
Abstract
Osteochondromas are one of the most common benign neoplasms. Malignant transformation of a solitary osteochondroma to secondary chondrosarcoma is very rare, ranging from 1% to 2%. A new onset of pain, rapid growth of lesion after the closure of the growth plate, and cartilage cap thickness of more than 2 cm in adults and more than 3 cm in children are features suggestive of malignant transformation. Excision of the tumor with free margins is the treatment of choice. We report the case of a 33-year-old man with complaints of pain and progressive swelling over the right axilla. X-ray and MRI features were suggestive of malignant transformation, which was confirmed by histopathology. He underwent a wide excision with tumor-free margins. At 14 months of follow-up, he is asymptomatic with no clinical and radiological signs of recurrence. Malignant transformation of a solitary osteochondroma is extremely rare. High index of clinical and radiological suspicion is mandatory for early diagnosis and prompt management, thereby improving the prognosis and overall survival.
Introduction
Osteochondroma is a benign neoplasm characterized by cartilage-capped bony outgrowth, seen during childhood and adolescence. It is the most common benign tumor and accounts for 20%–50% of all benign tumors. These are of two types, namely, sessile and pedunculated. They can present as a solitary lesion or multiple lesions, as in the case of hereditary multiple exostoses, with the former being the most common presentation. 1
Usually osteochondromas are painless, asymptomatic, and discovered incidentally. Pain in osteochondroma is usually due to bursal inflammation, fracture of the stalk, compression of adjacent neurovascular structures, or malignant transformation. The most dreaded and rare complication is malignant transformation, accounting for less than 1% of reported cases in solitary osteochondroma and approximately 10% in hereditary multiple exostoses 2 characterized by a hyaline cartilage cap thicker than 2 cm. 3 Transformation of osteochondroma usually results in low-grade secondary chondrosarcoma, with an overall good prognosis and 5-year survival rate of about 90% compared to its primary counterpart, 4 and is usually more common after maturity.5–7. Proximal femur, proximal humerus, scapula, and pelvis are the common locations where transformations are reported. 8 Pain, progressive growth of tumor after skeletal maturity, ill-defined tumor margin, internal lucency, permeation into adjacent bone, and cartilage cap thickness greater than 2 cm are signs of possible malignant transformation.3, 9 Here we report a case of malignant transformation of osteochondroma in an adult with most of the clinical and radiological signs of transformation, in whom histopathology confirmed a low-grade secondary chondrosarcoma. Wide excision of the tumor was carried out with tumor-free margins.
Case Report
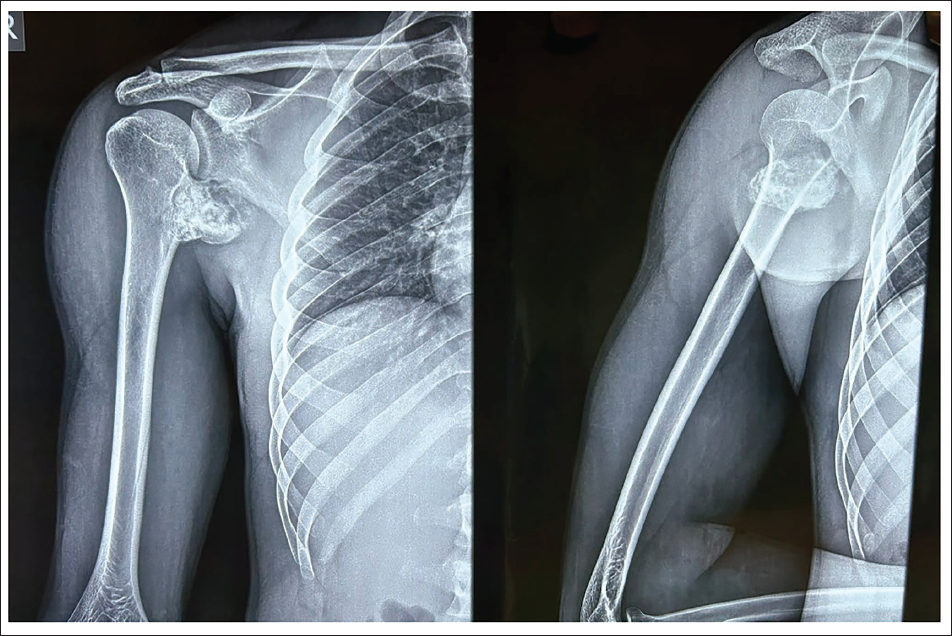
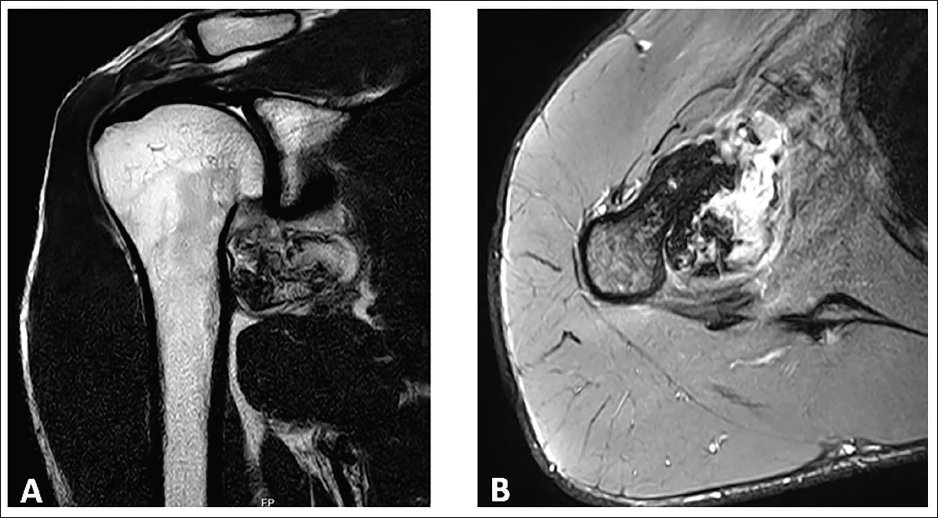
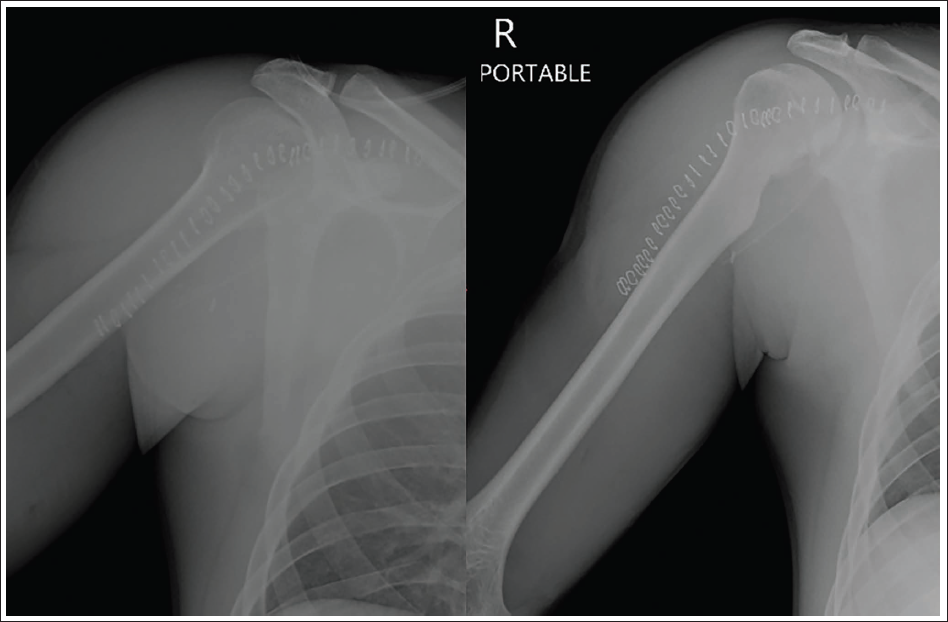
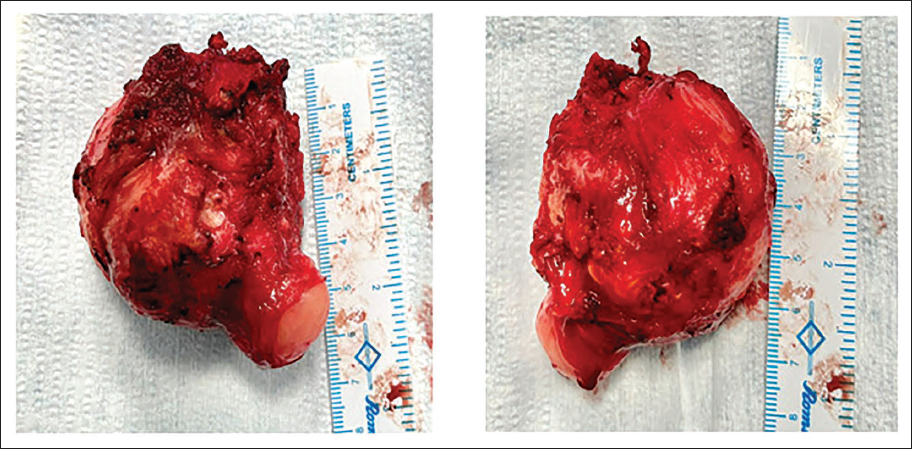
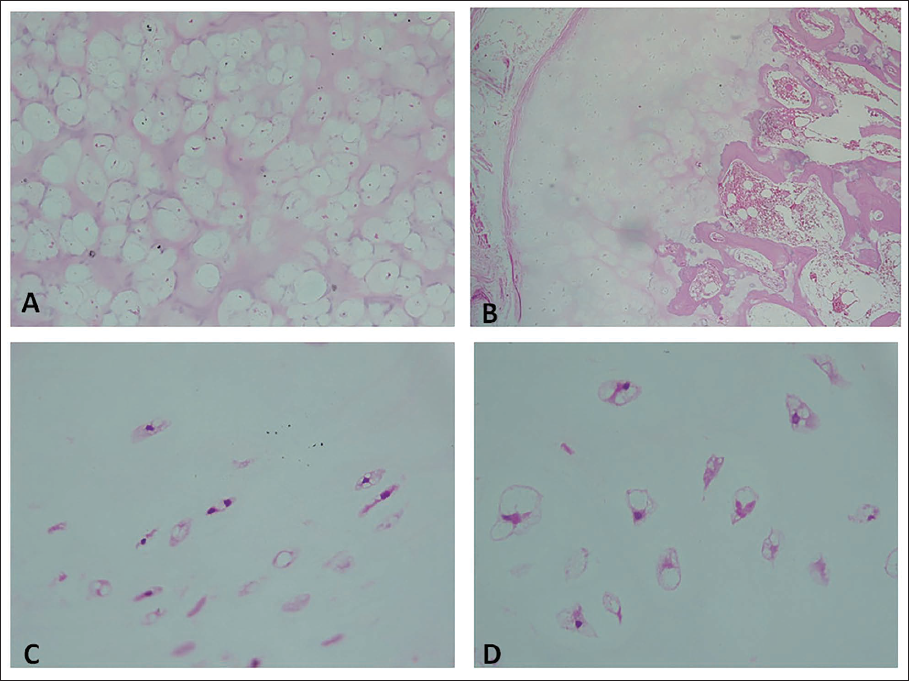
A 33-year-old male presented to our clinic with pain and progressive swelling over the right axilla for 4 months. Physical examination revealed a well-defined, irregularly surfaced, tender, bony-hard mass of size 5 × 5 cm over the medial aspect of right proximal humerus protruding into the axilla. The swelling was continuous with the medial cortex of humerus and moving with shoulder movements. Skin over the swelling was stretched and shiny. Extreme shoulder movements were restricted due to pain and swelling. Plain radiograph (Figure 1) and magnetic resonance imaging of the right humerus (Figure 2) revealed a well-defined, pedunculated, cartilagenous exostotic lesion with lucent areas at the tip, arising from the medial cortex of the metaphysis of proximal humerus with corticomedullary continuity, causing pressure erosion over the inferior aspect of scapular neck. Cartilage cap thickness was found to be 5 cm. Core needle biopsy was taken from the swelling, showing abundant binucleate chondrocytes in a hyaline matrix with atypical cells. Hence, a diagnosis of low-grade secondary chondrosarcoma arising from osteochondroma was considered. Wide resection (Figure 3) of the mass was done along with the previous biopsy tract. Grossly, the swelling was lobulated, measuring 5 × 5 × 4.8 cm (Figure 4A and B). Microscopic examination showed cartilaginous cap with abundant neoplastic cartilaginous cells arranged in lobules separated by myxoid stroma; cells showed mild nuclear atypia with areas of calcification (Figure 5A–D). Margins were reported free of tumor. At the 14-month follow-up, the patient is asymptomatic, with full range of shoulder movements, and no clinical or radiological signs of recurrence.
Plain Radiograph of Right Humerus AP and Lateral Views.
Magnetic Resonance Imaging of Right Humerus. (A) T2W Coronal Image, (B) T2W Axial Image Showing Pedunculated Osteochondroma with Cartilage Cap.
Post-operative Radiograph AP and Lateral Views.
Gross Examination Showing Lobulated Osteochondromatous Mass with White Cartilage Cap.
Microscopic Examination. (A) H&E Stain, 10× Magnification. Lobular Arrangements of Chondrocytes with Increased Cellularity. (B) 40×, Bony Trabecula with Intervening Marrow Elements and Spaces with a Cartilagenous Cap More Than 4 cm. (C) 40×, Binucleate Chondrocytes with Mild Nuclear Atypia.
Discussion
Osteochondromas are usually incidentally detected, as they are mostly asymptomatic. They usually grow in childhood, but seldom after skeletal maturity. 10 The development of symptoms and the growth of the lesion after skeletal maturity should arouse a clinical suspicion of malignant transformation. The malignant changes are seen mostly in the cartilage cap, leading to secondary chondrosarcoma. 11 Malignant transformation is found to occur in 1% of solitary osteochondroma and approximately 10% in HME. Worrisome imaging features suggestive of malignant transformation are ill-defined margins, internal lytic areas, calcification, and erosion of adjacent bone cortex.9, 11 However, the most sensitive feature is the measurement of cartilage cap thickness, evaluated with CT or MRI cross-sectional studies. A cartilage cap thickness of more than 2 cm in adults and 3 cm in children is suggestive of malignant transformation. 11 Most of these secondary chondrosarcomas are low to intermediate grade.2, 11 Tsuda et al., in their study, found that the accuracy of preoperative biopsy in predicting the final histological grade is only 27%. They recommended a multidisciplinary approach including orthopedic oncologists, radiologists, and pathologists for a collective scrutinization of the clinical, imaging, and pathological features collectively in diagnosing a secondary chondrosarcoma arising from preexisting osteochondroma rather than depending solely on histopathological diagnosis. 12
These secondary chondrosarcomas are low-intermediate grade, with less risk of distant metastases, and have favorable prognosis compared to the primary counterpart. Hence, wide resection is the treatment of choice. Marginal resection leads to a high recurrence, usually appearing within 5 years. 9
Conclusion
Malignant transformation of a solitary osteochondroma is extremely rare. The most common malignancy is secondary chondrosarcoma, which is mostly low grade with favorable prognosis. However, diagnosing the transformation is extremely challenging. In the event of suspicious clinical and imaging features, a wide excision and histopathological confirmation are mandatory.
Clinical Message
Since secondary chondrosarcoma arising from osteochondroma is rare and has subtle clinical and radiological features, we recommend a high index of suspicion and a multidisciplinary team approach involving the orthopedic surgeons, radiologists, and pathologists for early diagnosis and prompt management.
Ethical Approval
Not applicable.
Informed Consent
The authors confirm that informed consent was obtained from the patient for publication.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.