
Abstract
Dhat syndrome is a common semen-loss related physical and psychological distress usually reported by young males. The treatment mainly centres around nonpharmacological strategies such as psychoeducation. Most of the patients present as outpatients to alternative medicine or nonpsychiatry branches and treatment is usually not delivered. Some of the reasons may include perceived need for longer duration of sessions with the patient, available literature with complex psychiatric jargon and barriers to treatment due to stigma attached to psychiatry. This article presents a two session therapy proposal for Dhat syndrome that could be useful as a brief intervention over tele-consultations, and in consultation liaison clinics by nonpsychiatrists as well.
Background
Dhat syndrome is a common presentation in India. 1 It usually presents in young males. 2 They commonly report with multiple nonlocalizing somatic complaints, inability to control nocturnal emissions, self-blame for masturbation, and fatigue with a belief that the cause is related to semen loss. 3 Additionally, they may also complain of symptoms of anxiety, semen loss during urination or defecation, burning sensation at the tip of the penis, sexual difficulties (inadequate or decline in function), scrutiny of genitalia with associated complaints of inadequacy, or deterioration in size and appearance. 4 They may refuse to marry for fear of failure in sex and not unusually attempt to check the level of prowess through illicit encounters (such as commercial sex workers [CSWs]) in a furtive manner that have failed, often because of heightened anxiety, due to fear of failure, fear of discovery, and associated guilt. Some of the commonly held beliefs include that semen is a distillate of blood (and sometimes of brain material) in a ratio of 1:40, and that the volume of semen discharge during sexual intercourse is half of that of discharge during masturbation or nocturnal emissions. 5 Therefore, accordingly, loss of semen would result in progressive, nonreversible damage to the body, and masturbation is harmful than sexual intercourse. 6 These commonly held beliefs as cultural explanations often have immense authority in which these clients view their life and not just sexuality alone.
The clients usually present as outpatients to indigenous practitioners, general medicine, or urology, rather than psychiatry. Most of them have received multiple treatments usually from traditional and alternative medicines before seeking help from modern medicine. 7 Many may have also received significant reinforcement in causal belief by direct validation of belief by friends, relatives, and medical practitioners. Despite Dhat syndrome being well-studied and well-understood with sufficient literature available about approach and treatment, effective treatment is not being delivered for various other reasons. First, modern medicine dismisses the beliefs about semen being a vital fluid and masturbation. 8 Simultaneously, it is unable to provide any symptom relief through any medication. 9 Third, nonpsychiatrists find it difficult to follow the treatment protocols for Dhat syndrome which are time-consuming (often involving several sessions of cognitive-behavioral therapy), requiring a multistep approach and are confusing with psychiatric jargon. 9 Lastly, when referred to psychiatry, they do not follow-up for various reasons including an inadequate understanding of the need for referral, lacking awareness about availability of treatment, and most important the stigma attached to psychiatry. 10
Hence, this article proposes a simple two-session therapy designed by psychiatrists, who commonly encounter Dhat syndrome while working at consultation-liaison psychiatry and have come to understand the felt-needs of both their clients and the referring doctors. This may also be utilized as a briefer intervention considering the increased preference for tele-consultations due to the pandemic. However, it may be noted that this brief therapy proposal can be useful to patients with Dhat syndrome in the absence of other comorbidities and chronicity, but its real-life effectiveness has not been proven. A panoromic view of the proposed sessions is shown in Table 1.
Panoramic View of the Sessions and the Steps Involved
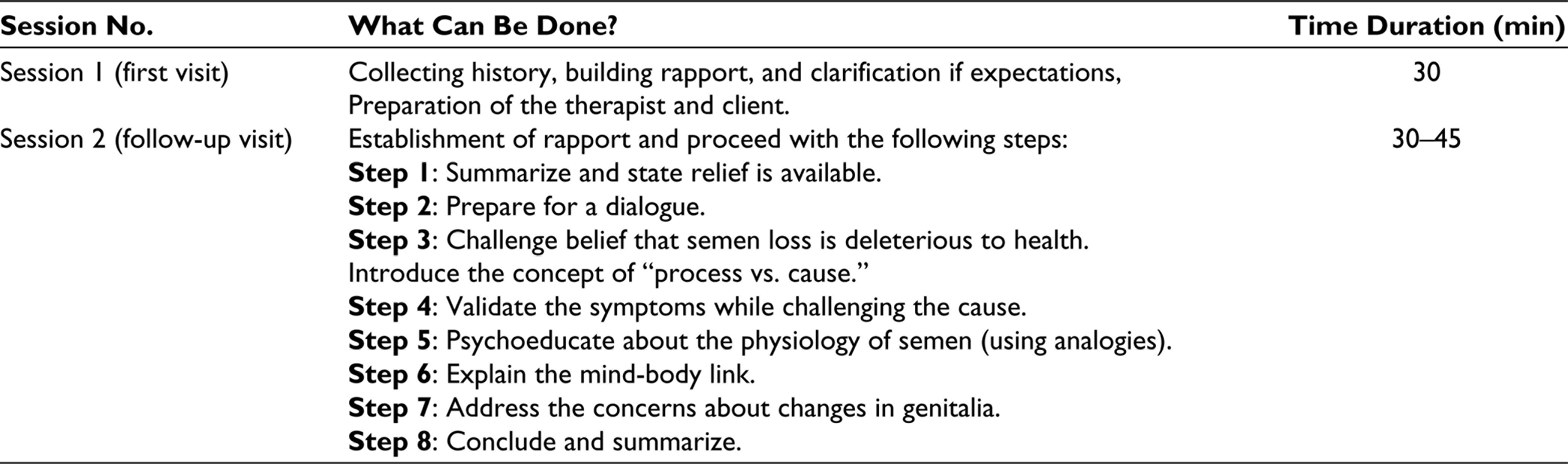
A Two-Session Therapy Proposal
Session 1
Session 1 is being considered as the first visit of the client with symptoms suggestive of Dhat syndrome.
Preparation of the Therapist and Client
Once Dhat syndrome is suspected during this therapeutic evaluation, building a foundation for good rapport becomes most crucial. To achieve this, ask, listen (actively), and document sequence of this individual’s story, covering all aspects of relevant history. This should be done in an unhurried manner, without any attempt to correct, contradict, or challenge any beliefs. To accomplish this, one needs to familiarize oneself with alternative respectful, decent, and nontechnical words for penis, vagina, penetration, semen, masturbation, nocturnal emission, and CSWs, and so on in the language preferred by the client. It is advised to be frank and straightforward in one’s manner of presentation. Especially if the doctor is a female, assure that being a professional, you are comfortable with the area of sexuality and will not be shocked or offended by discussion of sexual matters.
This session can be utilized to review the beliefs held by the client including the comorbidities, expectations of the patient from the treatment, carrying out a physical examination, and need for investigations.
Assessment and Necessary Investigations
A genital examination must be done to ensure that there is no anatomical abnormality. Necessary investigations such as urine and blood examination can be sent to rule out suspected urinary tract infection, and other sexually transmitted diseases (such as chlamydia and gonorrhea).
Reassurance can be provided to the client that there is no reason for worry and treatment is available. A date for review can be given for follow-up.
Session II
Session II can be considered as the follow-up visit after the initial therapeutic and diagnostic evaluation has been done. If sufficient time could not be given during the index visit, ensure that adequate time is allotted for the client during this visit, to ensure building a good rapport.
The following session should be a dialogue. The doctor has to introduce several different concepts that challenge, correct, and provide an alternative model that is both complete and of therapeutic use to the patient. The following steps are based on assumptions that the client can grasp a concept more easily when it is compared to an experience (concept) that he or she is already familiar with and that a question-and-answer format encourages active learning in comparison to being given information in a didactic manner. Questions are indicated as “Q” and expected answers from the client are indicated as “A.”
Based on the understanding of the client, the duration of the session can range from 30 to 45 min and can be done in 8 steps elaborated below with statements to guide the session. They may be modified and used as per the discretion of the treating doctor.
Q: “Is loss of a large volume of blood (eg, 1 L) harmful to health?”
A: “Yes.”
If client replies “no,” patiently mention that human body needs an average of 5 L for vital functions and explain the consequences of loss of large amount of blood. Then, repeat the question.
Q: “Does it matter if the blood loss is after a knife cut or if it is withdrawn using a needle and tubes?”
A: “No.”
If client replies “yes,” attempt to explain why the method of loss of blood (even through semen, if so) would not alter the consequences of blood loss. Then, repeat the question.
Q: “Hence, if semen loss causes weakness, why would married men, who have sex regularly, not get weak?” (Allow time to absorb the logic)
A: The expected answer would be a willingness to accept that the original premise (that semen is made of large volume of blood) is wrong.
Q: “I understand that you have a variety of pains, and I am hopeful that we can find a solution, but the cause is not due to semen loss. Would you agree that the latter is correct?”
A: “Yes.”
If client replies “no,” respectfully attempt to understand their alternative explanation without dismissing them too quickly.
One can clarify the agenda by saying, “Before I talk of why you are having aches and pains, I want to tell you what we know about semen from a doctor’s point of view.”
Q: “What happens when the urine bladder gets full?”
A: “We feel like visiting the toilet.”
Q: “If a toilet is not accessible immediately, can we hold on for a while?”
A: “Yes.”
Sometimes if the client replies “no,” explain that this is not referring to their personal experiences but in general.
Q: “How long can we hold?”
A: “A (finite/certain) period.”
Q: “What happens if we still can’t get to a toilet?”
A: “There will be spontaneous wetting.”
If the client does not spontaneously answer this, try leading them with the question, “Would there be spontaneous wetting?”
Q: “Does the same thing happen when the intestines/feces bag gets full?”
A: “Yes.”
If the client answers “no,” attempt to hand hold them the same way as the spontaneous wetting scenario.
Q: “Is there any harm to the body?”
A: “No.”
If the client answers “no,” mostly client may not have understood or is not following the questions. Can repeat question by asking, “whether loss of urine or feces, voluntarily or involuntarily cause any harm to the body?”
Q: “Can you tell the difference between the urge to pass urine and the need to defecate?”
A: “Yes.”
The doctor can clarify by saying, “A man’s body has a bladder for semen, very similar to that for urine, only smaller. When it gets full, nature wants to expel it just like it wants to expel urine/feces. The sensation that one feels for semen is to have sexual release. This can happen with intercourse or masturbation. (Allow time to absorb information). If neither happens, the semen bag discharges the contents during sleep. This is experienced as night falls. Hence, the popular idea that semen discharge is harmful to health has no medical basis. In fact, it is a normal process that happens to healthy men.”
On a case-by-case basis, a decision can be collaboratively made with the client, whether to continue or plan another, in order to prevent overload of information and to allow time for processing of these concepts. Reassure the client and revise the key points of the previous steps. Ask if they have any doubts regarding them and clarify the same. After this, the doctor can proceed with the following steps.
Q: “All that I have said so far, does not explain why you feel weak and tired, isn’t it?”
A: “No, it doesn’t.”
Q: “Yes, I understand. Let us take a person who is very frightened of snakes. He is walking at dusk and in the dim light, sees a length of rope lying in his path. What can happen?”
A: “He will get frightened.”
Q: “Is it possible that his heart beats fast, that he begins to tremble and sweat?”
A: “Yes.”
Q: “Why does this happen?”
A: “Because he gets scared.”
Q: “He shines a torch and sees that it is only a piece of rope. What happens then?”
A: “He stops being afraid.”
Q: “But does that mean that his raised heart rate, sweating, etc. did not happen?”
A: “No, they did happen.”
Q: “But if the snake wasn’t real, why did those happen?”
A: “It is because of fear.”
Q: “How can the person stop having this reaction?”
A: “By getting rid of the excess fear.”
Continue by saying; “So, if there is a fear sitting in our minds, the body will react even if the danger is not real. (Allow time to absorb)”
Q: “Is it possible that the belief and fear that semen loss is dangerous is affecting your body, even if it is medically normal? So, every time you experience a semen discharge, your fear makes your body weak and shaky?”
A: “Yes, it seems so.”
Q: “I have checked your private parts and find no abnormality. You tell me that you see some changes that worry you. But tell me, which part of your body is the same as it was 10 years ago? Hair? Skin? Stamina?”
A: “All have changed.”
Q: “So, maybe your expectation that these parts will remain unchanged is not correct. Would you agree?”
A: “I agree.”
Reassure by saying, “Whatever you have described are changes that we would expect with time.”
The loss of semen is a normal process and cannot explain the weakness/complaints of the client. The mind-relationship can explain this fear and wrong attribution that has developed over time especially due to cultural beliefs.
Welcome questions and reassure the client with the following:
If you have any doubts about what we have discussed so far, please feel free to ask. Has what we have discussed, apply fully to you or not? If the answer is yes, proceed with the next sentence, else listen and review understanding. What you need to do is empty the baseless fear from your mind—the fear that semen discharge is damaging your body. Will you be able to do that? If you can do that, you can be fully cured, and do not need to come back anymore.
Discussion
The therapeutic armamentarium for the management of Dhat syndrome involves predominantly nonpharmacological strategies such as sex education, relaxation therapy, psychoeducation, culturally informed cognitive behavioral therapy and in few cases, medications.11-13 Although this is mentioned as 2-session intervention, it can be extended to more number of sessions, depending on the ability of the client to progress. The therapist may note that many times, there may also be a need for booster sessions. If the patient does come back to you, it could be taken as an indicator of trust or acceptance of the explanation rather than failure of the brief intervention. In case of dissatisfaction, it may be prudent to utilize the rapport to be refer to a psychiatrist or psychologist for longer therapeutic interventions.
Conclusion
This 2-session therapy proposal can be an effective tool, especially for nonpsychiatrists for addressing clients with Dhat syndrome. It must be kept in mind that the strength of long-standing cultural models, the brevity of contact with the physician, underlying personality factors, and past experiences of shame during sexual acts might lead to failure of this 2-session model and might need sustained psychotherapy. Also, this article mentioned a few examples that may be helpful, the therapist may use other examples or clarifications as per the clients understanding and context. Hence, should the client report dissatisfaction or returns for further help, a referral to psychiatry can be considered for further evaluation and management.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.