
Abstract
Context: As sexual intercourse is a known risk factor for recurrent urinary tract infection (UTI) in women, we decided to evaluate a novel method of sex education using sexually explicit materials (SEM) to reduce the number of recurrences of UTI in sexually active women, when the other preventive measures fail to reduce the number of recurrences of UTI in these women.
Methods: After obtaining written informed consent and ethical committee approval, sexually active women with a single sexual partner, who presented for recurrent symptomatic UTI following sexual intercourse, were included in this study. The absence of recurrence for 6 months, successful postcoital drug prophylaxis, the presence of comorbidities, anatomical abnormalities of the genitourinary tract (GUT), history of instrumentation of GUT, and use of contraception were exclusion criteria. Their demographic profile, socioeconomic status, imaging studies, pre- and post-intervention urine culture profile and pre- and post-intervention sexual practices were recorded. During every visit, all these women along with their male partners were given sex education sessions about healthy sexual practices using SEM. Data is analyzed.
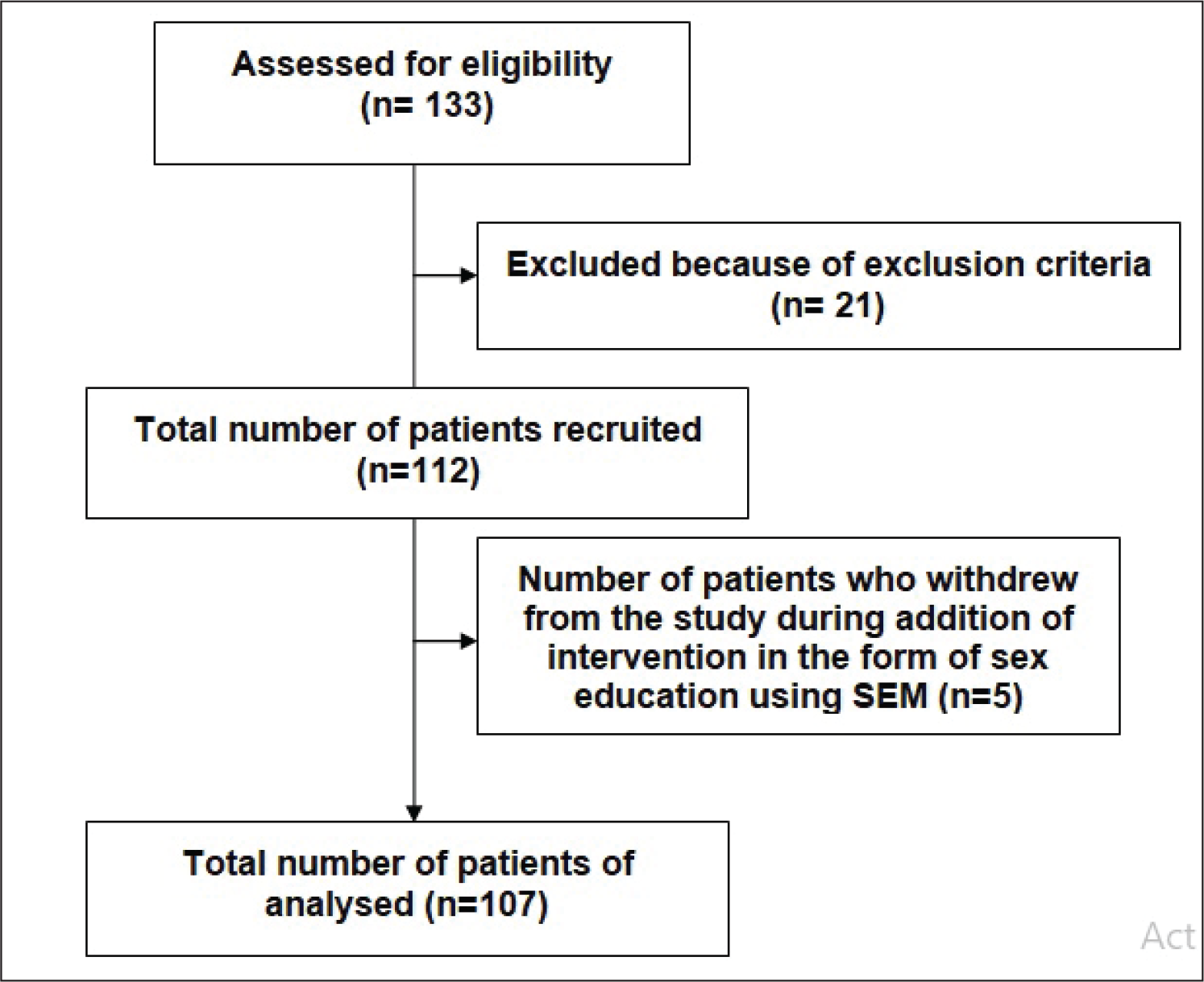
Results: Study period was January 2012 to June 2018. A total of 107 women with the mean age of 30.11 years were included in the study. A total of 82% of UTI were due to Escherichia coli, whereas the other cases were attributable to Klebsiella, Proteus, and Staphylococcus saprophyticus. Their preintervention yearly incidence of documented UTI was 4.04 episodes which reduced to 1.91 episodes post intervention.
Conclusions: Sex education with SEM can be an option to treat recurrent UTI in sexually active women.
Introduction
Urinary tract infection (UTI) is one of the most common causes of morbidity in women. They account for 25% of all the infections in women. 1 Though the recurrence of UTI is more common in women with anatomical abnormalities in the genitourinary system, there are many instances, wherein the women with normal urogenital anatomy suffer from recurrent symptomatic UTI. Recurrence is defined as 3 or more symptomatic UTI in 12 months or 2 or more symptomatic UTI in 6 months. 2 The relationship between the sexual intercourse and recurrent UTI in women is very well established. 3 - 7 As recurrent UTI can cause significant upper tract damage in some women, 1 physician needs to address the issue of recurrence by advising appropriate preventive measures to the patient. Continuous antimicrobial prophylaxis or low dose postcoital antimicrobial prophylaxis have proved to be effective prevention strategies. 2 But there are many instances wherein the women present with recurrent symptomatic UTI following sexual intercourse despite being on these preventive strategies. In such cases, we have used a novel method of sex education using sexually explicit material (SEM) as an educative tool to reduce the number of symptomatic recurrent UTI. SEM is defined as any kind of material aiming at creating or enhancing sexual feelings or thoughts in the recipient and, at the same time, containing explicit exposure and/or descriptions of the genitals and clear and explicit sexual acts such as sexual intercourse, masturbation, bondage, etc. 8 This novel idea of usage of SEM as an educative tool was derived from Rosser et al, who had used SEM for prevention of HIV in men having sex with men (MSM). 9 We are presenting here our experience of the use of SEM as sex education tool in sexually active women who presented with recurrent UTI following sexual intercourse despite being on proven preventive measures.
Materials and Methods
After obtaining written informed consent and institutional review board approval, sexually active women with a single sexual partner presenting to our outpatient department with the recurrent symptomatic UTI following sexual intercourse were included in the study. The participants were followed up for a minimum period of 1 year and maximum period of 6 years.
The exclusion criteria are as follows:
No recurrence of UTI for at least 6 months. Women who were on successful postcoital antimicrobial prophylaxis Women who had associated comorbidities, such as diabetes mellitus, immunodeficiency status, etc. Women with anatomical abnormalities of the genitourinary system. Women with history of instrumentation of genitourinary tract. Women using contraception.
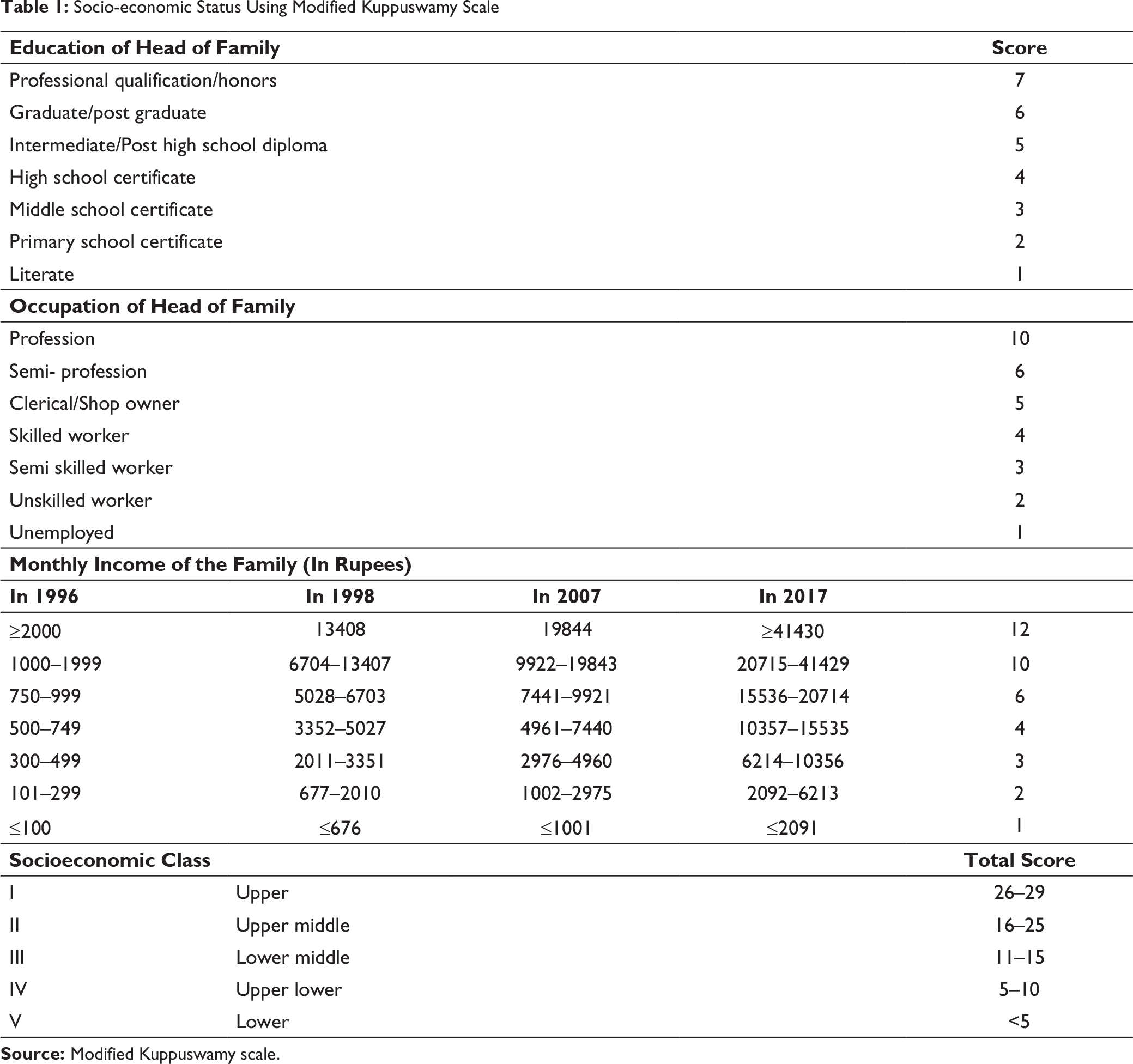
Initially, for the first 1 year, these women were treated with antibiotics alone based on urine culture and sensitivity reports. After this period, another intervention in the form of sex education using SEMs was added along with the antibiotic treatment based on the urine culture and sensitivity report. The participants’ demographic profile, socioeconomic status, urine culture profile during the therapy with antibiotics alone and also during the therapy with antibiotics and sex education, sexual practices during the therapy with antibiotics alone and also during the therapy with antibiotics and sex education, number of recurrences of documented UTI in a calendar year during the therapy with antibiotics alone and also during the therapy with antibiotics and sex education were recorded. The socioeconomic status was calculated based on the modified Kuppuswamy scale. 10
The table for calculation of the socioeconomic status as per the modified Kuppuswamy scale is given in Table 1.
Method of Sex Education Using Sexually Explicit Materials
During every visit, the couples were given sex education using SEMs, which included both audiovisual materials and literature. The literature containing salient points about foreplay, romance, and sexual intercourse from Vatsyayana’s Kamasutra was translated into the couples’ native language. As explained earlier, SEM is defined as any kind of material aiming at creating or enhancing sexual feelings or thoughts in the recipient and, at the same time, containing explicit exposure and/or descriptions of the genitals and clear and explicit sexual acts such as sexual intercourse, masturbation, bondage, etc. 8 Sex education was given in an enclosure that had adequate privacy.
Statistical Analysis
Data was analyzed using GraphPad software (©2018 GraphPad Software Inc., USA). Descriptive statistics, chi-squared, and t test was used to compare the urine culture profile, sexual practices, and number of recurrences during antibiotic therapy alone and therapy with antibiotics and sex education. P value of less than .001 was considered statistically significant.
Results
Socio-economic Status Using Modified Kuppuswamy Scale
Prior to addition of intervention in the form of sex education using SEMs, mean weekly frequency of intercourse was 2.35 ± 1.03. Of the 107 couples, 43% knew about foreplay, but only 20% used them during their sexual intercourse. In total, 35% had knowledge about the cunnilingus, but only 9% used it as a method of foreplay. In total, 17% had knowledge of the oral sex, but only 9% used it during their sexual intercourse. All the couples knew about anal sex and 17% performed it routinely. After the addition of intervention in the form of sex education using SEMs, none of them performed anal sex. Prior to the addition of intervention in the form of sex education using SEMs, 95% of the women reported sexual intercourse as “not so pleasurable.”
After the addition of intervention in the form of sex education using SEMs, the mean weekly frequency of sexual intercourse was reported as 3.52 ± 0.67. All the couples performed adequate foreplay during the sexual intercourse. Oral sex was performed by 82%. In total, 65% performed cunnilingus. None of them performed anal sex. Postintervention in the form of sex education using SEMs, all the women reported sexual intercourse as “very much pleasurable.”
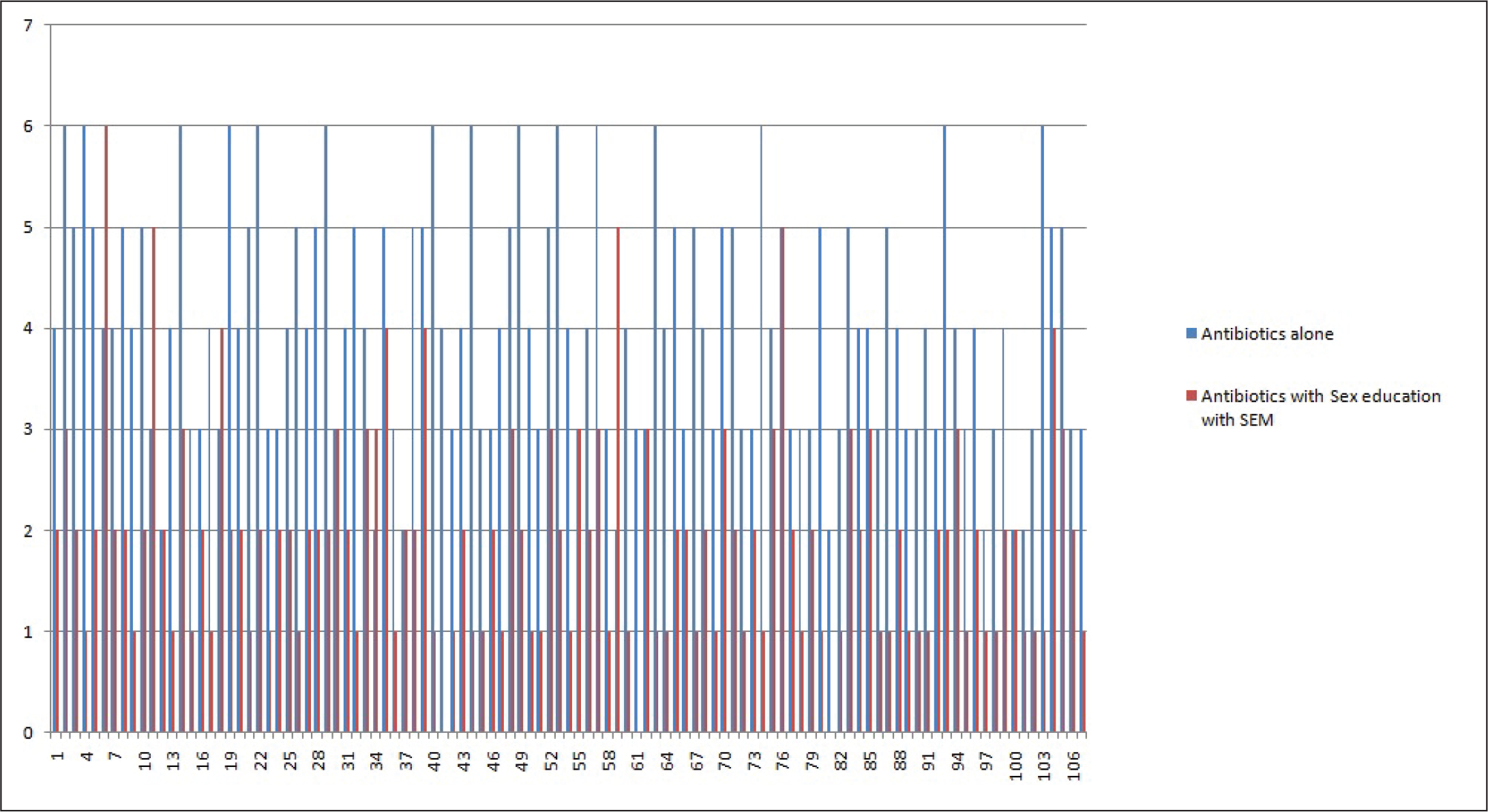
The average number of documented symptomatic UTI in a calendar year, prior to the addition of intervention in the form of sex education using SEMs was 4.04 ± 1.18. After the addition of intervention in the form of sex education using SEMs, the incidence of documented symptomatic UTI reduced to 1.91 ± 1.09 in the study population (Figure 2). The difference was statistically significant at a P value of .001(2-tailed t test). Except in one case, where the intervention failed to make any impact on the incidence of recurrent UTI, in all the other cases, the impact was clearly visible.
Discussion
We are presenting here a comparative study, wherein we have compared the number of recurrences of symptomatic UTI in sexually active women while on antibiotic treatment based on urine culture and also after addition of an intervention in the form of sex education using SEMs along with the antibiotic treatment based on urine culture. The study proved that sex education using SEM containing the audiovisual material and the related literature reduces the number of recurrences of symptomatic UTI in sexually active women, especially when antibiotic alone could not prevent the recurrences.
Incidence of symptomatic UTI is more common in females. UTI in females is known to occur due to bacteremia as a result of colonization of the introital mucosa of the vagina and urethra with Enterobacteria from rectal flora. Sexual intercourse is known to increase the ascent of these bacteria into the urethra and bladder resulting in UTI in females.11, 12 As explained earlier, the sexually active women with a single sexual partner, reporting to our outpatient department with symptomatic recurrent UTI following sexual intercourse, were included in the study. As none of the proven measures could prevent recurrence in these women, we decided to address the issue of sexual intercourse, as sexual intercourse was the most common triggering point in these females.
Formal sex education is not part of the school curriculum in majority of the nations across the globe. 13 Even if sex education is included in the curriculum, most of the times, the information is limited to the contraceptive methods and sexually transmitted diseases.14, 15, 16, 17 Sexuality issues and information related to the sexual intercourse are left unattended. Not much of informal sex education exists within the family as well. 18 Hence, the internet is being used by the men and women to acquire knowledge about the issues related to sexual desire, romance, foreplay, sexual intercourse, etc.19, 20 Most of the unhealthy sexual behavior as well as unhealthy sexual practices are attributable to the audiovisual media available on the internet. 21 However, it is already proved that properly chosen SEM can be used as an educative material. 22 This was shown for the first time in a clinical setting by Rosser et al, when they used SEM for prevention of HIV in men having sex with men. 9
Unlike the orgasm in males, the orgasm in females is not clearly evident. The available literature clearly shows that only 21% to 30% of women experience orgasm during sexual intercourse. 23 Along with the orgasm, plenty of vaginal fluid is secreted, which not only makes the vagina wet but also makes intercourse more pleasurable. Without adequate stimulation, women fail to reach orgasm and hence the sexual intercourse is described as “not so pleasurable.” This fact was clearly evident in our study, wherein majority of the women reported sexual intercourse as “not so pleasurable” prior to the addition of intervention.
Vatsyayana’s Kamasutra is known as the most erotic discourse on sex, sexuality, and romance. 24 We have utilized salient points about foreplay, romance, sexual desire, and sexual intercourse in Vatsyayana’s Kamasutra as literature to inculcate healthy romantic sexual habits in the couples who practiced “not so pleasurable” sex. Along with the literature from Vatsyayana’s Kamasutra, these couples were given sex education with sexually explicit audiovisual material that depicted healthy, romantic sex with adequate foreplay. Postintervention, the couples reported the sex as “very much pleasurable.” This implies that the sexual activity with adequate stimulation of the female partner by the male partner with adequate foreplay resulted in a “very much pleasurable” sex. Adequate stimulation of the female during sexual intercourse results in increased secretion of vaginal fluid. This healthy vaginal fluid acts as a deterrent to recurrence of bacterial UTI, as vaginal fluid is known to exert antimicrobial activity mediated by lactic acid, low pH, and antimicrobial polypeptides.25, 26 We hypothesize that it was this antimicrobial effect of the vaginal fluid that reduced the incidence of recurrences of UTI to such a significant level in our case series.
Sexual intercourse performed without adequate stimulation of the female partner usually results in dry sex, which can injure the introital epithelium and hence endangers the natural defense mechanism of the body against microbial invasion, whereas the intercourse performed with adequate stimulation of the female partner results in adequate lubrication, which prevents damage to the epithelial surface. This also helps in prevention of microbial invasion, thus preventing recurrent UTI. As sex education with SEM helped the couples to perform sex with adequate stimulation, the recurrence of UTI in these women reduced significantly in our cases.
Ours is the first study to use the SEM as an educative tool to reduce the number of recurrences of UTI in sexually active women. We could not conduct a placebo-controlled study in view of the risk of sepsis in the absence of use of antibiotics in a patient with symptomatic UTI. However, the clear and statistically significant decrease in the number of recurrences of UTI in women following sex education sessions using sexually active materials proves the beneficial role of sex education using SEMs in sexually active women.
As per the present understanding, onset of sexual activity is associated with increase in the number of UTI in women. In contrast to the present understanding, we could prove that despite the sexual activity, the number of recurrences of UTI could be reduced, if the sexually active couples are provided with sex education using SEMs, thereby inculcating healthy sexual habits in these couples. This study could form the basis of future research in this direction as it has brought out an important role of sex education using SEMs in reducing the recurrences of UTIs in sexually active women.
Conclusion
Use of SEMs as an educative tool can be a useful method to reduce the number of recurrences of UTIs in sexually active women. Such a method attains significance, especially in cases when the other preventive measures fail to reduce the number of recurrences of UTI in these sexually active women.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.