomenology, origin, and course of Koro in migrant populations.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Statement
Appropriate informed consent was sought from the participants.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.