
Abstract
Palpable breast mass is rare in infants and toddlers, which are mostly fibroadenoma (FA). As per English literature, to the best of our knowledge, only three cases of juvenile FA in toddlers have been reported (at ages 13, 16, and 17 months). We present a case of a 16-month-old female child, with a unilateral breast mass of size 5 × 5 cm2, diagnosed as juvenile fibroadenoma (JFA) with micropapillary hyperplasia, exhibiting gynecomastoid morphology. JFA are known to depict an immunoprofile similar to that seen in gynecomastia, with typical three-layered ductal lining (two basal layers and one luminal layer). Giant JFA must be distinguished from phyllodes tumors, virginal hypertrophy, and malignancy. Treatment of JFA includes either excision or observation; large-sized FA may require reconstructive techniques to maintain symmetrical breasts.
Introduction
Fibroadenomas (FA) are rarely seen in young infants and can be of concern to the parents as well as treating clinicians. These can be challenging to diagnose when showing significant papillary proliferation. We report a rare case of juvenile FA (JFA), fourth as per the literature of previously reported cases.
Case Report
We present a case of a 16-month-old female child, with right breast swelling noticed by parents since 7-10 days, showing insidious onset but progressive increase in size. There was no associated fever or weight loss or any other swelling elsewhere in body.
On examination, the right breast showed a 5 × 5 cm2 well-defined non-tender, firm, and mobile mass, soft in consistency, causing stretched overlying skin with visible veins and without any erythema. The nipple areola complex was normal, and no axillary lymph node enlargement was seen. The left side breast was normal for age, and the systemic examination was normal.
The child is the second of twins, born via in-vitro fertilization and delivered preterm at 33 weeks by caesarean section, with birth weight of 1.9 kg. The child achieved normal milestones. Mother did not have any history of hormonal intake during or prior to pregnancy.
Biochemical investigations including serum LH, FSH, estradiol, and thyroid function tests were within normal range.
On ultrasonogram, right breast showed well-defined lobulated heteroechoic lesion measuring 4.1 × 1.6 × 3.3 cm3, radiologically diagnosed as FA. There was no evidence of calcification, asymmetry, or skin thickening, and nipple areola was unremarkable (BIRADS II).
Fine needle aspiration cytology (FNAC) from the lesion showed features of benign breast disease likely FA. The child underwent excision of the nodule, which grossly was well circumscribed and measured 4 × 2.5 × 2 cm3. Outer surface was smooth with a thin capsule, and cut surface was grey white and vaguely lobulated, with few slit-like areas.
Microscopic examination revealed a well-circumscribed biphasic tumor with proliferation of both glandular and stromal elements. The dilated ductal component shows a pericanalicular pattern, with florid hyperplasia, pseudostratification, and micropapillary hyperplasia. Floating micropapillary structures were also seen within the duct lumen (Figures 1 and 2).
Sections Showing a Well Circumscribed Biphasic Tumor with Proliferation of Both Glandular and Stromal Elements.
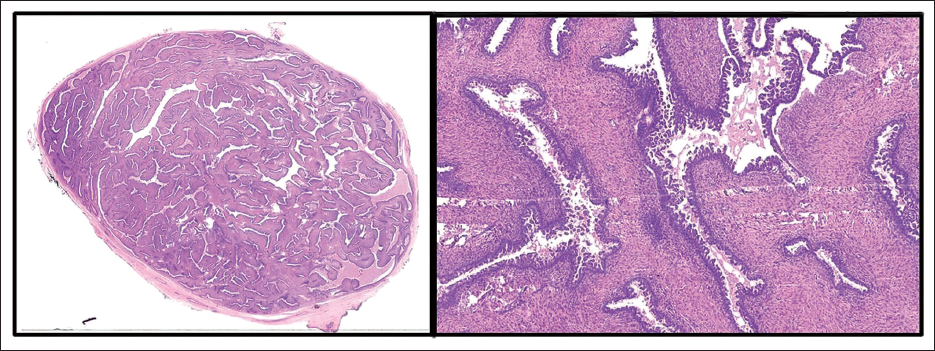
(a) Dilated Duct Showing Pericanalicular Pattern, with Florid Hyperplasia, Pseudostratification and Micropapillary Hyperplasia. (b–d) Floating Micropapillary Structures also Seen Within the Duct Lumen. The Cells Are Round to Oval with Vesicular Chromatin, Inconspicuous Nucleoli and Moderate Cytoplasm.
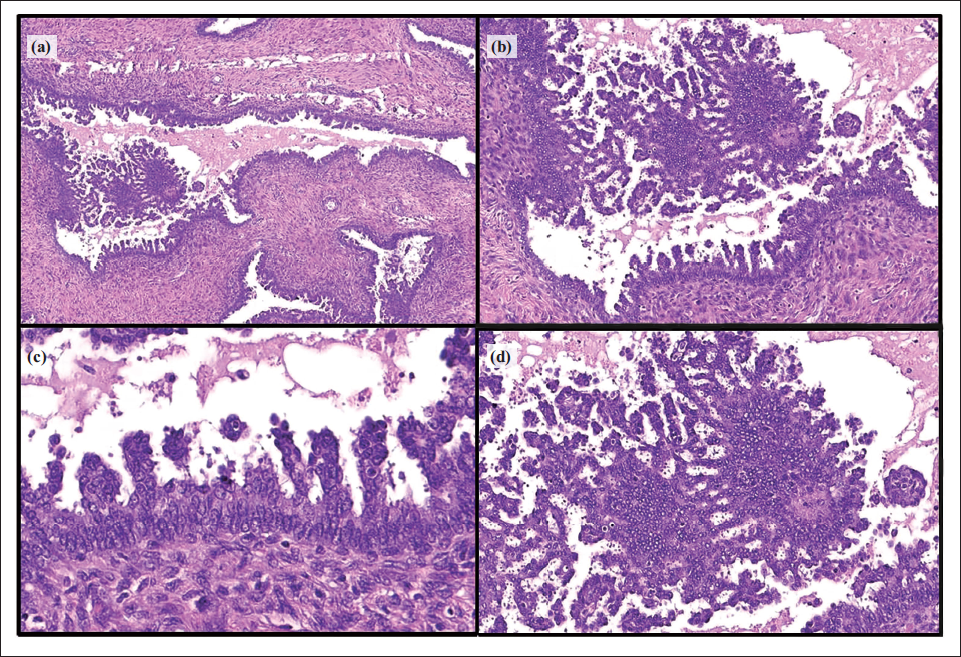
The cells were round to oval with uniform nuclei having dispersed vesicular chromatin, inconspicuous nucleoli, and moderate cytoplasm. Intervening stroma was cellular. Focal leaf-like structure was seen, however, no evidence of stromal overgrowth was seen. No definite nuclear atypia or pleomorphism was seen. No significant mitotic activity or any necrosis was seen.
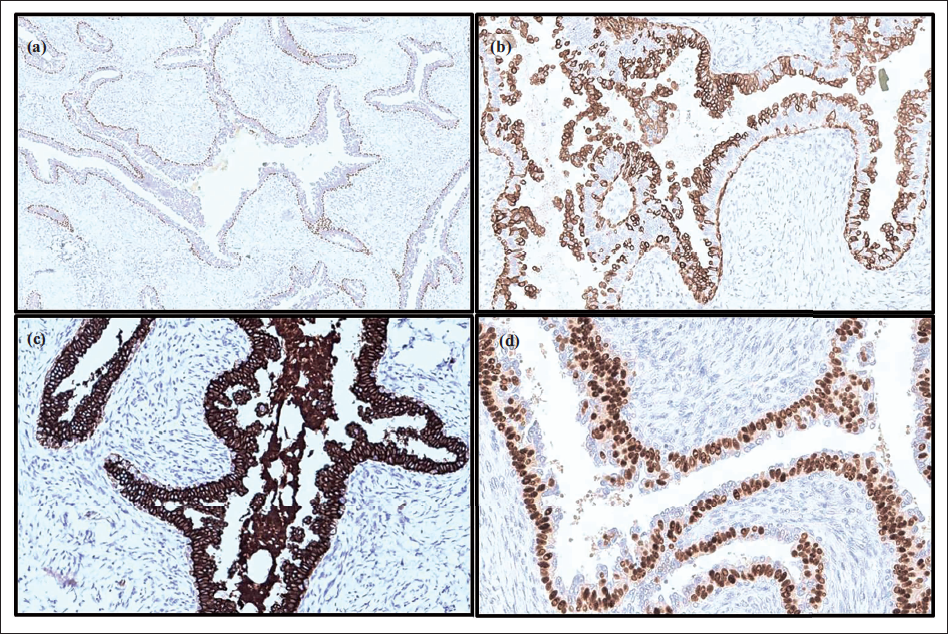
On immunohistochemistry (IHC), p63 highlighted the intact myoepithelial layer around all ducts, and ER expression was seen in the basal layer. CK5/6 expression was seen in basal cells as well as surface hyperplastic cells, and the intervening cell layer was diffusely positive for CK7, confirming the triple cell layer of duct lining (Figure 3). Ki67 proliferative index was insignificant. A final diagnosis of JFA with micropapillary hyperplasia was given.
Images of Immunohistochemistry: (a) p63 Highlights the Intact Myoepithelial Layer; (b) CK5/6 Expression Seen in Basal Cells and Surface Hyperplastic Cells; (c) Intervening Cell Layer Is Diffusely Positive for CK7; and (d) ER Expression Seen in Basal Layer.
Discussion
Palpable breast mass is very uncommon in young patients and rare in infants and toddlers. 1 Unilateral breast masses in adolescent girls and women aged < 35 years are mostly FA. FAs are well-circumscribed benign breast tumors originating from terminal duct lobular units and are most frequent benign tumors of breast, after fibrocystic disease.1, 2
FAs present as painless, solitary, firm, slow-growing, mobile, well-defined nodules, and JFAs comprise 0.5% to 4% of all FA.1, 2
Exact etiology of FA is still not known; however, excess of estrogen, increased estrogen receptor sensitivity, or decreased estrogen antagonist sensitivity are said to be the major cause, leading to premature thelarche and precocious puberty.1, 3
In neonates, postulated effect of maternal estrogen is considered a causative agent; however, in the presented case mother gave no history of hormonal therapy. 4
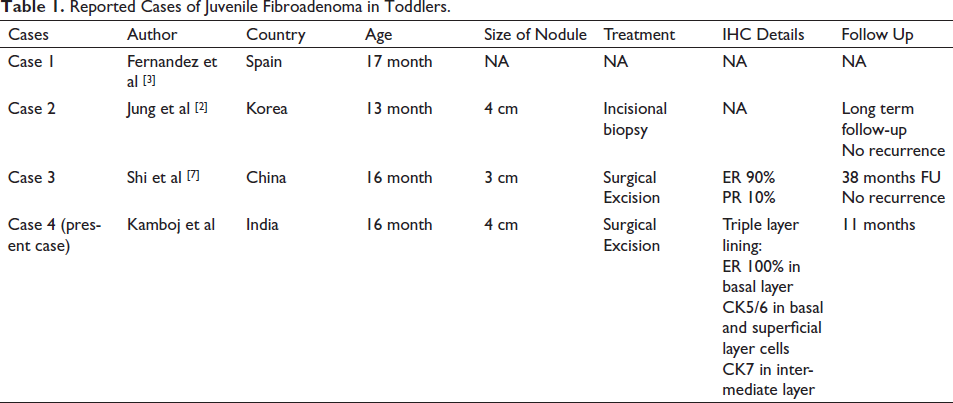
FAs more than 5 cm in maximum dimension and/or weighing more than 500 gm are labelled as giant FA, which are rare and occur only in 0.5% of all cases of FA. 2 Juvenile FA are also usually large in size, which can grow rapidly, may double in size within three to six months, reaching 15 cm to 20 cm causing breast distortion with prominent veins.1, 2 They occur more commonly in adolescents, between 11 and 18 years, the age for onset of puberty. 2 As per the literature, three cases of juvenile FA in toddlers have been reported; ages of girls being 13 months, 16 months and 17 months (Table 1).3–5
Reported Cases of Juvenile Fibroadenoma in Toddlers.
Mammography has a limited role in young patients due to high breast density and also risks of radiation. Ultrasound is superior to mammography in ruling out malignancy with a negative predictive value of 99.5%. 6
Histopathologically, FA shows biphasic epithelial and stromal cell components. Juvenile FAs are more cellular than those seen in adults. 5 These show gynecomastoid type morphology: pericanalicular growth pattern with mild to moderate increase in stromal cellularity, and no significant nuclear atypia. Usual duct hyperplasia is commonly seen.1, 4 Mitotic activity in the stromal component is usually low: <2 mitoses per 10 high-power fields (<1 mitosis/mm2). 1 Juvenile FA with features of phyllodes tumor has been reported in an 11-year-old girl, showing unusual intraductal/intracystic growth. 7
JFA is known to depict a immunoprofile similar to that seen in gynecomastia, with typical three-layered ductal lining (two basal layers and one luminal layer). The inner epithelial cell layer and outer myoepithelial cells express basal cell markers (CK5/6 and CK14), and the intervening middle layer cells express ER, PR, and AR. 1 However, in our case intervening layer expressed CK7, and ER was limited to outer cell layer.
Giant juvenile FA must be distinguished from similar nodular lesions, like phyllodes tumors, virginal hypertrophy, and malignancy. 5 Benign phyllodes tumors exhibit exaggerated leaf-like projections lined by bilayered epithelium, extending into dilated and elongated lumen. The stroma in phyllodes tumors is far more cellular than that seen in FAs. 8 Virginal hypertrophy of breast buds is seen in response to hormonal stimulation, characterized by abundant connective tissue with duct proliferation and lack of lobule formation. 5
Secretory carcinoma is known to occur in children and can mimic FA on radiology, being a lobulated and circumscribed tumor. 9 However, secretory carcinoma is a low-grade (Grade 1 or 2) invasive malignancy presenting as a slow-growing and firm mobile mass, with characteristic intracytoplasmic secretory vacuoles in epithelial cells. 9
Female gynecomastia-like changes have been reported to be 0.15% of all female breast lesions. Cases with juvenile breast hypertrophy have been labeled as gynecomastia-like hyperplasia, mammary hamartoma, or adenolipoma. 10
Treatment of JFA is either excision or observation, and 10% of cases resolve spontaneously. Large-sized FA are often cosmetically distressing to the patient, and reconstructive techniques may be needed for complete excision, preservation of nipple-areola complex, and maintaining symmetrical breasts. 2
Criteria for Inclusion in the Authors’/Contributors’ List
Concept and design of study or acquisition of data or analysis and interpretation of data: Dr Meenakshi Kamboj, Dr Gurudutt Gupta
Drafting the article or revising it critically for important intellectual content: Dr Meenakshi Kamboj, Dr Sunil Pasricha, Dr Anila Sharma, Dr Garima Durga
Final approval of the version to be published: Dr Meenakshi Kamboj, Dr Sunil Pasricha
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Statement
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional or regional) and with the Helsinki Declaration of 1975, as revised in 2000.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Patient Consent
A general informed consent was taken from the patient regarding sharing of clinical data for research purpose. All the patients’ information in the manuscript is anonymized and only de-identified data is used.