
Abstract
Background:
Clinical research and evidence are limited regarding sexual functioning in patients with obsessive-compulsive disorder (OCD) and the impact of pharmacological treatment on it.
Aim:
To study and compare sexual functioning in females among three groups viz. drug naïve symptomatic OCD cases (Group 1), OCD patients receiving pharmacological treatment, and in remission (Group 2), and age-matched healthy controls (Group 3).
Method:
Heterosexual sexually active females of 18 and 45 years with OCD seeking treatment at a tertiary care center in north India were assessed on the Relationship Assessment Scale (RAS), Female Sexual Functioning Index (FSFI), and Sexual Quality of Life-Female (SQOL).
Results:
The sample consisted of 150 subjects, (50 in each group). The majority of women were married, in the reproductive age group (18-45 years). The majority of women in Groups 1, 2, and 3 (84%, 74%, and 82%, respectively), were Hindus and homemakers. Most belonged to the nuclear family (58%, 52%, and 54% in Groups 1, 2, and 3, respectively) and were educated up to secondary school and monthly family income was comparable among the groups which were 10,000-20,000 in most of them (50%, 54%, and 50% in Group 1, 2, and 3, respectively). All the groups were homogeneous regarding socio-demographic variables. Sexual dysfunction (SD) was 68% in (Group 1) and (Group 2) and 28% in (Group 3) as per FSFI. There was no significant difference between Group 1 and Group 2. Subjects having symptoms in contamination and sexual domain had more dysfunction in desire, arousal, and satisfaction. Sexual functioning and SQOL were negatively correlated with the age and duration of illness
Conclusion:
SD is significantly higher in both drug naïve symptomatic OCD and pharmacologically treated patients in remission in comparison to healthy controls. There is no major difference in sexual functioning of drug naïve and adequately treated patients receiving pharmacotherapy and currently in remission.
Introduction
Obsessive-compulsive disorder (OCD) is among one of the tenth leading and most disabling psychiatric conditions with an overall lifetime prevalence of 2%. 1 The lifetime prevalence of OCD is 1.6%-2.3% in the general population, with a point prevalence of nearly 1%.2-4 The average age of its onset is approximately 19.5 years. 5
Psycho-physiological abnormalities related to the sexual response cycle in both men and women are what define sexual dysfunctions (SD). 6 Patients with OCD may experience individual or diffuse effects on their sexual response cycle throughout all phases (desire, excitement, and orgasm). 7
High rates of sexual dissatisfaction and dysfunction are reported in OCD (54%-73%) in several historical studies. 8 A study, comparing SD in drug naïve out patient department (OPD) patients, of OCD, major depressive disorder (MDD), and generalized anxiety disorder (GAD), with those of healthy controls; found that about 76% of patients with MDD, 64% of patients with GAD, 50% of patients with OCD, and 30% of healthy controls had SD. Orgasmic dysfunction was found to be the most commonly reported symptom of OCD. 9
In addition, studies found that 24% of women with panic disorder and 57% of OCD felt that their anxiety symptoms had a detrimental impact on their ability to have sex. 10 The study discovered a negative correlation between sexual satisfaction and anxiety. Furthermore, the study analysis revealed that in comparison to the control group; women with OCD and their partners experienced reduced sexual satisfaction. 10 It appears that a complex and bidirectional relationship exists between SD and OCD. 11 It has been hypothesized that OCD and SD potentially involve a causative route. Increased sensitivity to anxiety could be a significant contributor to the onset and maintenance of SD.
Some specific symptoms, such as obsessions with pollution, religion, or sexuality, have been described to interfere with sexual function in the literature. 12 SD may result from avoidance, which is an important issue in the domain of contamination. Another relevant theme is disgust, which has been characterized as a core and deep-seated emotion in OCD. 13 Additionally, doubting and checking, which are rather common in OCD patients, may contribute to SD. 14 Other significant influencing elements in this matter are the high rate of OCD and depression co-morbidity, 15 sexual side effects of medication (such as SSRI [selective serotonin reuptake inhibitors]) in OCD, and sexual obsessions. 16
Furthermore, OCD is typically correlated with problems with interpersonal interactions. 17 Patients with OCD have reportedly had significant marital issues and distress. 18 As per studies approximately half of the patients either do not have partners or have not had sex in a long time. 19 Other factors, like social skill deficiencies, have been brought out as contributing to OCD patients’ difficulty forming and maintaining relationships 17 and sexual discontent is likely to play a significant part in this. According to a study, 50%-70% of a couple’s sexual pleasure and intimacy is lost when they report low sexual satisfaction. 20
Various other factors may influence sexual functioning or contentment in OCD patients. 21 SSRIs can decrease libido and precipitate erectile dysfunction, and can also delay ejaculation and female orgasm. 22 Although SSRI side effects are dosage-related and typically reversible, large doses are involved in OCD treatment and it has been found that side effects especially in the sexual domain are usually prolonged and may continue even after therapy has been terminated. 12 The persistent side effects include reduced libido, anesthesia around the genital region, difficulty in erection and ejaculation, loss of lubrication in females, and difficulty in attaining orgasm. 23 Research data have suggested that approximately 10%-50% of patients receiving SSRIs develop adverse effects.24,25
Overall, we can conclude that SD is found to be associated in patients with various psychiatric disorders and it may be linked to both psychopathology and medication implicated in the treatment of the disorder. Despite the considerable prevalence of SD among OCD patients and the negative effects it has on satisfaction related to marriage and life; most sufferers choose not to seek treatment, either out of embarrassment or ignorance of the issue.
The attitude of healthcare professionals toward sexual difficulties in those patients would be improved by knowledge of the prevalence and proposed processes of SDs in mental patients. This would lead to increased adherence to therapy. This study was performed to assess SD in female OCD patients to address some of these issues and questions. This research was conducted for the first time in our country and compares SD in drug naïve symptomatic OCD cases, cases with OCD in remission receiving psychopharmacological treatment and those of healthy adults.
Method
The study is a cross-sectional, observational study conducted, on cases presenting with OCD in OPD in the Department of Psychiatry of a tertiary care medical institution in north India.
Study Design & Sample
The study sample consists of 150 subjects (50 drugs naïve symptomatic OCD cases [Group 1], 50 OCD cases in remission under pharmacological treatment for at least three months [Group 2], and 50 groups matched for age-healthy controls [Group 3]).
Sample in Group 1 was drawn from sexually active females with last sexual intercourse within one month, aged 18-45 attending OPD diagnosed with OCD as per DSM-5 having a duration of illness for at least six months and those who were drug naïve and symptomatic at presentation and had not received any psychopharmacological treatment for at least past three months, able to speak and understand Hindi or English willing to give informed consent and cooperative for assessment. Group 2 included those cases diagnosed with OCD who were in remission under pharmacological treatment for at least three months.
Those having any psychiatric or medical illness, active suicidal ideation, any substance use disorder except tobacco use disorder and those whose partners had a significant physical, mental, or sexual disorder as per provided history and those reporting significant relationship discord affecting sexual relationship with partners were not included.
Age-group matched controls (Group 3) were taken from sexually active healthy females aged 18-45 years. Eligible hospital staff and accompanying persons to patients scoring less than 3 on the General Health Questionnaire (GHQ-12) were included. The exclusion criteria were the same for all the groups. As the study was planned with a pre-specified time frame, a convenient sampling technique was followed and a sample size of 50 individuals in each group was calculated after a thorough review of outpatient attendance in our center records over the past two years.
Procedure
All new and old patients diagnosed with OCD as per DSM-5 by the consultant in charge of OPD were screened as per selection criteria and those who were meeting inclusion criteria were evaluated on semi-structured proforma. Clinical selection criteria were assessed on Yale-Brown Obsessive-Compulsive Scale (Y-BOCS), 26 Dimensional Yale-Brown Obsessive-Compulsive Scale (DY-BOCS), 27 Relationship Assessment Scale (RAS), 28 Female Sexual Functioning Index (FSFI), 29 and Sexual Quality of Life-female (SQOL-f) 30 and data was collected.
Age-matched controls were recruited from non-blood relative healthy caregivers of patients attending OPDs, office staff and GHQ-12 31 were applied for the controls for screening and those who were meeting the selection criteria, were assessed on RAS, FSFI, and SQL-f and data was collected.
Assessment Tools Used
Y-BOCS was used to assess the presence and severity of OCD symptoms. It is a clinician-administered checklist (Y-BOCS-CS) to determine the target symptoms of OCD and a severity scale (Y-BOCS-SS) to assess the severity of obsessions and compulsions using a 5-point Likert scale from 0 to 4: total score being 0-40. 26
DY-BOCS is a semi-structured interview-based scale for assessing the presence and severity of OC symptom dimensions in two parts: (a) an 88-item OC symptom checklist; and (b) rating scales for each OC symptom dimension, for the assessment of the impairment caused by the symptoms and an overall estimate of OCD severity. The checklist provides a detailed description of six OC symptom dimensions. 27
RAS: is a 7-item Likert-scale based; for the assessment of intimacy (of a relationship). The respondents answer on a 5-point scale from 1 to 5 for each item. The higher the score, the more satisfied the indicates non-distressed partners. 28
FSFI is a 19-item questionnaire scale for the assessment of the key dimensions of sexual functioning in women in the previous month. It measures six domains—sexual desire, arousal, lubrication, orgasm, satisfaction and pain. A total FSFI score below 26.55 is taken as an indicator of FSD. 29
SQOL-F is a clinician-rated 18-item questionnaire rating scale. It is an eighteen-item 6-point Likert scale. The range is between 18 and 101. A higher score corresponds to a better quality of sexual functioning. Questions assess; sexual life: including both the physical sexual activities and the emotional sexual relationship a person has with their partner, sexual activity: includes any activity which may result in sexual stimulation or sexual pleasure, for example, intercourse, caressing, foreplay, masturbation (i.e., self-masturbation or your partner masturbating you) and oral sex (i.e., your partner giving you oral sex). 30
GHQ-12 is a screening device for identifying minor psychiatric disorders in the general population. It has 12 items and is rated on a Likert-type scoring method, 0 = less than usual, 1 = no more than usual, two rather more than usual and three much more than usual. Positive questions (Items 1, 3, 4, 7, and 12) are scored inversely. Any score exceeding three is classified as “psychiatric caseness.” 32
Statistical Analysis
The collected data were tabulated using computer software and statistically evaluated using a statistical package for the social sciences. The normality of the distribution of numeric variables in different subgroups of categorical variables has been checked by the Shapiro-Wilk test. The association between numeric variables and categorical variables among the group has been assessed by the Kruskal-Walli’s test and Mann-Whitney U test. The correlation was assessed by using the Spearman correlation. P < .05 were considered statistically significant.
Results
Socio-demographic and Clinical Characteristics
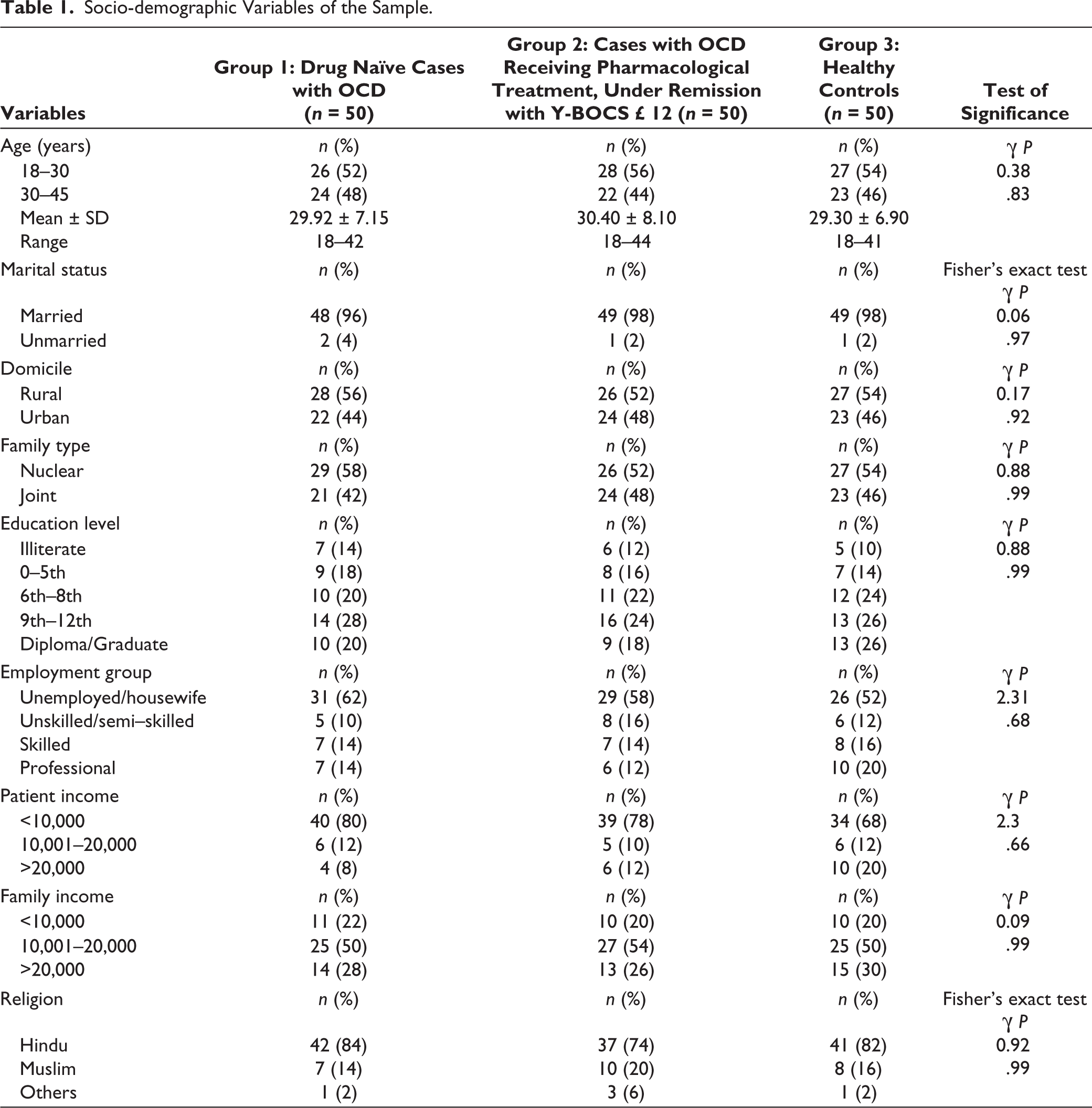
Majority of the subjects were married (96%, 98%, and 98% in Groups 1, 2, and 3, respectively) and were in the reproductive age group. Most of the cases in Group 1 (n = 26,52%) were aged 18-30 years. Most cases in Group 2 (n = 28,56%) were aged 18-30; were age-matched with (n = 27.54%) between 18 and 30 years in Group 3. Majority of the subjects belong to rural areas (56%, 52%, and 54% in Groups 1, 2, and 3, respectively). Majority of subjects belong to the nuclear family (58%, 52%, and 54% in Groups 1, 2, and 3, respectively). Majority of subjects in all three-group belonged to the Hindu religion (84%, 74%, and 82% in Groups 1, 2, and 3, respectively). Majority of the subjects in all three groups were studied up to secondary school. Also, majority of the subjects were unemployed (62%, 58%, and 52% in Groups 1, 2, and 3, respectively) and were dependent on their family income which was 10,000-20,000 in most of them (50%, 54%, and 50% in Group 1, 2, and 3, respectively). All three groups were comparable regarding socio-demographic variables (Table 1).
Socio-demographic Variables of the Sample.
Clinical Variables
The mean years of duration illness in our study sample were 5.5 ± 5.08 and 6.2 ± 5.89 in Group 1 and Group 2, respectively, which is evident from the chronic course and prolonged duration of the illness.
Assessment of Intimacy of Relationship, SD, and SQOL in Drug Naïve Symptomatic Patients of OCD (Group 1) as per RAS, FSFI, and SQOL-F Scores and Comparison with Healthy Controls (Group 3)
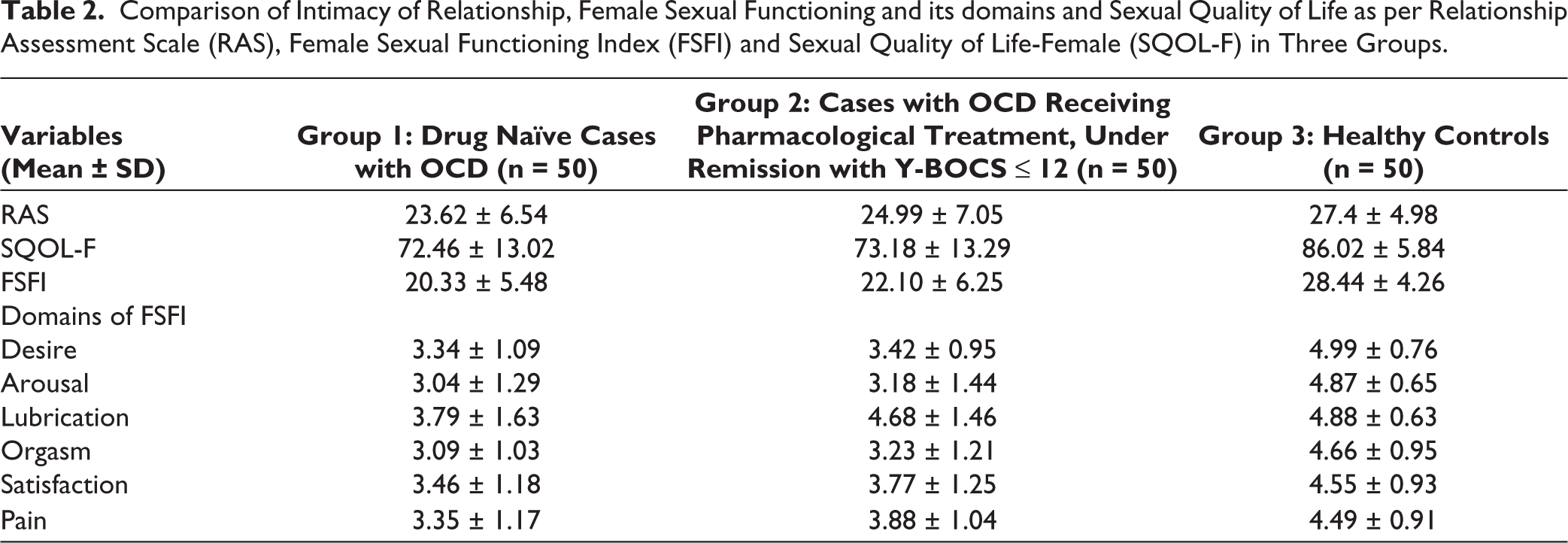
The mean RAS score was 23.62 ± 6.54 in Group 1 and 27.4 ± 4.98 in Group 3. On comparison of the means of the two groups, there was a statistically significant difference found with P < .007.
The mean FSFI score was 20.33 ± 5.48 for Group 1 as compared to 28.44 ± 4.26 for Group 3. On comparison of the means of the two groups, there was a statistically significant difference found with P < .0001. Thirty-four of the 50 cases (68%) in Group 1 had SD (score <26.55) on FSFI as compared to 14 of the 50 controls (28%) in Group 3. Cases in Group 1 were found to have dysfunction in the domain of desire (n = 45, 90%), arousal (n = 43, 86%), lubrication (n = 27, 54%), orgasm (n = 44,88%), satisfaction (n = 31, 62), and pain (n = 16, 32%).
The mean SQOL-f was 72.46 ± 13.02 in Group 1 and 86.02 ± 5.84 in Group 3. On comparison of the means of the two groups, there was a statistically significant difference found with P < .0001(Table 2).
Comparison of Intimacy of Relationship, Female Sexual Functioning and its domains and Sexual Quality of Life as per Relationship Assessment Scale (RAS), Female Sexual Functioning Index (FSFI) and Sexual Quality of Life-Female (SQOL-F) in Three Groups.
Assessment of Intimacy of Relationship, SD, and SQOL in Remitted Patients of OCD Receiving SSRIs (Group 2) as Assessed as per RAS, FSFI, and SQOL-f Scores and Comparison with Healthy Controls (Group 3)
The mean RAS score was 24.99 ± 7.05 in Group 2 and 27.4 ± 4.98 in Group 3. On comparison of the means of the two groups, there was a statistically significant difference found with P < .0003.
The mean FSFI score was 24.99 ± 7.05 for Group 2 as compared to 28.44 ± 4.26 for Group 3. On comparison of the means of the two groups, there was a statistically significant difference found with P <.0001. Thirty of the 50 cases (60%) in Group 1 had SD (score <26.55) on FSFI as compared to 14 of the 50 controls (28%) in Group 3. Cases in Group 2 had dysfunction in the domain of desire (n = 43, 86%), arousal (n = 44, 88%), lubrication (n = 35, 70%), orgasm (n = 39,78%), satisfaction (n = 38, 76%), pain (n = 22,44%).
The mean SQOL-f was 73.18 ± 13.29 in Group 2 and 86.02 ± 5.84 in Group 3. On comparison of the means of the two groups, there was a statistically significant difference found with P < .0001.
Comparison of Group 1 and Group 2 as per Scores of RAS, FSFI, and SQOL-F
The mean scores of Group 1 and Group 2 were statistically nonsignificant in terms of RAS, FSFI, and SQOL scores. Both groups were statistically significant when compared to Group 3.
Correlation of Socio-demographic and Clinical Variables with Intimacy of Relationship, SD, and SQOL in Group 1
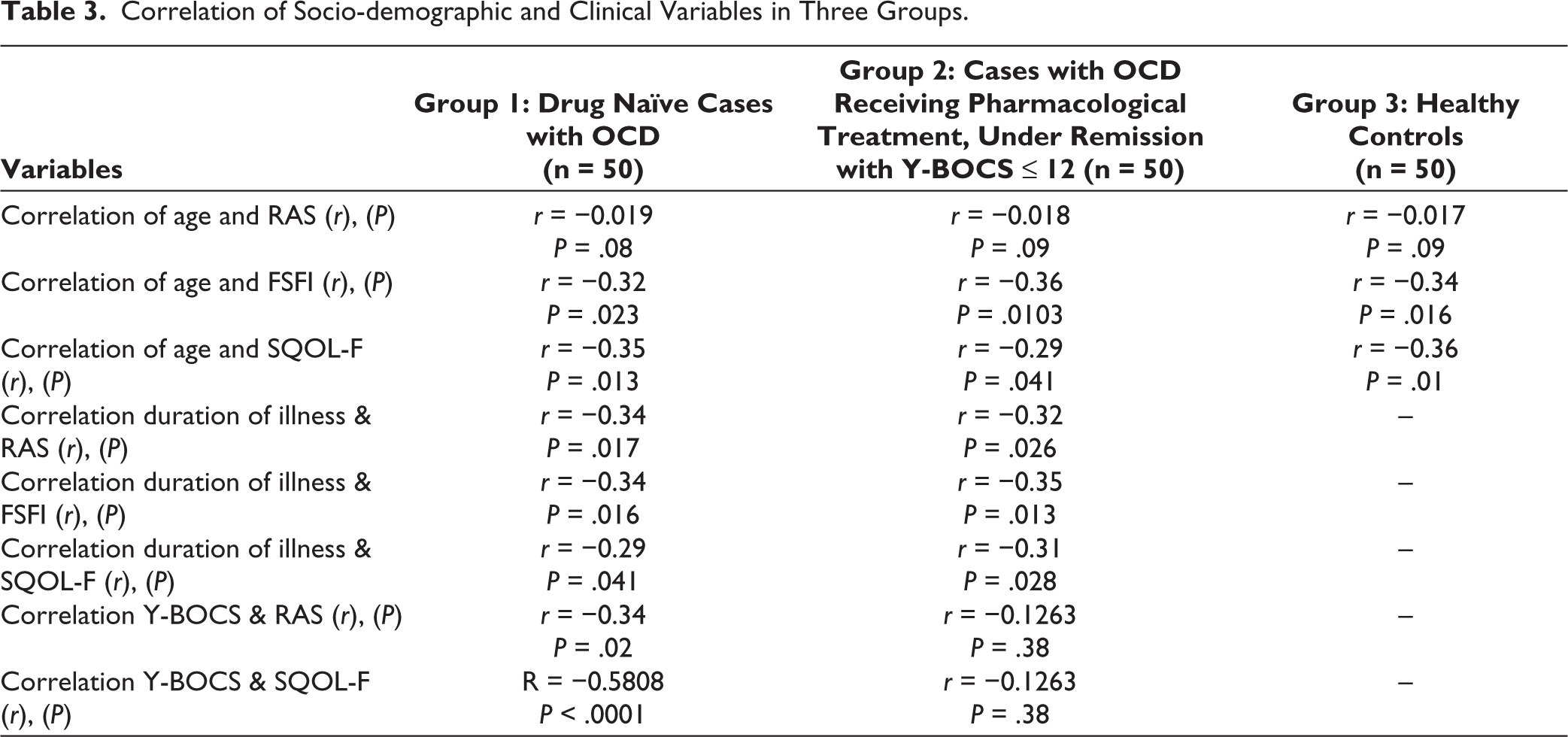
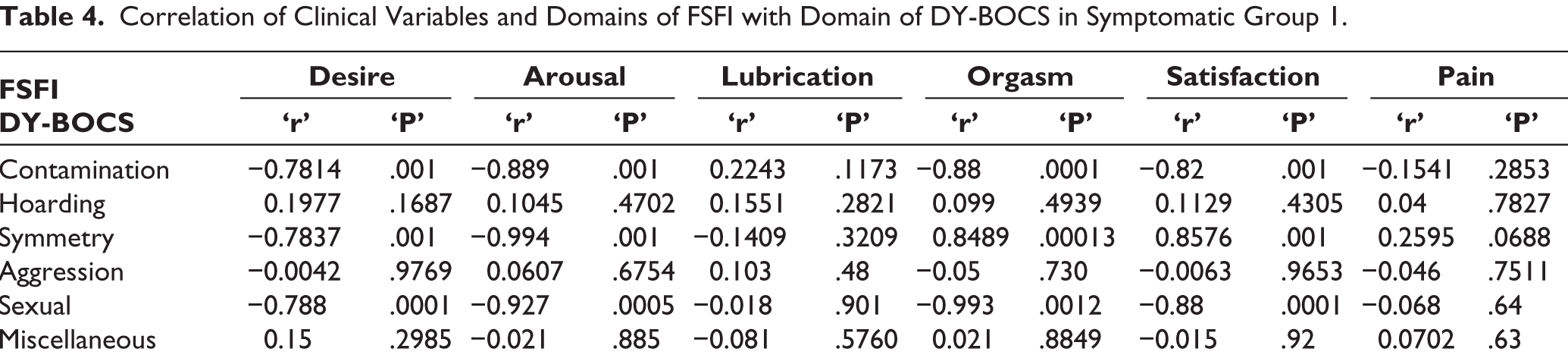
No significant correlation between RAS, FSFI total score and SQOL scores with education, personal income, and family income was found. However, age was found to have a significant negative correlation with FSFI (r = −0.32, P = .023) and SQOL-f (r = −0.35, P < .01). There was no correlation found between RAS and age. There was significant negative correlation was also found between the duration of illness and RAS, FSFI and SQOL-F scores. There was a significant negative correlation also found between the contamination domain of DY-BOCS and with desire, arousal, orgasm, and satisfaction domains of FSFI. There was a significant negative correlation between the symmetry and exactness domain of DY-BOCS and sexual domain of DY-BOCS and the arousal, desire, and orgasm domain of FSFI. There was a significant negative correlation between the sexual domain of DY-BOCS and sexual domain of DY-BOCS and the arousal, desire, and orgasm domain of FSFI (Tables 3 and 4).
Correlation of Socio-demographic and Clinical Variables in Three Groups.
Correlation of Clinical Variables and Domains of FSFI with Domain of DY-BOCS in Symptomatic Group 1.
Correlation of Socio-demographic and Clinical Variables with Intimacy of Relationship, SD, and SQOL in Group 2
No significant correlation of RAS, FSFI total score and SQOL scores with education, personal income, and family income was found. However, age was found to have a significant negative correlation with FSFI (r = −0.36, P < .01) and SQOL-f (r = −0.29, P < .04). There was no correlation found between RAS and age. There was significant negative correlation was also found between the duration of illness and RAS, FSFI and SQOL-F scores. There was no correlation found between the domains of DY-BOCS and FSFI domains.
Discussion
In our study population characteristics of all three groups were similar and comparable with regard to socio-demographic characteristics.
Group 1 consisted of cases that did not receive any pharmacological interventions. Group 2 consisted of cases in remission under pharmacological treatment for at least three months. Three-month remission period for Group 2 was quantified considering that; the response of OCD to pharmacological treatments 33 as well as its side effects mainly sexual side effects may start after 8-12 weeks of starting SSRIs.
As per the cut-off FSFI score (26.55), 68% of cases in Group 1 had SD. This value corroborated with the reported range of SD in female OCD cases in the literature.34,35 60% of cases with OCD under remission receiving SSRI as a pharmacological treatment in Group 2 had SD. This was also comparable to previous studies. 25 Earlier studies have stated that under-reporting of sexual problems in females has been a major area of concern for persisting symptoms. Apprehensive behavior in females experiencing SD adds to the problem further. 36 Most common domains of FSFI observed to be affected in the study individuals are desire, arousal, satisfaction, and orgasm. In a study conducted by Grover et al., 37 91% of patients receiving SSRIs had decreased desire and 60% had decreased arousal. Partial or non-remission of sexual symptoms even after remission of OCD symptoms as well as similar neurobiological mechanisms being determinants of sexual desire and arousal can explain the comparable values of reduced desire and arousal in our study. SSRIs inhibit the nitric oxide synthesis that reduces the vaginal blood flow and reduced lubrication. 38 Dysfunction in the domain of pain could be explained based on desire, arousal and lubrication dysfunction which are determinants of the physical discomfort during any sexual act or intercourse.
Fourteen subjects from the control group had been found to have SD on FSFI. Previous studies suggested the prevalence of 22%-40% dysfunction in the domain of desire 36 and arousal problems in 11%-48% 39 among healthy females.
A significant negative correlation was found between FSFI scores and age as well as the duration of illness, further, it is predicted that even after clinical remission of OCD, significant SD was found. This can be an aftermath of OCD, a chronic course of illness, long-standing stress among family members and partners and antidepressant usage. 37
Our study concluded that SDs were found in about more than 60% of the female cases with symptomatic OCD, and also in those in remission receiving treatment. Reduced desire, delay in arousal, and difficulties achieving orgasm and satisfaction during any intimate sexual activity or during sexual intercourse are all adverse effects of a treatment given, that is, SSRIs can be one of the probable causes of high rates of SD in remitted patients.
Usually, few patients seek medical help for their sexual difficulties during OCD or its treatment. Lack of awareness about sexual difficulties, fear of stigmatization, and a disdain for the pleasures of the female sex can be some of the contributors to poor help-seeking. The clinicians should inquire about the sexual functioning of patients.
Limitations
The sample in our study may not be representative of the actual population of patients having the disease and may only represent those attending the clinical setting; hence more patients should be included, including single subjects and subjects from different cultures for the finding to be more generalizable.
The cause-and-effect relationship could not be established; for which a long-term follow-up study needs to be designed. A comprehensive assessment of spouses could not be done in our study due to resource constraints.
Strength of the Study
To our knowledge, this is the first Indian study on female sexual functioning in OCD patients of both symptomatic and remitted subjects and comparing them with those of healthy adults. Both medicated and un-medicated patients were included along with healthy controls and we attempted to compare sexual functioning in all the groups simultaneously. We tried to exclude all the confounding comorbidities which might have obscured the finding regarding the sexual functioning in females with OCD. Standardized rating scales were used for the assessment of sexual Functions. Additionally, it should be emphasized that the FSFI which is the main diagnostic tool in our study is validated for implementation in Indian contexts. 5
Conclusion
All domains of sexual functioning as measured by the FSFI scale were affected in both groups having drug naïve symptomatic OCD and in cases having OCD in remission with pharmacological treatment for at least three months in comparison to healthy controls. SQOL in cases were also significantly poorer.
There is a need to increase awareness among practicing psychiatrists regarding the increased prevalence of sexual disorders among OCD patients and the need to wisely implement the best therapeutic intervention as per the patient’s requirement. A collaborative approach can be adopted to assess the baseline sexual function in each and every patient with OCD.
Footnotes
Author’s Contribution
Conceptualization: Nirupama Jaiswal, Adarsh Tripathi, Bandna Gupta and Shweta Singh.
Literature search: Nirupama Jaiswal, Adarsh Tripathi, Bandna Gupta.
Data collection: Nirupama Jaiswal.
Analysis: Nirupama Jaiswal, Adarsh Tripathi.
Manuscript writing and editing: Nirupama Jaiswal, Adarsh Tripathi, Bandna Gupta and Shweta Singh.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
The study was approved by the Institutional Ethics Committee of institution vide letter no 542/Ethics/2021 Ref. Code: II PGTSC-IIA/P8.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent
Informed consent was taken from all the subjects. The study was carried out from January 2021 to October 2022.