
Abstract
Melanoma arising from melanocytes is an uncommon neoplastic lesion, with rare occurrences in anorectal mucosa. While mucosal melanomas constitute a small portion of all melanomas, anorectal cases are even rarer and present with aggressive behavior and poor prognosis. Surgical management is central, with evolving debates regarding optimal approaches. We present a case of a 60-year-old woman with anorectal melanoma. She complained of rectal bleeding and weight loss. Clinical examination and pelvic magnetic resonance imaging revealed a 3-cm budding lesion on the anterior rectal wall. Colonoscopy identified a pedunculated anorectal tumor of 3 cm, situated 4 cm from the anal margin. A biopsy led us to a malignant lesion: anorectal melanoma. Pelvic imaging displayed a localized tumor, prompting wide local excision with millimetric negative margins. These resection margins were estimated insufficient, even in front of R0 resection. Thus, and after multidisciplinary discussion, we opted for abdominoperineal resection after wide local excision. Lymph nodes were biopsied, confirming no residual tumor. Follow-up exhibited no recurrence at 1 year. Our case emphasizes the pivotal role of surgical strategy in managing anorectal melanoma, challenging the paradigm of organ preservation. Despite therapeutic progress, surgery remains integral, contributing to improved outcomes and addressing the metastatic potential inherent to this disease.
Introduction
Melanoma stands as an extraordinary neoplastic lesion originating from melanocytes. While predominantly located within the skin, these cells can also manifest in the nasal and anorectal mucosa. 1 Among melanomas, mucosal melanomas constitute a mere 1.3% with anorectal occurrences being even rarer, comprising a mere one-quarter of cases. 1 This aggressive tumor presents a bleak prognosis, with a mere 15% estimated survival at 5 years. 2 This dire outlook, influenced by early metastasis, is gradually improving due to advancements in targeted therapy and immunotherapy. 3 Nonetheless, surgical intervention remains pivotal in managing early-stage anorectal melanoma (ARM). Although abdominoperineal resection (APR) was the conventional surgical approach, the paradigm is shifting toward wide local excision (WLE), 4 often coupled with adjuvant therapy. Amidst this ongoing debate, we present a case of a 60-year-old woman with ARM to illustrate this dilemma.
Case report
A 60-year-old woman, with a history of hypothyroidism under treatment, experienced 3 months of rectal bleeding and weight loss. Physical examination revealed a non-painful abdomen, while digital rectal examination unveiled a 3-cm budding lesion with a thin pedicle on the anterior aspect of the rectum, located 3 cm from the anal verge. Colonoscopy identified a pedunculated anorectal tumor of 3 cm, situated 4 cm from the anal margin. A biopsy led us to a malignant lesion: ARM. It showed an invasion of the anorectal mucosa by pigmented polypoid proliferation arranged in sheets and thecae (Figure 1) Pelvic magnetic resonance imaging (MRI) demonstrated a 2-cm budding tumor in the anal canal with hyperintensity on T2 acquisition and no local extension, particularly to the mesorectum and sphincter complex (Figure 2). Computed tomography and positron emission tomography (PET) scans revealed no distant metastasis. A nonmetastatic ARM without sphincter complex invasion was diagnosed, leading to the decision to perform WLE. Intraoperatively, a 3-cm tumor with an 8-mm implantation base was found at the dentate line (Figure 3). A WLE was executed, maintaining a 5-mm healthy tissue margin from the internal sphincter (Figure 4). Pathological analysis exhibited a 15-mm polypoid ulcerated lesion with characteristics suggestive of melanoma. Molecular tests confirmed melanoma, revealing positivity for proteins S100 and Melan A. Resection with negative 1-mm margins (R0 resection) was confirmed, along with seven mitoses per mm², devoid of vascular or perineural neoplastic invasion. A multidisciplinary discussion ensued, culminating in the choice of APR due to safety margin concerns. Indeed, the resection margins of 1 mm were estimated insufficient, even in front of R0 resection. The dilemma in front of such a rare tumor with a pejorative prognosis was to guarantee a recurrence-free and longer survival for our patient with her consent. Hence, APR was performed after the WLE. Right and left iliac sentinel lymph nodes were biopsied, all showing absence of residual tumor. Subsequent follow-up exhibited no recurrence at 1 year, supported by pelvic MRI and PET scans.

(a) Low magnification (×40) anorectal mucosa invaded by pigmented polypoid proliferation arranged in sheets and thecae. (b) Cells loaded with melanin pigment with, at high magnification, central mitosis and clear cytonuclear atypia (×400).

Magnetic resonance imaging showing a 2-cm budding tumor of the anal canal with no local extension.
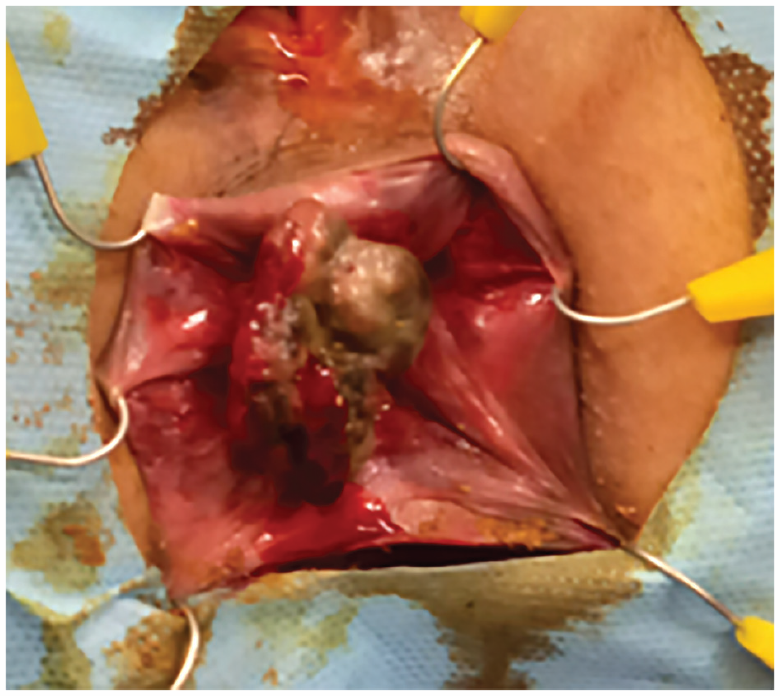
Intraoperative findings of the tumor located on the dentate line with an implantation base of 8 mm.

Wide local excision of the tumor.
Discussion
Malignant melanoma of the rectum typically presents in the fifth or sixth decade of life with nonspecific complaints such as rectal bleeding or anal pain. 5 In front of clinical nonspecific features, imaging plays a crucial role in the management of ARM, thereby, fixing local and distant extension workup. MRI is used to evaluate local involvement as it shows habitually a bulky intraluminal polypoid mass in the anorectum with the mass showing T1 hyperintensity, high or mixed signal T2 intensity, hyperenhancement, minimal perirectal or anal infiltration, and lymphadenopathy. 6 Thus, findings such as perirectal infiltration or invasion of the sphincter complex considerably affect the choice of the operating technique. The surgical procedure saw the emergence of a new approach in the last decade. APR which was considered the standard intervention is nowadays discussed. It can control the lymphatic spread and ensure safe resection margins. However, it is a mutilating intervention with psychological side effects as it affects body image. Local wide excision is nowadays more attempted showing good results. It has clear advantages, including faster recovery and little impact on bowel function without the need for a permanent stoma. 6 Several studies have investigated the difference between these different surgical approaches.1,7–10 In fact, in different studies the survival rate is higher in patients who had a WLE compared to APR, especially in early-stage disease (stage I and II). As it was shown in the study of Sven Goldman et al., 11 There was a clear correlation between tumor size and survival. In fact, APR is more associated with bigger tumors. The recurrence rate is substantially greater in the WLE group as the R0 resection is less obtained. However, survival is in favor of local excision, and the only factor that could determine the long-term prognosis is the N+ patients regardless of the surgical approach, and that was the reason for which we initially opted for WLE, despite a size of the tumor >2 cm. Smith et al., 12 besides the similarity in terms of overall survival (OS), do not conclude a significant difference in terms of disease-free survival and especially in local recurrence-free survival. This leads us to ask about the interest of such major interventions as the APR while organ preservation by a local excision associated eventually with adjuvant treatment shows satisfying results. Indeed, radiation, chemotherapy, or recently immunotherapy have been introduced as adjuvant treatment to surgery. In a recent retrospective cohort analysis published in 2019, 13 immunotherapy has shown a significantly better 2-year OS than other therapies. It also showed its efficiency through a randomized clinical trial. 14 Adjuvant ipilimumab significantly improved recurrence-free survival for patients with completely resected high-risk stage III melanoma. Our report has value as it emphasizes the WLE as a cornerstone of the management of ARM. Our patient had a WLE followed by an APR and the specimen did not show any residual tumor in the pathological examination. This lets us think about the best surgical treatment for ARM considering that the site of recurrence was, for more than 30%, 15 distant. Therefore, considering that the prognosis of ARM is on its metastatic potential, the principle of organ preservation is now being considered more and more.
Conclusion
Our case underscores surgical strategy’s significance in treating ARM. Despite therapeutic advancements, the role of surgery is pivotal, challenging the notion of organ preservation in a context where metastasis primarily dictates prognosis.
Footnotes
Acknowledgements
None.
Author contributions
T.M.M.: Conceptualization; writing—original draft. K.N.: Supervision. I.M.: Writing—original draft. C.M.A.: Validation; writing—review and editing. B.R.H.: Validation; writing—review and editing. K.W.: Validation; writing—review and editing. J.H.: Validation; writing—review and editing.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.