
Abstract
Background and aims:
Acute calculous cholecystitis (ACC) represents about one-third of all surgical emergencies. The gold standard management of ACC is laparoscopic cholecystectomy. Although cholecystectomy is a safe procedure, it may be dangerous and contraindicated in patients with complex comorbidities. Endoscopic transpapillary gallbladder stenting (ETGBS) and drainage had been widely used to manage patients suffering from ACC with comorbidities.
Methods:
We searched PubMed, SCOPUS, Web of Science, and Cochrane Library for relevant studies assessing the use of ETGBS in patients suffering from ACC with various comorbidities. Risk of bias assessment was performed using the National Institues of Health (NIH) tool. We included the following outcomes: clinical success, technical success, late complications, and pancreatitis.
Results:
We included seven studies that met our inclusion criteria. We found that the pooled proportion of clinical success, technical success, late complications, and pancreatitis was [91.3%, 95% confidence interval (CI) (86.8%, 95.9%)], [92.8%, 95% CI (89%, 96.5%)], [5.4%, 95% CI (2.9%, 7.9%)], and [3.5%, 95% CI (1.2%, 5.8%)], respectively.
Conclusion:
We found that an ETGBS was an effective and well-tolerated method for the treatment of cholecystitis, especially in high-risk individuals.
Introduction
Acute calculous cholecystitis (ACC) is an acute inflammation of the gallbladder. Gallbladder stones are considered the most common cause of ACC. It represents about one-third of all surgical emergencies. 1 ACC occurs due to blockage of either the gallbladder opening or cystic duct by stones directly or edema that occurs as a result of mucosal ulceration and erosion caused by stones. 2 Patients with cirrhosis are more liable to develop cholelithiasis which may be attributed to gallbladder immobility, the impairment of hepatic transport of bile salts, or hyperbilirubinemia. 3
In 1992, the National Institues of Health (NIH)4 Consensus Development Conference Statement on Gallstones and Laparoscopic Cholecystectomy demonstrated that any patient with symptomatic gallstones should be treated. 5 The gold standard management of ACC is laparoscopic cholecystectomy. 6 Although cholecystectomy is a safe procedure, it may be dangerous and contraindicated in patients with complex comorbidities. A previous study demonstrated that patients with advanced liver disease have more incidence of bleeding and infectious complications of cholecystectomy in addition to the increased risk of adverse events of general anesthesia. 7 Other studies reported that the emergency cholecystectomy mortality rate in critically ill elderly patients may be as high as 30% compared to 0.5% in patients without comorbidities.8 –10 Therefore, surgeons made many attempts to temporarily manage patients with comorbidities with nonsurgical options. These options include dissolution therapy (with either oral or direct contact), extracorporeal shock wave lithotripsy, and percutaneous cholecystectomy with stone removal or drainage in patients without stones.11–14 However, some of these techniques have high morbidity and mortality rates. 15
Therefore, endoscopic transpapillary gallbladder stenting (ETGBS) and drainage had been widely used to manage patients suffering from ACC with comorbidities. A previous systematic review of ETGBS in patients who are not fit for surgery for different causes concluded that about 88% of patients had a significant short-term improvement of symptoms. 16 Other studies assumed that ETGBS may be a viable option for the long-term management of cholelithiasis in patients with liver diseases.15,17,18
We aim in this meta-analysis to evaluate the efficacy and safety of ETGBS for the management of ACC in patients with comorbidities.
Methods
We followed the guidelines of Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) to perform our study. 19
Search strategy
We searched the various databases using the following search strategy: (‘endoscopic stenting’ OR ‘transpapillary stenting’ OR ‘gallbladder stenting’ OR ‘stent’) AND (‘cholecystitis’ OR ‘calculous cholecystitis’ OR ‘gallbladder stones’).
Study selection
The screening was performed in the following steps: First, we imported the studies from research databases to a Microsoft Excel 20 sheet by EndNote Software. 21 Then, we screened the titles and abstracts of the articles presented in the Excel sheet. The last step was the full-text screening of the included studies from the second step.
Eligibility criteria
The inclusion criteria for study selection were as follows:
Study design: We included observational studies and randomized clinical trials and we excluded the other study designs, abstracts, meta-analyses, and reviews.
Participants: Patients suffering from ACC with various comorbidities.
Intervention: Endoscopic stenting of the gallbladder.
Outcomes: Clinical success, technical success, late complications, and pancreatitis.
Data collection
We searched Scopus, Cochrane Library, PubMed, and Web of Science databases till April 2022 for articles that met our eligibility criteria. We collected three groups of data from included studies: the first category is the baseline and demographic characteristics of the included participants, such as the author, year, age, gender, model for end-stage liver disease (MELD) score, Child-Pugh-Turcotte score, and American Society of Anesthesiology (ASA) score. The second category included the primary outcomes for analysis including technical success which was defined as the placement of one end of a pigtail stent into the gallbladder and the other end having been placed through the nose with a nasobiliary tube or within the duodenal lumen, a clinical success which was defined as normalization of the ACC clinical hallmarks, including abdominal pain, fever, and leukocytosis, within 3 days of the intervention, pancreatitis, and late complications included complications >2 weeks after performing endoscopic transpapillary gallbladder drainage. The third category was data of quality assessment.
Risk of bias assessment
We utilized the quality assessment tool from the National Heart, Lung, and Blood Institute (NHLB) to assess the risk of bias in the included observational studies. 22 We attempted to reduce the selection bias as possible by having two blinded authors perform the study selection step. Also, we manually searched all the references in the included studies for the possibility of missing studies.
Statistical analysis
We used Open Meta analyst software to analyze the data retrieved from the included studies. 23 Our study included dichotomous outcomes. We analyzed data using pooled proportion and a 95% confidence interval (CI). The homogeneous data were analyzed using a fixed-effects model, while heterogeneous data were analyzed using a random-effects model. To estimate heterogeneity among data, we used the I2 and the p-value of the chi-squared tests. 24 Values of p < 0.1 were a significant indicator of the presence of heterogeneity. We tried to solve the inconsistency of heterogeneous outcomes using Cochrane’s leave-one-out method. 24
Results
Summary of included studies
We performed a PRISMA that demonstrates our search in the databases (Figure 1). A total of 335 patients indicated to undergo endoscopic stent insertion into the gallbladder were analyzed in our meta-analysis from seven studies.14,16,17,25–28 The mean age of our participants was 59.6 years. The baseline data of our included studies and our participants are demonstrated in Table 1.

PRISMA flow diagram of our literature search.
A summary of the included studies and the demographic data of patients.
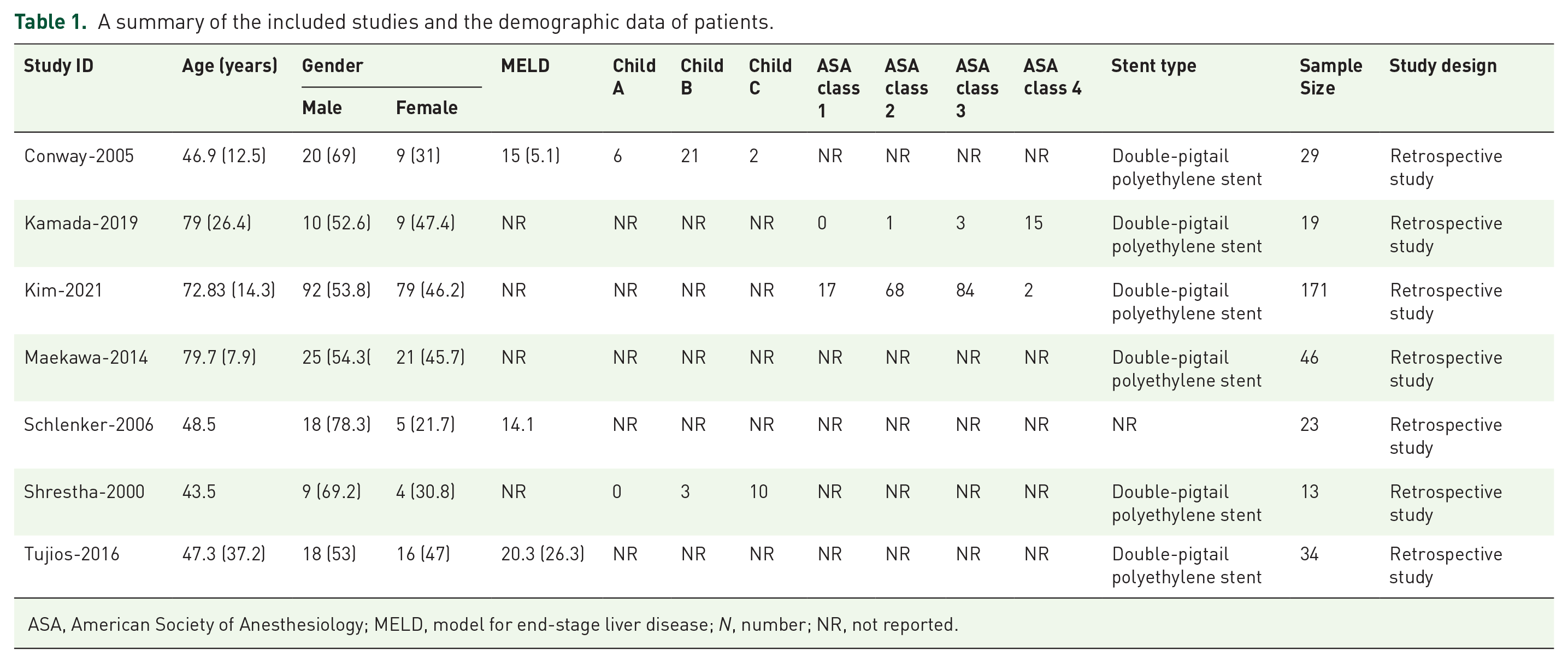
ASA, American Society of Anesthesiology; MELD, model for end-stage liver disease; N, number; NR, not reported.
Results of risk of bias
The quality assessment of our included studies demonstrated an overall score of 10.3 out of 14 according to the NHLB tool of quality assessment. Table 2 demonstrates the details of the quality assessment.
Quality assessment for included retrospective studies.

Key: 1 = Yes, 0 = No.
Not reported.
N/A, not applicable.
Analysis of outcomes
Clinical success rate
All studies15,17,18,25–28 reported this outcome. The pooled proportion was 91.3%, 95% CI (86.8%, 95.9%). Data were heterogeneous (p = 0.058) (I2 = 50.73%) Figure 2(a). We could solve heterogeneity by excluding Maekawa et al. 27 (p = 0.153) (I2 = 37.91%). The overall proportion after solving the heterogeneity was 92.7%, 95% CI (88.6%, 96.9%) Figure 2(b).

Forest plot of clinical success rates. (a) Before leave-out-one, and (b) After leave-out-one.
Technical success rate
Seven studies15,17,18,25–28 reported the technical success rate outcome. The overall proportion was 92.8%, 95% CI (89%, 96.5%). Pooled analysis was homogeneous (p = 0.143) (I2 = 37.38%) (Figure 3).

Forest plot of technical success rates.
Late complications
Late complications outcome was reported in six studies14,16,17,25,27,28. The combined analysis showed that the pooled proportion was 5.4%, 95% CI (2.9%, 7.9%). Pooled data were homogeneous (p = 0.715) (I2 = 0%) (Figure 4).

Forest plot of late complications.
Pancreatitis
A total of 335 patients from seven studies15,17,18,25–28 were analyzed regarding the suffering from pancreatitis. In all, 16 patients had pancreatitis. The pooled proportion was 3.5%, 95% CI (1.2%, 5.8%). The overall analysis was homogenous (p = 0.285) (I2 = 18.96%) (Figure 5).

Forest plot of pancreatitis.
Discussion
In our meta-analysis, we evaluated the efficacy of ETGBS in cases with ACC with various comorbidities. We included 335 patients with ACC with various comorbidities. Regarding efficacy outcomes, out of 335 patients, 299 reported clinical success. The technical success was reported in 304 patients. In terms of safety, only 16 patients suffered from pancreatitis as a consequence of the procedure, and 19 patients reported late complications.
The high rates of morbidity and mortality associated with cholecystectomy in severely ill patients made the nonsurgical treatment critical in such situations29–31
Schlenker et al. 17 performed a retrospective study based on his previous experience that was published in 1999. 15 They found that the cases with liver cirrhosis who underwent ETGBS had reported a resolution of their symptoms. Besides, the procedure was well tolerated and no immediate morbidity had been reported. After the procedure, 39% of the patients underwent successful liver transplantation and 43% were in good condition waiting for the liver transplantation. However, this study is limited by its retrospective design and small sample size.
The transpapillary approach of gallbladder stenting increases the risk of pancreatitis. Besides this procedure requires advanced skills, which makes conservative therapy such as percutaneous transhepatic drainage (PTD) selected as the initial step in the management of acute cholecystitis.32–34 However, PTD is contraindicated in certain situations such as coagulopathy, the results from hepatic impairment, and ascites. Nowadays, the rapid improvement in endoscopic techniques makes transpapillary gallbladder stenting an alternative way of managing acute cholecystitis in such cases. 35
Kamada et al. 26 conclude that ETGBS provides a safe and effective option for managing recurrent cholecystitis in high-risk individuals who cannot undergo cholecystectomy.
Kim et al. 25 estimated the rates of clinical success and technical success of ETGBS. The pooled analysis by the intention-to-treat method showed that the clinical success was 90.1%, and the technical success was 90.6%. These findings were significantly higher than the findings of the previously published evidence, which may be contributed to the experience of the endoscopist and the use of a SpyGlass DS Direct Visualization System (SpyDS). Using SpyDS helps with the detection and advancement of the guidewire. For these reasons, the rates of technical success increased by 4.6%. Finally, they concluded that endoscopic transpapillary gallbladder drainage using either ETGBS or endoscopic naso-gallbladder drainage can be considered a bridge therapy for acute calculus cholecystitis, especially in high-risk individuals.
Shrestha et al. 15 found that from 13 patients with cholecystitis treated with ETGBS, all patients were clinically free for up to 3 years. Seven patients underwent successful liver transplantation, five patients were waiting for liver transplantation, and only one patient died from complications. They concluded that ETGBS is an effective and safe procedure in high-risk populations.
Conway et al. 18 reported that ETGBS was successful in 26 out of 29. The average period of follow-up was 9.8 months. Six patients underwent liver transplantation after the procedure, 14 were alive, and the remaining were awaiting transplantation. The only immediate complication was mild pancreatitis. The late complications were the recurrence of symptoms and death.
Maekawa et al. 28 retrospectively estimated the effect of endoscopic gallbladder stenting on 46 elderly patients aged 65 years. They concluded that ETGBS was an effective option for old patients with acute calculus cholecystitis who are at high risk for operation.
Tujios et al. 27 found that ETGBS was feasible in about 94% of cirrhotic patients and was associated with a significantly low risk of late complications.
Limitation
The main limitation of this paper is the heterogeneity in one outcome, which weakens the certainty of evidence according to GRADE. 36 Another limitation is the lack of a placebo or comparator and the observational nature of some studies.
Conclusion
In our meta-analysis, we found that an ETGBS was an effective and well-tolerated method for the treatment of cholecystitis, especially in high-risk individuals.