
Abstract
Hereditary multiple exostosis has a 3%–5% chance of converting into chondrosarcoma. It is a rare case report of a 32-year-old female with hereditary multiple exostosis who presented with pain and progressive swelling over her right chest wall for 3 months. A clinical examination revealed a large globular swelling over her right chest. Imaging revealed a large, ill-defined, aggressive, and exophytic lesion with a thick cartilage cap arising from the 8th rib. The lesion was hypermetabolic and avid on PET CT scan. She underwent a core needle biopsy which showed features of malignant transformation. En-bloc resection of the tumor with 7, 8, and 9 ribs followed by plate and mesh reconstruction was carried out.
Introduction
Chondrosarcoma affecting the ribs is a rare cancer with an incidence of 0.5 cases per million people annually. 1 These tumors grow slowly and can originate spontaneously or from existing osteochondromas. 2 Typically, they are located in the anterior part of the chest wall, such as the costochondral junction or sternum, and makeup about 20% of all chest wall malignancies. 3 The prevalence is higher in individuals between their fifth and sixth decades of life, slightly favoring males. 4 Treatment of chondrosarcoma involves surgical removal with wide margins due to its resistance to chemotherapy and radiotherapy. 5 However, excising this tumor from the chest wall presents challenges due to its proximity to crucial neurovascular structures, and incomplete removal can lead to an increased chance of recurrence. Managing chondrosarcoma of the chest requires a collaborative effort involving multiple medical specialties.
Case Report
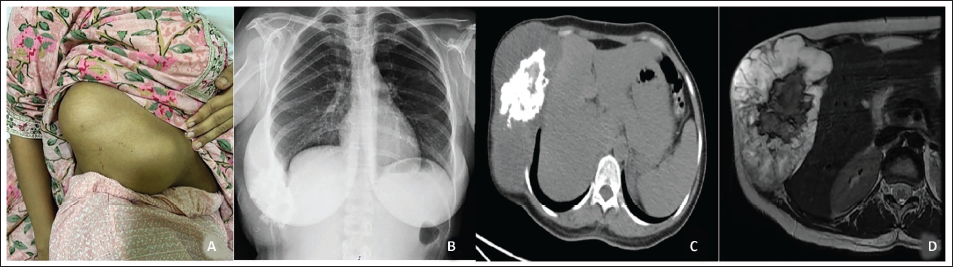
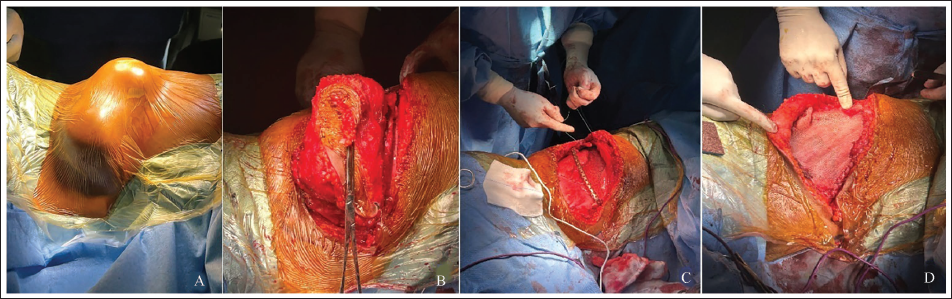
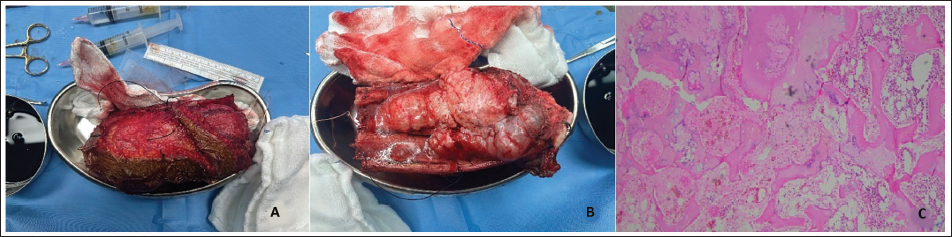
A 32-year-old female who is a known case of hereditary multiple exostosis presented to our clinic with complaints of pain and progressive swelling over her right chest of 3 months duration (Figure 1). Clinically, the swelling is an ill-defined, lobulated, tender, nonmobile, bony hard swelling over the right lower chest wall with an irregular surface, stretched, and shiny skin overlying it (Figure 2A). Plain radiography of chest showed an ill-defined, lytic, exophytic lesion arising from the eighth rib with periosteal elevation, a wide zone of transition, and irregular calcification in the matrix suggestive of an aggressive chondroid lesion (Figure 2B). MRI revealed an irregular, chondroid lesion with involving the right 8th rib near the costochondral junction with an associated extraosseous soft tissue component and cartilage cap thickness of 6 cm, abutting the right 7th and 9th ribs and compressing the right lobe of the liver and the right lung lower lobe suggestive of malignant transformation of an osteochondroma (Figure 2D). PET CT showed avidity in the rib lesion with all other exostoses being nonavid (Figure 2C). She underwent a core needle biopsy under ultrasound guidance, which showed a chondroid tumor with cellular atypia. She underwent wide en-bloc resection of the tumor with 7, 8, and 9 ribs followed by reconstruction of the chest wall defect with titanium plate and polypropylene mesh (Figure 3). The histopathology of excised specimen confirmed malignant transformation to low-grade chondrosarcoma with negative, tumor-free surgical margins (Figure 4). At 18 months follow-up, she is asymptomatic and on active surveillance.
(A) X-ray of Bilateral Forearm Showing Osteochondroma. (B) AP View of Bilateral Leg Showing Osteochondroma. (C) Lateral X-ray of Bilateral Leg Showing Osteochondroma. (D) X-ray Pelvis AP with Bilateral Hip Showing Osteochondroma.

(A) Clinical Picture of Right Chest Wall Showing Swelling. (B) X-ray of Chest Showing Swelling in the Right Lower Ribs. (C) CT of the Rib Showing Swelling of Ribs. (D) MRI of the Rib Showing Cartilage Cap.
(A) Preoperative Photograph Showing Swelling from Right Ribs. (B) Intraoperative Photograph After Intraoperative Wide Local Excision. (C) Intraoperative Photograph Showing Titanium Plate Implantation. (D) Intraoperative Image After Reconstructing with Polypropylene Mesh.
(A, B) Intraoperative Images After Resection of the Tumor. (C) Histological Images Showing Chondrosarcoma.
Discussion
Chondrosarcoma is the second most common primary malignant tumor of the bone after osteosarcoma. 6 Chondrosarcoma can occur denovo or with preexisting multiple exostoses. 7 Chondrosarcoma mainly involves the appendicular skeleton, even though involvement of axial Skeltons is described. 8 Chest wall involvement is in the anterior chest wall at the area of the costochondral junction and in the superior ribs. 3
Various varieties of chondrosarcoma have been described. 9 The most common form of chondrosarcoma is primary chondrosarcoma, which includes conventional (the most common), mesenchymal, dedifferentiated, and clear cell variants. 9 A total of 12% of chondrosarcoma can arise as secondary chondrosarcoma. 10 The preexisting lesions with a risk of chondrosarcomas include solitary osteochondroma, multiple osteochondroma, Olliers disease, Maffucci disease, fibrous dysplasia, synovial chondromatosis, Paget’s disease, and irradiated bone. 11
The grading of chondrosarcoma has an important role in the treatment and prognosis of individuals. 10 WHO has divided chondrosarcoma into three grades, which take into consideration cellularity, nuclear atypia, and mitosis. 10 Further grade 1 chondrosarcoma of the appendicular skeleton is called an atypical cartilaginous tumor, which has a better prognosis than its axial counterpart. 10 Apart from EXT mutations, certain molecular genes like Indian hedgehog genes, isocitrate dehydrogenase enzyme mutations, m-TOR pathways, and PI3K-AKT pathways have been demonstrated, which may aid in targeted therapy in the future.12–14
Chondrosarcoma is both chemo- and radioresistant, which makes surgical management the keystone of treatment. 5 Hence, each patient requires a tailored treatment plan based on the location, grade of tumor, proximity to neurovascular structures, and presence of metastasis. 15 Wide local excision is the gold standard treatment in the management of chondrosarcoma. 16 Obtaining a negative margin is an important modifiable factor in the management of chondrosarcoma, as positive margins are associated with increased recurrence rates and fatalities. 17 With the advent of advanced implants, there is a paradigm shift towards limb salvage surgery rather than amputation, which has similar patient survival and increased functional outcomes. 18
Various approaches exist to address the chest wall defect resulting from extensive local excision. Smaller defects that are less than 5 cm or those situated around the scapular area can typically be handled through conservative measures. 3 However, larger defects exceeding 5 cm or those covering the cardiac region necessitate reconstruction due to their interference with cardiorespiratory function. 5 Reconstruction of these larger defects commonly involves the use of materials like polypropylene and polytetrafluoroethylene, which facilitate the ingrowth of soft tissue. 19 Limited case reports are available for the management of chondrosarcoma of the ribs, and all cases were managed by means of wide local excision and reconstruction of defects based on the size of the defect, just as in our case report.1, 3, 5
Conclusion
The incidence of malignant transformation of osteochondroma. HME is 3%–5%. The diagnosis is made when there are suspicious clinical or radiological features. Such features include sudden progressive increase in size of the lesion, associated symptoms, signs of aggressiveness on imaging, and cartilage cap thickness beyond 2 cm. Confirmation is made on histopathology, which shows marked atypia, myxoid changes, and infiltrative growth pattern. Wide surgical resection with negative margins is the mainstay of treatment. Long-term active surveillance is mandatory to detect recurrences.
Footnotes
Author Contribution
Abin Mohammed prepared the manuscript. Hari S. Nair and Ebin Rahman reviewed the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.