
Abstract
Symptomatic colon lipoma is a rare occurrence in clinical practice, and its association with sigmoid volvulus is even rarer. We present a case of a man in his 70s who presented to our emergency department with suspected intestinal obstruction. Upon examination, sigmoid volvulus was diagnosed and successfully treated endoscopically through decompression and detorsion. However, the patient experienced a recurrence, leading to the decision to perform sigmoid resection as a Hartmann’s procedure. Subsequently, a prolapsed tumor was observed through the stoma, which was endoscopically resected, revealing a pedunculated submucous colonic lipoma. This case report highlights the potential association between sigmoid volvulus and the presence of a large colon lipoma. Thus, giant colonic lipoma should be considered as a differential diagnosis among the causes of colonic volvulus.
Background
Lipomas are benign tumors that frequently occur in the soft tissues of the human body. While lipomas in the gastrointestinal tract (GIT) are rare, symptomatic variations are even less frequent. Typically, these tumors are located in the submucosa, with muscle layer or serosa involvement being rare. The majority of submucosal lipomas in the GIT occur in the colon (65–75%), with only 25% in the small intestine and sporadically in the stomach. The first colonic lipoma was reported by Bauer in 1757. 1 After Adenomas, colonic lipomas represent the second most common benign tumor with a prevalence that varies between 0.2 and 4.4%. 2 They are usually asymptomatic and found incidentally during colonoscopy, surgery, or autopsy. 3 Lipoma is the most benign tumor causing intussusception of the colon in adults.
Case presentation
A man in his 70s, presented to our emergency department with acute, noticeably distended abdomen and suspicion of intestinal obstruction. Clinically, the patient denied history of abdominal pain, nausea, vomiting, rectal bleeding, changes in bowel habit, or weight loss. The last passage of stool was on the day before. He denied any personal history of malignancy. Abdominal examination revealed diffuse distension with increased tympanic bowel sounds. No tenderness, guarding, or rigidity could be observed. BMI was 31 kg/m2 and he had no clinical history of previous abdominal surgery or colonoscopy.
Investigations
On arrival, the WBC count was normal and the C-reactive protein level was mildly elevated (12 mg/l). Ultrasound of the abdomen was hardly assessable in the presence of massive obesity and meteorism. A plain abdominal radiograph was performed and showed a typical ‘coffee bean sign’ with extensive air filling of the sigmoid colon as well as marked air filling of the ascending colon and transverse colon. The findings were consistent with sigmoid volvulus (Figure 1).
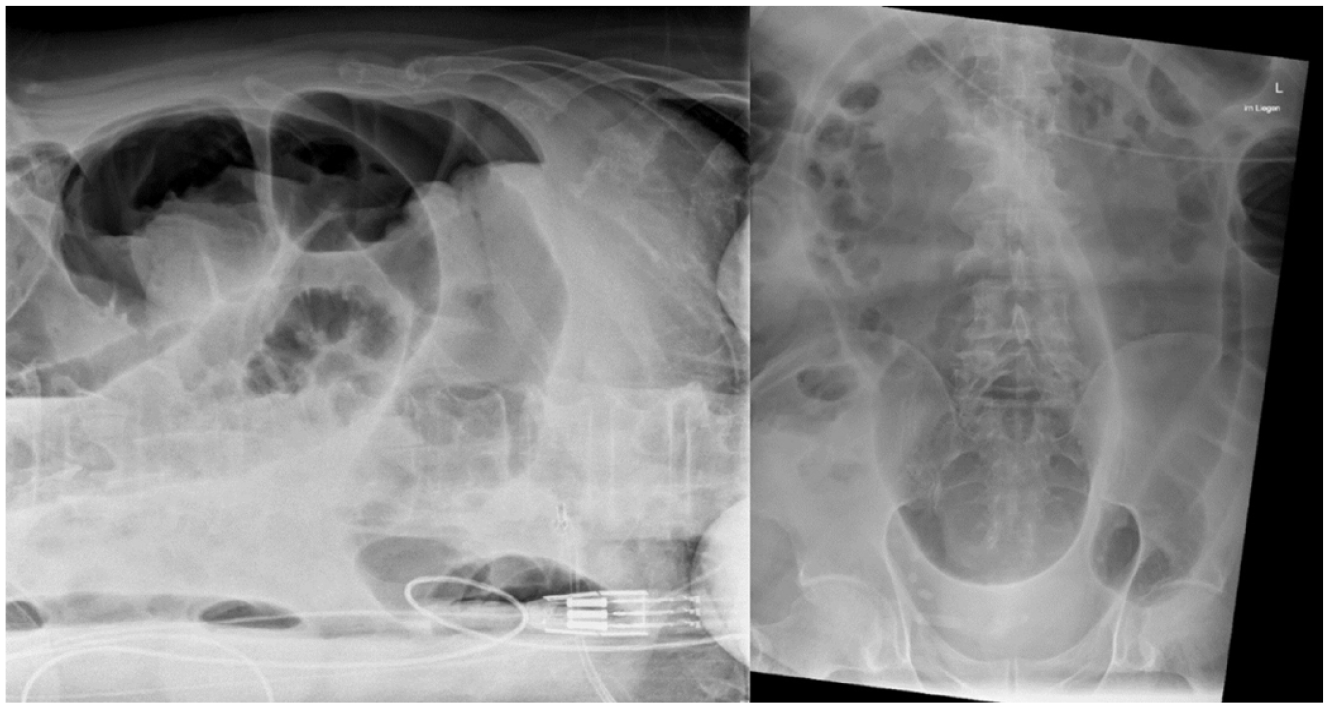
The plain abdominal X-ray shows a typical ‘coffee bean sign’.
Treatment
A colonoscopy up to the distal transverse colon with successful endoscopic detorsion and decompression of the entire colon was performed with the placement of a decompression tube (Figure 2).

Endoscopic detorsion of the sigmoid colon.
After initial clinical improvement over 72 h and removal of the decompression tube, the patient developed clinical and radiological signs of recurrent colonic volvulus. An urgent laparotomy was performed. Intraoperatively, we found a massively dilated Sigma volvulus (12 cm in diameter) without any sign of ischemia. The volvulus was de-rotated and resected as a Hartmann’s procedure. Histopathological examination of the specimen showed a high-grade chronic dilatation of the sigmoid colon, with sclerosing mural edema and hypertrophy of the muscularis propria. There was no evidence of malignancy. On post-op day 1 a prolapsed mass from the colostomy was noted. A colonoscopy via the colostomy under sedation with propofol was performed and revealed a large submucosal pedunculated polypoid mass measuring about 9 × 4 cm, which was located at the transverse colon. Notably, this mass had not been accessible during the initial emergency detorsion procedure. This inaccessibility could be attributed to the marked dilation of the colon, compounded by the presence of liquid and semi-solid stool within its lumen. We chose to perform an endoloop-assisted polypectomy as diagnostic and therapeutic procedure. After submucosal infiltration at the peduncle base with a saline-diluted adrenaline (1:10,000) mix methylene blue, a detachable endoloop (single-use ligating device, HX-400U-30, 30 mm®, Olympus Medical System Corp., Tokyo, Japan) was placed at the peduncle base to ensure hemostasis after resection. A diathermic snare (36 mm oval 2.3 mm–230 cm, Creo Medical GmbH, Germany) was utilized along with the forced COAG setting of 60 watts (Endo-cut Q, Erbe Elektromedizin GmbH, Tübingen, Germany) to sever the stalk 5 mm above the loop and to avoid thermal injury to the colonic wall (Figure 3). The histopathological examination showed a polypoid-structured colon mucosa with a submucosal lipoma and focal erosion (Figure 4). There was no evidence of malignancy or dysplasia.

(a) Giant pedunculated lipoma with about 9 cm long stalk occupying 1/3 of the proximal transverse colon lumen. (b) The stalk appeared to be a continuation of normal mucosa. (c) Mass at the top of stalk: 25 mm erythematous lesion with erosion. (d) Endoloop tightened at the stalk base after submucosal infiltration with saline-diluted adrenaline. (e) Endoloop in place without bleeding at the resection site. (f) Endoscopic image 3 weeks after the resection.

Histopathological feature of the resected specimen showed lipoma (hematoxylin and eosin, original magnification ×20).
Outcome and follow-up
The patient had an uneventful postoperative course and was discharged to rehabilitation facility on the eighth post interventional day. The patient was doing well after 3 weeks with no fresh complaints.
Discussion
Colonic lipomas are tumors that develop in the connective tissue of the intestinal wall and are typically found in the right colon and cecum. 4 They typically manifest as a sessile polypoid mass and are less frequently pedunculated. 5 Colonic lipomas are generally asymptomatic. Lipomas greater than 4 cm are considered giants and more likely to cause intussusception, mucosal ulceration, hemorrhage, and obstruction. 6 Surgical removal is usually preferred when lesions are large and sessile or difficult to distinguish from malignant tumors. 7
For lesions under 2 cm or pedunculated lipomas, endoscopic resection is typically preferred, with various techniques available, including unroofing, dissection-based techniques, endoscopic mucosal resection, and loop-assisted snare resection. 7 The endoloop, which enables endoscopic ligation of the base of an elevated lesion, was first developed by Hachisu in 1991. 8 In recent years, endoloop technique has been described for removal of large colonic lipomas.9 –11
The term ‘volvulus’ comes from the Latin term ‘volvere’ meaning twist. The exact incidence of colonic volvulus remains uncertain. Halabi et al. performed a retrospective review of the Nationwide Inpatient Sample Data between 2002 and 2010 for all colonic volvuli in the United States and indicated that colonic volvulus accounted for approximately 2% of cases admitted with bowel obstructions. 12 It occurs in different parts of the GIT, but in the majority of cases (65–80%) in the sigmoid colon. 13 Having a redundant sigmoid colon with a narrow mesenteric attachment seems to increase the likelihood of developing a sigmoid volvulus. 14 Other risk factors include advanced age, chronic neuropsychiatric conditions, excessive use of laxatives, and persistent constipation. 14 A colonic volvulus is a rare complication of colonic lipomas. Parmar et al. 15 reported a case of submucous lipoma of the ileocecal valve presenting as cecal volvulus. Crocetti et al. 16 published a systematic review describing 184 patients affected with colonic lipomas. Volvulus of the sigmoid colon at presentation was noted in 1% only. Treatment of sigmoid volvulus depends on the clinical presentation and initial paraclinical findings. The ideal strategy for uncomplicated volvulus is an endoscopic detorsion procedure followed by surgery within 2–5 days. 17 A colonoscopy enables the assessment of the sigmoid’s viability and the volvulus detorsion transforming the urgent situation into an elective one. If colonic ischemia is present, immediate surgery is necessary. A colonoscopic detorsion has a success rate of 70–95% with a relatively low complication rate of 4%. 17 A complete colonoscopy before surgery is difficult due to technical challenges. Bowel preparation is often not possible, the colon may be excessively long or have difficult angulations due to the presence of a megacolon. In our case and based on the imaging, endoscopic findings, and the pathological result, we believe that the giant lipoma was the likely cause of the sigmoid volvulus.
Conclusion
Colonic Lipomas > 2 cm can cause intussusception, mucosal ulceration, hemorrhage, and intestinal obstruction.
This case report highlights the potential association between sigmoid volvulus and a large colon lipoma. Thus, giant colonic lipoma should be considered as a differential diagnosis among the causes of colonic volvulus.