
Abstract
Background:
Major depressive disorder (MDD) can cause sexual dysfunction (SD), and it is more frequent with antidepressant treatment. Different antidepressant agents have different effects on SD according to their group and dose, which is studied in the present research.
Aims:
(a) To study the prevalence and patterns of SD in male patients with MDD, both drug naïve and on antidepressant treatment. (b) To correlate the severity of depression and SD.
Settings and Design:
Cross-sectional study carried out among 200 patients who attended to the psychiatry outpatient department of a tertiary care hospital.
Materials and Methods:
Every fifth patient with MDD attending to an investigator had been enrolled for the study. Sociodemographic details and clinical variables were obtained. The diagnosis of MDD established by the Diagnostic and Statistical Manual of Mental Disorders, fifth edition, criteria and the Hamilton Depression Rating Scale was used to assess the severity of depression. The Arizona Sexual Experience Scale and Change in Sexual Functioning Questionnaire-14 was applied to measure SD.
Statistical Analysis:
Statistical analysis was done using the χ2 test, unpaired t test, Pearson correlation coefficient, and analysis of variance test.
Results:
Total 82 (41%) patients had SD. Amongst them, 37 (45.12%) patients had the onset of SD before and 45 (54.88%) patients had the onset of SD after treatment. There was a statistically significant correlation between the severity of depression and SD (P = .001), SD responses of patients on the selective serotonin reuptake inhibitor and tricyclic antidepressant (P = .005). Sexual pleasure shows statistical significance with severity (P = .004) and duration of depressive illness (P = .03). The age factor was statistically significant with SD.
Conclusions:
Sexual dysfunction had significance with the severity of depression. Sexual pleasure had significance with severity and duration of depression, and some SD domains had significance with age groups.
Introduction
Sexual behavior is a result of interaction between biology and psychology, which is also an important factor determining a person’s quality of life. In depressed patients, sexual problems are 3 times as frequently as in nondepressed patients and more frequent in patients taking antidepressants.1, 2 It also depends on severity, duration, and recurrence of depression. 3 The sexual side effects vary amongst antidepressants, and they are dose dependent. 4 The study was conducted with the vision that it will help healthcare providers to be more concerned about sexual dysfunction (SD) related to antidepressants and depressive disorders.
Methodology
Aims
The aims of this study are as follows.
To study the prevalence and patterns of SD in male patients with major depressive disorder (MDD), both drug naïve and on antidepressant treatment.
To correlate the severity of depression and SD.
Subjects and Methods
The study was carried out in the psychiatry outpatient department (OPD) of the tertiary care hospital, PDU Government Medical College & Hospital, Rajkot, Gujarat, during the period from June 2017 to May 2018 with the approval of the institute ethical committee. The convenient sample of 200 patients was taken with every fifth patient with MDD attending to an investigator had been enrolled for the study.
Inclusion Criteria
Sexually active male aged between 18 and 65 years.
Men newly diagnosed with MDD as per the Diagnostic and Statistical Manual of Mental Disorders, fifth edition, for the first time as well as previously diagnosed patients.
Patients on antidepressant medication or drug naïve.
Men who had given informed written consent.
Exclusion Criteria
Patients who were suffering from depression along with another psychiatric illness.
Those who were staying with wife or partner but sexually inactive in the past 1 week or having the onset of SD prior to depressive illness.
Patients who were unable to cooperate owing to psychiatric disorder or serious physical illness.
Patient who were not willing to participate in the study.
Patients who did not understand Gujarati, Hindi, or English.
Instrument
The Hamilton Depression Rating (HAM-D) Scale was used to assess the severity of depression. The Arizona Sexual Experience Scale (ASEX) was applied for screening questionnaire to measure sexual functioning. Change in Sexual Functioning Questionnaire-14 (CSFQ-14) was applied to measure major dimensions of male SD. Sociodemographic and clinical data were collected in a uniform and standard manner by using a sociodemographic datasheet. All the collected data were appropriately tabulated, and data were analyzed to find out statistical significance with the help of the chi-square (χ2) test, unpaired t test, and analysis of variance (ANOVA).
Results
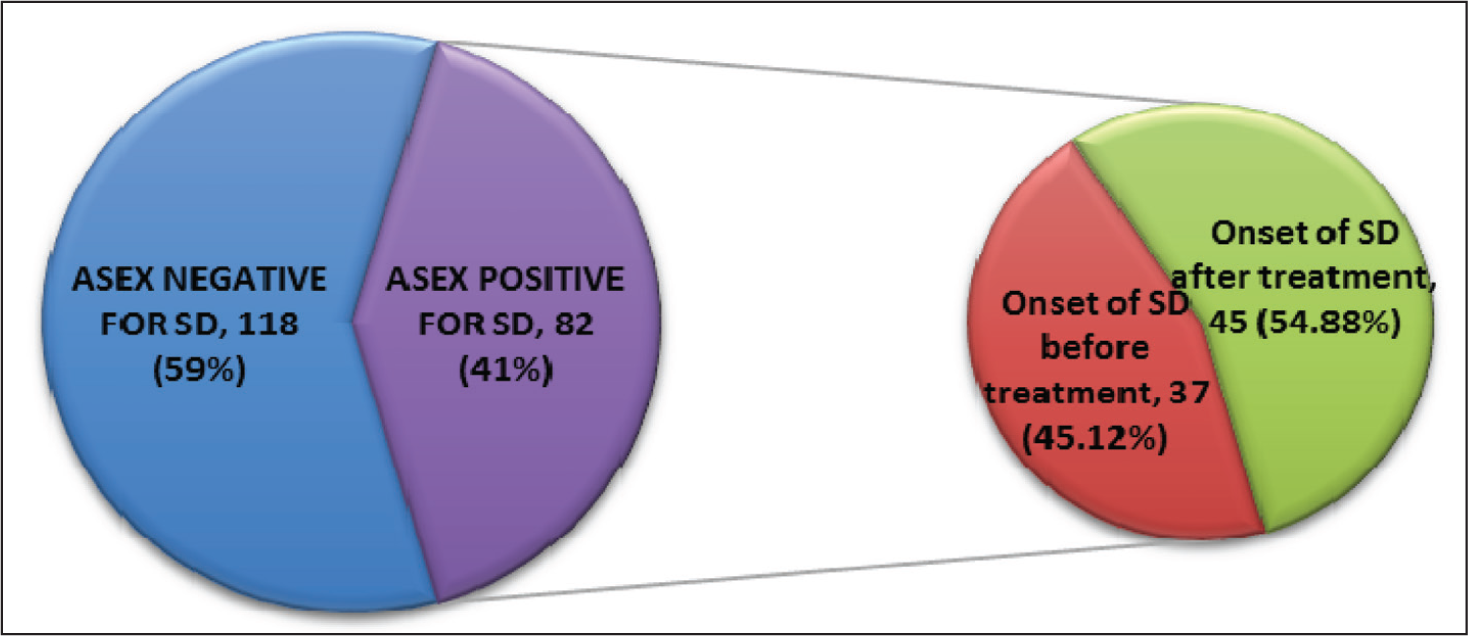
Figure 1 shows the prevalence of SD in patients with MDD. As assessed by ASEX, out of 200 patients suffering from major depression, 82 (41%) patients are having SD and 118 (59%) patients are not having SD. Out of 82 SD positive patients, 37 (45.12%) patients are having the onset of SD before treatment and 45 (54.88%) patients are having the onset of SD after treatment.
Sociodemographic variables related to SD are depicted in Table 1, which shows that out of 82 SD positive patients, 16 (19.51%) patients belong to the 18- to 35-years age group, 44 (53.66%) patients are from the 36- to 55-years age group, and 22 (26.83%) patients are from the 56- to 65-years age groups. This variable is statistically significant (P = .002), whereas rest of the variables are not statistically significant.
Sociodemographic Variables Related to Sexual Dysfunction.
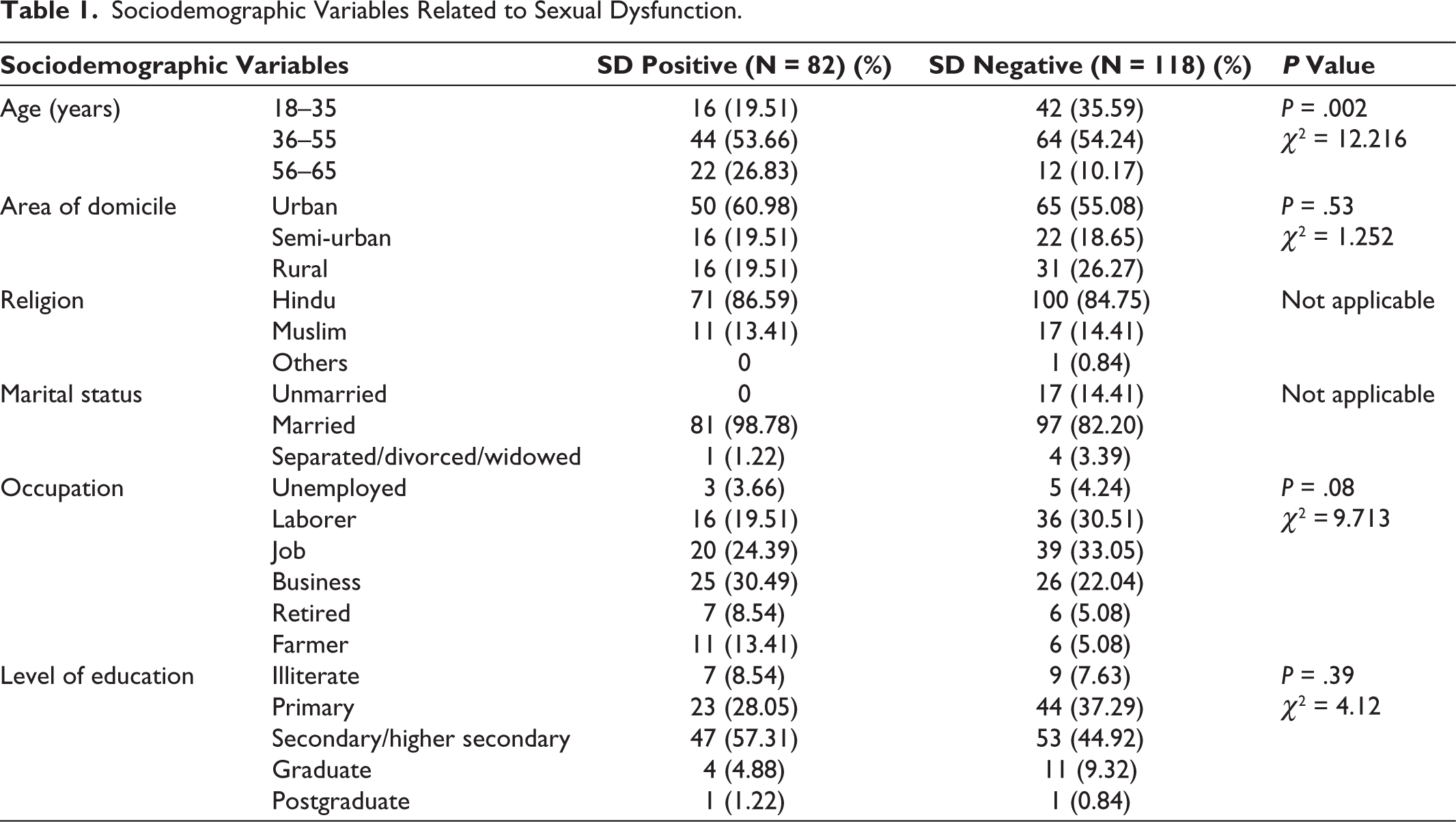
Table 2 shows the relation between the severity of depression and SD. Out of 82 SD positive patients, 38 (46.34%) patients scored normal/in remission (0–7) on the HAM-D Scale, 12 (14.63%) scored as mild depression (8–13), 17 (20.73%) scored as moderate depression (14–18), 8 (9.76%) scored as severe depression (19–22), and 7 (8.54%) scored as very severe depression (≥23). These are statistically significant findings (P = .001).
Relation Between the Severity of Depression and Sexual Dysfunction.

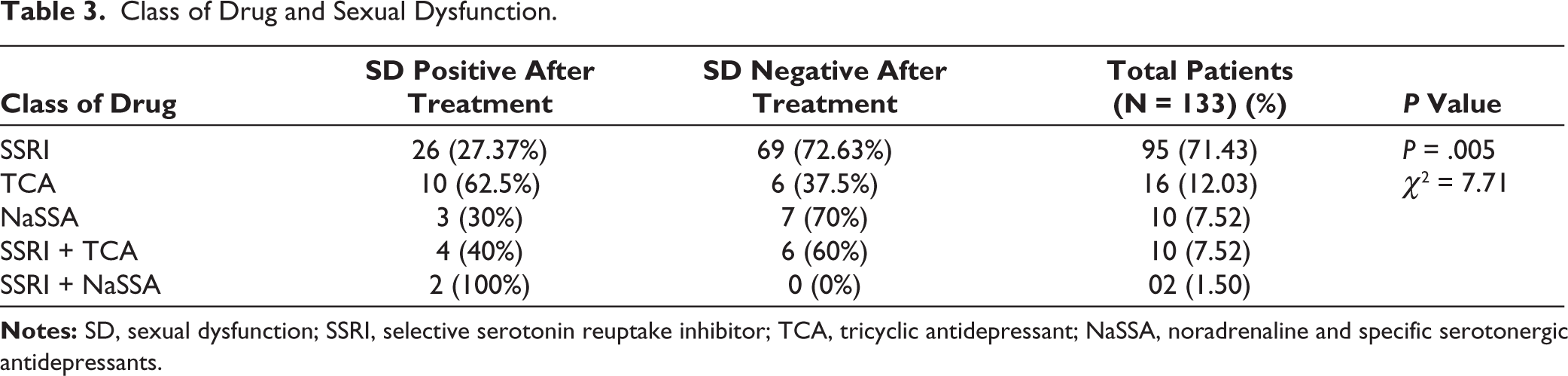
In our sample, we assessed SD after antidepressant treatment. As shown in Table 3, we analyzed total 133 patients who were on antidepressant. Out of 95 (71.43%) patients on the selective serotonin reuptake inhibitor (SSRI), 26 (27.37%) had SD, whereas 69 (72.63%) did not have SD. Total 16 (12.03%) patients were on tricyclic antidepressant (TCA), out of which 10 (62.5%) had SD, whereas 6 (37.5%) did not have SD. There is statistical significance (P = .005) between the SD responses of patients who were on SSRI and TCA. Rests of the SD responses with other class of antidepressants were not statistically significant.
Class of Drug and Sexual Dysfunction.
In the present study, the frequency of SD responses in different domains with respect to the treatment was analyzed. It shows that depressive illness and treatment status both affect all the domains of SD as response noted, but illness affects sexual pleasure and treatment affects sexual orgasm markedly. Unpaired t test was applied for each classified SD, but that is not statistically significant.
The Pearson correlation coefficient was applied to assess whether the frequency of responses in classified SD is affected with HAM-D severity or not, and the ANOVA test was applied to assess statistical significance. The Pearson correlation coefficient for sexual desire/frequency, sexual desire/interest, and sexual pleasure shows a weak negative correlation, whereas that for sexual arousal/excitement, sexual orgasm/completion, and total CSFQ score shows a weak positive correlation. Out of the domains of SD, only sexual pleasure was statistically significant (P = .004) between mild-moderate and moderate-very severe of HAM-D severity.
Out of all patterns of SD, only sexual pleasure shows statistically significant finding over a variable period of duration of depressive illness (P = .03). Rest of the patterns do not show statistical significance over a variable period of duration of depressive illness.
As described in Figure 2, the Pearson correlation coefficient was applied to assess whether the frequency of responses in classified SD is affected with HAM-D severity or not.
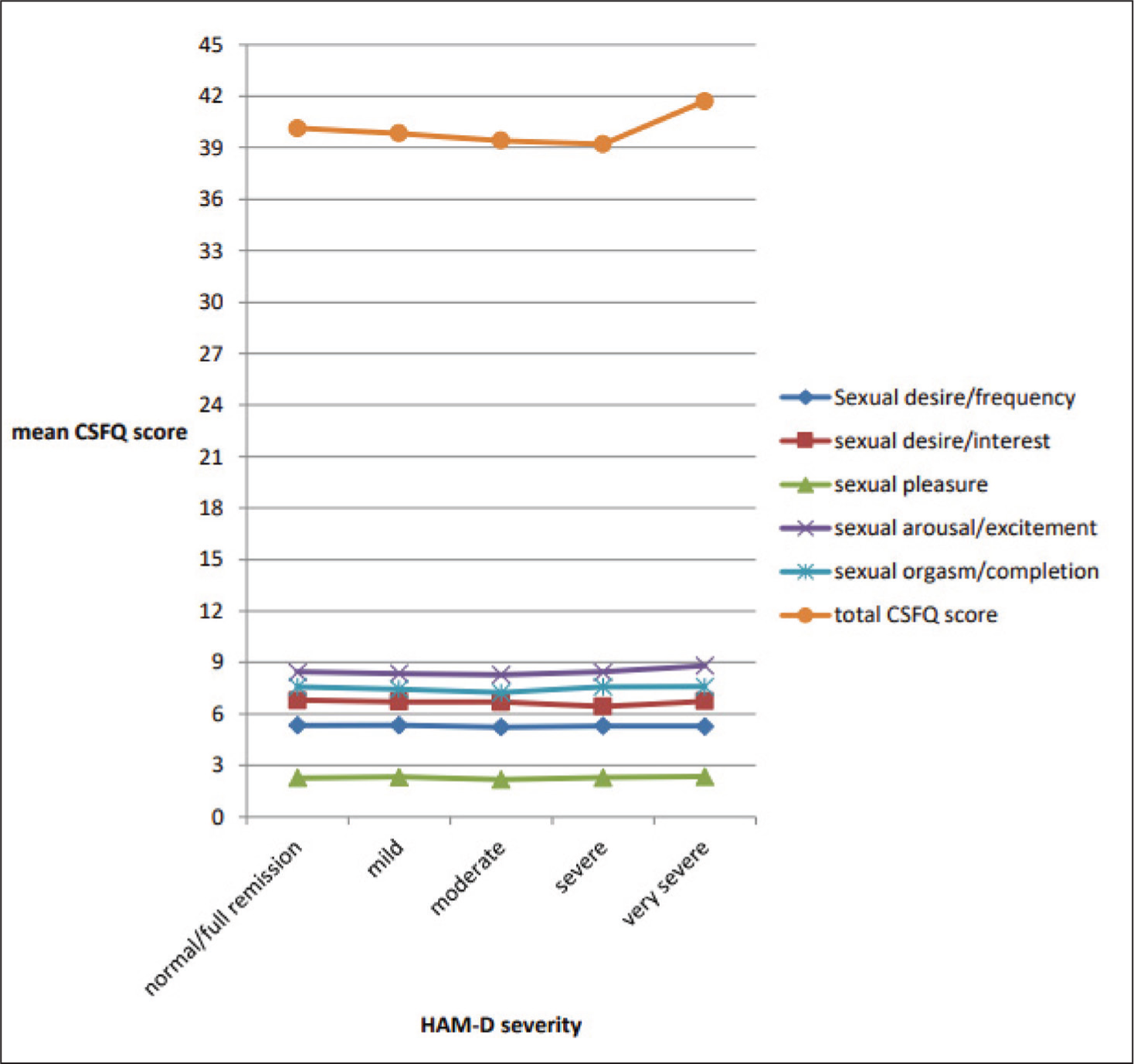
The Pearson correlation coefficient for sexual desire/frequency, sexual desire/interest, and sexual pleasure shows a weak negative correlation, whereas that for sexual arousal/excitement, sexual orgasm/completion, and total CSFQ score shows a weak positive correlation.
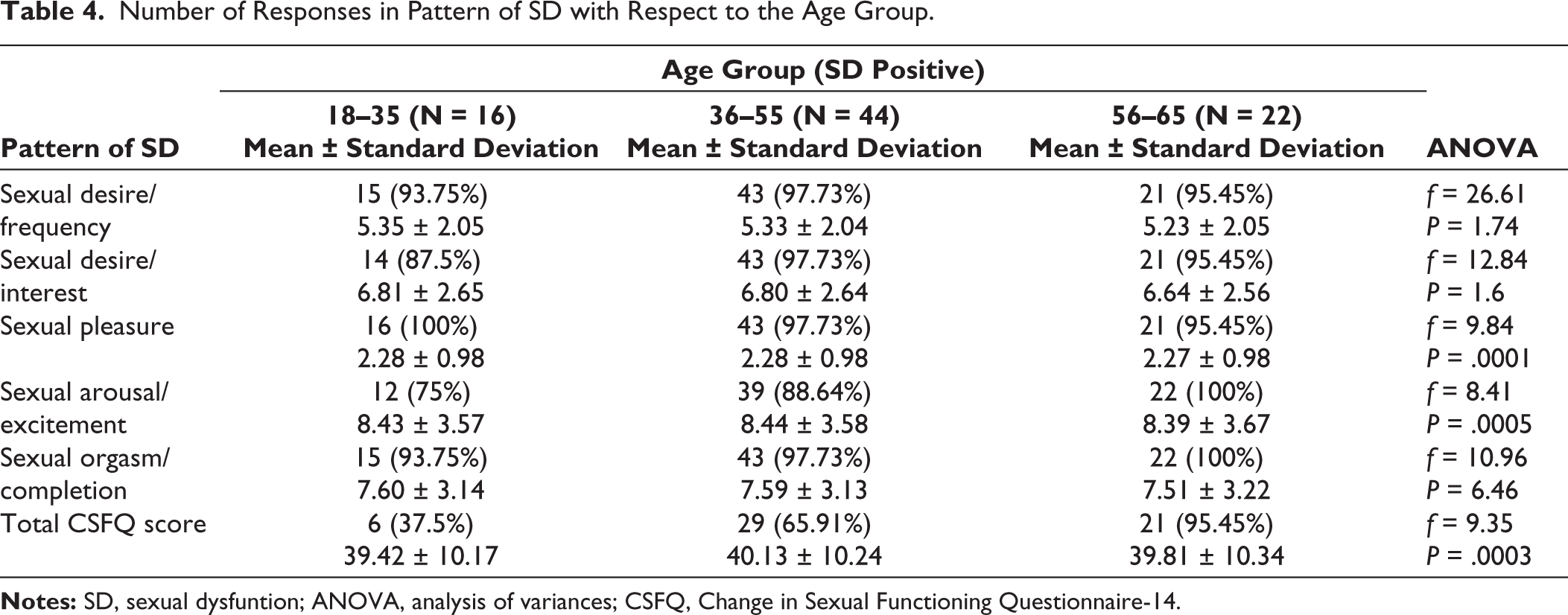
Table 4 shows that there are statistically significant findings for sexual pleasure (P = .0001), sexual arousal/excitement (P = .0005), and total CSFQ score (P = .0003) between the age groups of 18 to 35 years and 56 to 65 years and 36 to 55 years and 56 to 65 years.
Number of Responses in Pattern of SD with Respect to the Age Group.
Discussion
Prevalence of Sexual Dysfunction
We studied the prevalence and pattern of SD in male patients suffering from MDD. Out of 200 patients, we found SD in 82 (41%) patients. Angst (1998) 1 found that the prevalence of sexual problems in depressed subjects—including those with major depression, dysthymia, and recurrent brief depression—is approximately twice than that in controls (50% vs 24%). In our study, out of 82 patients of SD, 37 (45.12%) patients had the onset of SD before treatment started, which may be because of depressive illness, whereas 45 (54.88%) patients had the onset of SD after treatment, which may be attributed to antidepressants. Kennedy et al 5 reported that out of 55 males, 26% (n = 14) reported having no sexual activity over the last month before the start of antidepressant therapy. Somewhat higher prevalence was found in some studies for patients with SD before antidepressant treatment started. One similar study was conducted by Sakhare et al 6 who analyzed 43 newly diagnosed male cases of depression and found that 79% patients had SD, whereas Barot 7 studied 60 drug-naïve patients suffering from depression and found that in patients with depression, SD was reported by 65% of subjects as compared with 29.6% of subjects among healthy individuals.
Sociodemographic Variable in Respect to Sexual Dysfunction
In our study, out of 82 SD positive patients, 16 (19.51%) were from the 18- to 35-years age group, 44 (53.66%) were from the 36- to 55-years age group, and 22 (26.83%) were from the 56- to 65-years age group. This variable is statistically significant (P = .002). We also found that there are statistically significant findings for sexual pleasure (P = .0001), sexual arousal/excitement (P = .0005), and total CSFQ score (P = .0003) between the age groups of 18 to 35 years and 56 to 65 years, and 36 to 55 years and 56 to 65 years. We did not find any statistical significance with respect to other variables, such as the area of domicile, occupation, level of education, type of family, and socioeconomic class. For the religion and marital status, the statistical test was not applicable. Similar to our study finding, Barot 7 reported that the difference of the mean ASEX total score between married and unmarried/widow/separated population and gender-wise comparison was statistically not significant, but there is a statistically significant relation between age and SD in the control group, and in the patients with depression, a fair linear relation was found (r = <50). On the other hand, Matthew and Weinman 8 and Montejo-Gonzalez et al 9 concluded that delayed ejaculation correlated significantly with age (P = < .03) and with significantly older married people, of course; thus, delayed orgasm was more severe in married people (P = .001). Araujo et al 2 noted that the relationship between depressive symptoms and male erectile dysfunction in middle-aged men is robust and independent of important aging and para-aging confounders, such as demographic, anthropometric and lifestyle factors, health status, medication use, and hormones.
Severity of Depression and Sexual Dysfunction
In our study, out of 82 SD positive patients, 38 (46.34%) patients scored normal (0–7) on the HAM-D Scale, 12 (14.63%) scored as having mild depression (8–13), 17 (20.73%) scored as having moderate depression (14–18), 8 (9.76%) scored as having severe depression (19–22), and 7 (8.54%) scored as having very severe depression (≥23). These are statistically significant findings (P = .001). We also found statistical significance for sexual pleasure (P = .004) between mild and moderate depression and between moderate and very severe depression by applying ANOVA. Similar findings were observed in some studies like Thakurta, 10 which found that the mean HAM-D scores were significantly higher in the SD group, and they were positively correlated with total ASEX scores (P < .000), all individual items on the ASEX Scale, and also significantly with the duration of illness (P < .001). Casper et al 11 reported that increasing severity of depression and anxiety was associated with more loss of libido. Bornierbale et al 12 found that the prevalence of SD increased with the severity and duration of the depressive episode (P < .01) in both treated and untreated patients, whereas Sakhare et al 6 and Kennedy et al 5 found no association between the severity of depression and SD.
Pattern of Sexual Dysfunction in Drug Naïve/Onset Before Antidepressant Treatment
In our study, out of 82 patients of SD, 37 (45.12%) patients had the onset of SD before treatment started, which may be because of depressive illness. It shows that depressive illness affects all the domains of SD as response noted. In our study, most frequent responses amongst SD items were in sexual pleasure (100%), whereas in sexual desire/frequency (97.28%), sexual desire/interest (94.59%), sexual arousal/excitement (78.38%), and sexual orgasm/completion (94.59%), and in total CSFQ score (64.86%) responses reported out of 37 patients who had the onset of SD before antidepressant therapy. Similarly, Sakhare et al 6 and Barot 7 also reported that SD was more in patients with depression in all phases of sexual response cycle. Sakhare et al 6 found that 76.74% patients had erectile dysfunction, 55.81% had sexual desire dysfunction, and 53.48% had orgasmic dysfunction, whereas Barot 7 reported that male patients with depression had maximal complaints of low desire (43.7%). Similar findings were observed by Kennedy et al 5 and Matthew and Weinman 8 in which the most frequently reported sexual problem in untreated patients with depression is reduction in sexual desire 42% and 31%, respectively. Angst 1 also noted the same that libido appears to be the core problem with which other sexual problems overlap.
Antidepressants and Sexual Dysfunction
In our study, out of 82 SD positive patients, 45 (54.88%) patients had the onset of SD after treatment started. It was somewhat higher than the onset of SD before treatment, that is, 37 (45.12%). We found statistically significant differences in the SD response between different classes of drugs, such as SSRI and TCA (P = .005), and treatment affects all domains of SD as the response noted. Bornierbale et al 12 also found that the frequency of SD was somewhat higher in patients treated with antidepressants than in untreated patients (71% and 65%, respectively, P < .001). Somewhat similar findings were observed by Chen et al, 13 who studied 125 medicated patients (40 males and 85 females) with major depression using the CSFQ, Taiwanese Depression Questionnaire, and the estimated prevalence rate of SD was 53.6% (95% CI 44.9-62.3%) in medicated patients with major depression, and there were no significant differences in the prevalence rate of SD among different antidepressants, whereas Montejo et al 14 reported that the overall incidence of SD was 59.1% (604/1022) when all antidepressants were considered as a whole and men had a higher frequency of SD (62.4%) than women (56.9%). Balon et al 15 studied 60 patients (22 men and 38 women who were being treated with various antidepressants, and the incidence of SD during antidepressant use in this study was 43.3%. Similar to our study, the SD was not limited to any particular diagnostic group or to any particular antidepressant. Angst 1 reported that sexual problems were more prevalent in the 78 (62%) depressed patients who received treatment than in 122 patients who did not (45).
Duration of Illness and Sexual Dysfunction
In our study, out of all patterns of SD, only sexual pleasure shows statistically significant finding on the application of ANOVA over a variable period of duration of depressive illness (P = .03). Bornierbale et al 12 found that the prevalence of SD increased with the severity and duration of the depressive episode (P < .01) in both treated and untreated patients, whereas Landen et al 16 reported that SD correlated with the duration of the depressive episode, but not with age, dose of SSRI, plasma level of SSRI, duration of SSRI treatment, or any measurement of depression.
Limitations
As this study is a cross-sectional study, the follow-up clinical assessment of each patient was not possible. The prevalence and pattern of SD in our study cannot be generalized as it was done in patients with MDD only. Findings cannot be generalized for the whole community as it was conducted in the psychiatry OPD. Because of the availability of limited drugs in the studied set-up, this study restricts the assessment of SD with all classes of antidepressant drug treatments. The study evaluated SD with respect to the class of drug, that is, SSRI, TCA, etc, so it could not establish the impact of an individual molecule on SD. Some components of the study were related to history taking; therefore, the chances of recall bias are present. The instrument that was used in our study has certain limitations. First, ASEX is a screening instrument and not diagnostic. Second, when ASEX turned to be positive for SD, then only further evaluations about SD were done by using the CSFQ scale; however, if ASEX was not positive, then other patients were excluded from further evaluations even if there might be chances of such patients having SD. The present study is a single-center study. To get more generalized findings, multicentric studies can be planned with a wider sample size.
Conclusion
Out of 200 patients, it was found that 82 (41%) patients had SD, and amongst them, 37 (45.12%) patients had the onset of SD before treatment and 45 (54.88%) had the onset of SD after treatment started. Statistical significance was found between the severity of depression and SD. Also, there was statistical significance between SD responses of patients on SSRI and TCA. Out of all patterns of SD, only sexual pleasure as a response to questionnaire shows statistically significant findings with respect to the severity of depression and over a variable period of duration of depressive illness. Amongst the sociodemographic variables, statistical significance was found between the age variable and SD, and it was also found that there was statistically significant difference for sexual pleasure, sexual arousal/excitement, and total CSFQ score between the age group of 18–35 years and 56–65 years, and 36–55 years and 56–65 years.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
The study was carried out in the psychiatry outpatient department (OPD) of the tertiary care hospital, PDU Government Medical College & Hospital, Rajkot, Gujarat, during the period from June 2017 to May 2018 with the approval of the institute ethical committee.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent
The participant consented to the submission of the article to the journal.