
Abstract
Purpose
To explore the role of radiotherapy (RT) in management of moderate to severe thyroid-related eye disease in terms of efficacy, treatment outcome, and response.
Material and methods
A case series of 5 patients with moderate to severe Graves Ophthalmopathy treated with orbital RT between July 2020 and March 2021. Patient symptoms and ophthalmic findings prior to RT and after 6 months post RT were analyzed. Computed tomography was performed before and after RT to compare orbital (muscles) volume change. Endpoints including improvement in ocular symptoms such as diplopia, proptosis, extraocular movement were compared. Acute and long-term complications were documented to assess its safety and treatment response.
Results
Addition of RT improved diplopia, visual acuity, proptosis, and color vision significantly. RT also decreased upper lid edema, optic nerve compression, and reduced intraocular muscle bulk. Extraocular muscles diameter reduced significantly. Patients experienced relief of symptoms and significant reduction in diplopia clinically.
Conclusion
External beam radiation is a safe and effective intervention in thyroid ophthalmopathy. Our study demonstrated that radiation is effective in decreasing inflammatory signs, symptoms, and muscle bulk. This treatment modality is well tolerated, and long-term complications are tolerable.
Keywords
Abbreviations
Ag-Ab: Antigen antibody
IMRT: Intensity modulated radiotherapy
OAR: Organ at risk
OR: Orbital radiotherapy
TAO: Thyroid associated orbitopathy
TED: Thyroid eye disease
TRO: Thyroid related orbitopathy
TSH-R: Thyroid stimulating hormone-receptor
Introduction
Graves’ orbitopathy (GO) is an autoimmune disorder of the orbit associated with many ocular symptoms. It is the most prevailing extra thyroidal manifestation of Graves’ disease. Almost 90% cases are associated with hyperthyroidism. Other causes of thyroid-related ophthalmopathy are Hashimoto’s thyroiditis and thyroid carcinoma. 1 Females are more frequently affected than males and the disease is more severe in elderly patients. Smokers are more labile for severe course of disease. Smoking cessation reduces risk of disease progression. 2 GO causes inflammatory changes in orbital tissues which include potential thickening and fibrosis of the extraocular muscles (EOM) and orbital fat. This results in increased volume of bony orbit leading to ocular symptoms such as orbital pain, proptosis, diplopia, optic nerve compression, exposure keratitis, corneal ulceration, and visual damage. 3 The development of GO is characterized by progressive deterioration of active symptoms, followed by a plateau. 4 In acute phase of disease, progressive deterioration appears as an autoimmune response which is characterized by lymphocyte infiltration, cytokine secretion, and fibroblast proliferation. The primary aim of GO treatment includes preserving vision, reducing diplopia, relieving ocular pain, and improving cosmetic appearance. Backbone of treatment in active inflammatory phase is systemic glucocorticoids and orbital radiotherapy (RT). 5 High-dose intravenous (IV) glucocorticoids are the first-line treatment for moderate-to-severe active GO patients, with success rates from 54.3% to 77%.6, 7, 8 The main drawback is frequent relapse when they are withdrawn or tapered. Apart from that multiple side effects including immune suppression, hyperglycemia and hypertension could restrict the usage of corticoids administration. Retro-orbital RT is useful in treating GO patients who are not responding, recurrent disease, and patients intolerable to corticoids therapy. The mechanism is mainly through the nonspecific anti-inflammatory effects of RT, suppressing radiosensitive infiltrating lymphocytes, inhibiting fibroblast proliferation and muco-polysaccharide secretion. 9 RT is moderate to reveal therapeutic effects than corticoids but it provides a more prolonged protection period. 10 The available data suggest particularly effective in EOM involvement, especially when it is of recent onset. 11 Recent-onset active GO is much more sensitive to treatment than longstanding or inactive disease. Inflammatory signs, recent-onset eye muscle dysfunction, and optic neuropathy respond very well to orbital RT, while proptosis and longstanding eye muscle restriction respond relatively. 12 So far, studies have reported a wide range of responses to radiation therapy for GO.13-15 20 Gy in 10 fractions was most widely used in the literature reviewed, although other fractionation schemes (1 Gy per week for 10 or 20 weeks) have shown clinically significant therapeutic responses.16, 17
We report this case series of 5 patients with moderate to severe graves ophthalmopathy with progressive disease after initial treatment. Patients received 20 Gy in 10 fractions (2 Gy per fraction) over 2 weeks with IMRT technique.
Case History
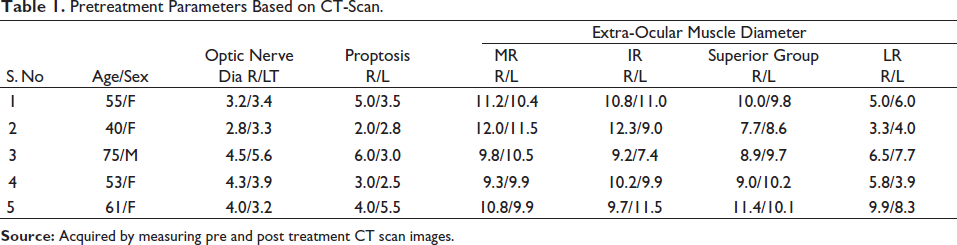
We have treated 5 patients with moderate to severe thyroid eye disease between the ages of 40 and 75 years with a known history of hyperthyroidism during July 2020 and March 2021 in our center. Four female patients and one male patient were evaluated for acute onset gritty red sore eyes. Symptoms including restriction of movements, demised vision, proptosis, and feeling of generalized weakness were noticed in patients. Patients were diagnosed as thyroid-related eye disease after complete laboratory and radiological workup. All these patients were under treatment regular with endocrinologist and ophthalmologist for control of thyroid hormone levels and eye symptoms, respectively. Patients underwent orbital decompression surgery to relieve compressive symptoms and course of oral/IV steroid was given along with oral carbimazole/methimazole. After complete evaluation and pretreatment, workup patients were planned for treatment with External beam RT. Dose of 20 Gy in 10 fractions over 2 weeks was delivered using the IMRT-VMAT technique. After 6 months of treatment, a follow up CT scan was done and compared with pretreatment CT scan to assess the treatment response. The findings are documented in Tables 1 and 2.
Pretreatment Parameters Based on CT-Scan.
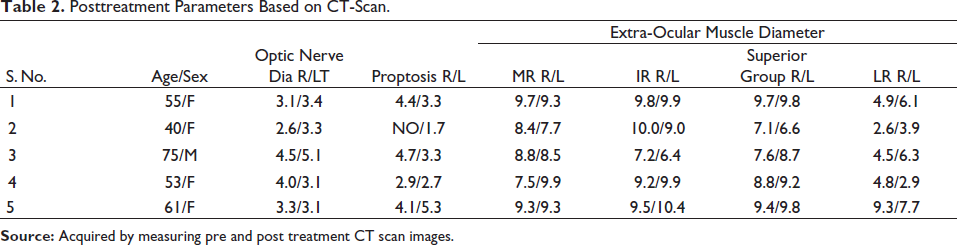
Posttreatment Parameters Based on CT-Scan.
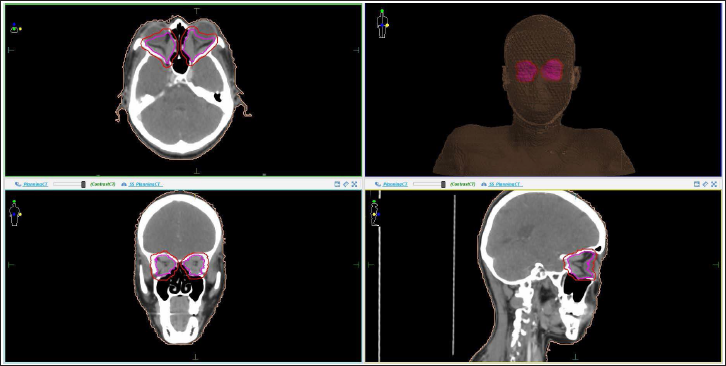
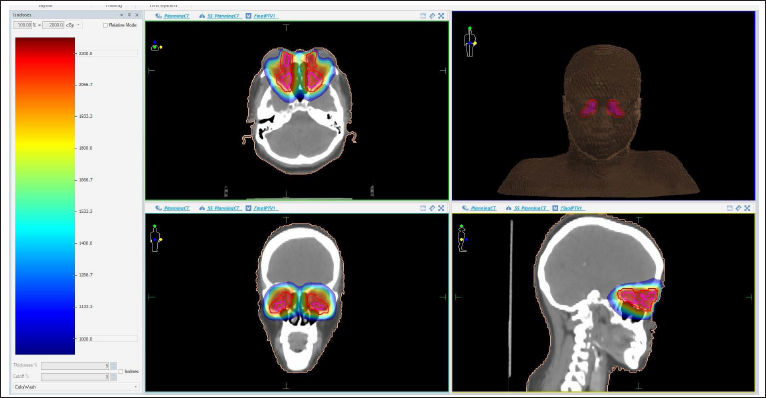
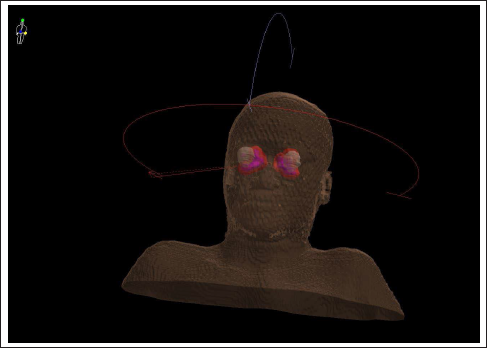
Methods
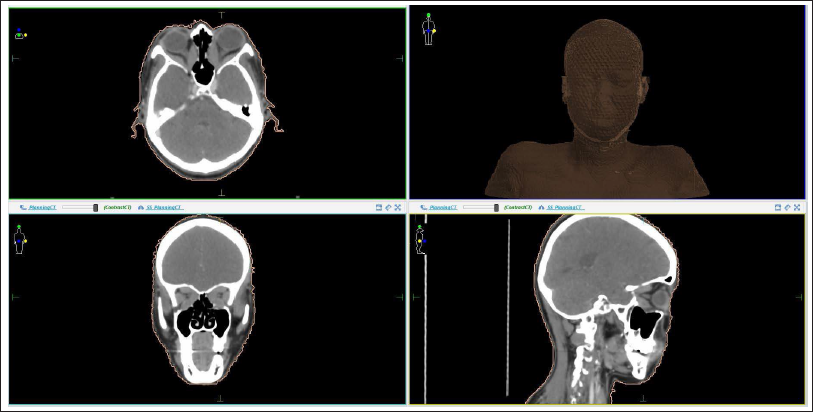
After explaining the pros and cons of the radiation treatment, written and informed consent was taken. Patients were simulated in supine position (Figure 2a) and a Perspex® shell immobilized the head and neck. The target volumes were contoured meticulously (Figure 2b). Plans were generated on Monaco (Version 5.51.10) TPS (Figure 2d) and treatment was executed on Elekta Versa HD. Patients received 20 Gy in 10 fractions (2 Gy per fraction) (Figure 2e) over 2 weeks with IMRT technique with 6 MV photon beams (Figure 2c). Treatment was completed in 2 weeks and tolerated well by the patients. Two patients were observed having mild inflammation and redness in eyes after receiving 3 to 5 fractions which was resolved in 2-3 days after using artificial tear drops at regular intervals. Follow-up scan was done and findings were documented (Tables 1 and 2).
Discussion
A recent review on the efficacy and safety of orbital RT for GO concluded that the combination of orbital RT and oral glucocorticoids is superior to either alone. Treatment with orbital RT, are most effective during the active phase of disease. Consistent with our study findings, this review concluded that RT significantly reduced the need for further treatment, including further steroid or immunosuppressive therapy. 11 A recent meta-analysis of prospective studies did not show a difference between RT and sham RT, based on changes in the clinical activity score (CAS, a validated scoring system based on signs of inflammation such as pain, redness, swelling, and impaired function), but did show that RT yielded a higher response rate for diplopia with an odds ratio of 4.88. 11 This meta-analysis concluded that orbital RT as a sole treatment modality for GO remains controversial, but RT in combination with corticosteroids has greater efficacy than either treatment alone.11, 16
Prospective studies comparing RT with sham irradiation and comparing RT with corticosteroids for GO reporting variable responses to RT have generally included patients at all phases of disease and have largely aimed at measuring response to ocular symptoms.15, 18, 14 A recent Cochrane Review of orbital RT for GO, which included only 2 studies in their meta-analysis due to the large heterogeneity of outcome measures in prior trials, concluded that RT was superior to sham RT. 19 The individual studies included in this review suggested that RT in combination with corticosteroids was more effective than corticosteroids alone. Orbital RT is generally well tolerated with few adverse effects, as noted in our retrospective review. With approximately 11 years of follow-up after orbital RT for GO, prior studies found no associated increase in secondary malignancy or difference in overall survival. 20 Almost all studies agree on the tolerability and safety of RT, showing no increase in secondary malignancies and difference in survival. The risk of cataracts from low-dose RT for GO also appears low approx 12%, based on prior retrospective studies that have reported similar prevalence of cataracts in patients treated with corticosteroids for GO, patients treated with low-dose RT for GO (20 Gy in 10 fractions), and the general population. 21
In attempts to minimize radiation-related toxicities and potentially improve treatment efficacy, alternative dose and fractionation schedules have been evaluated, including 20 Gy in 20 fractions, 10 Gy in 10 fractions, 16 Gy in 8 fractions, and 2.4 Gy in 8 fractions. 20 Gy in 10 fractions was most widely used radiation dose in the literature reviewed Prospective studies comparing these dose and fractionation schedules have shown similar responses, but these studies are small and the endpoints for therapeutic responses were again variable.22, 23 Nonetheless, low-dose radiation has been suggested to have a greater inhibitory effect on the inflammatory response and the nitric oxide pathway, and given the greater risk of retinopathy with higher radiation doses, these studies provoke further investigation of lower dose RT for GO.
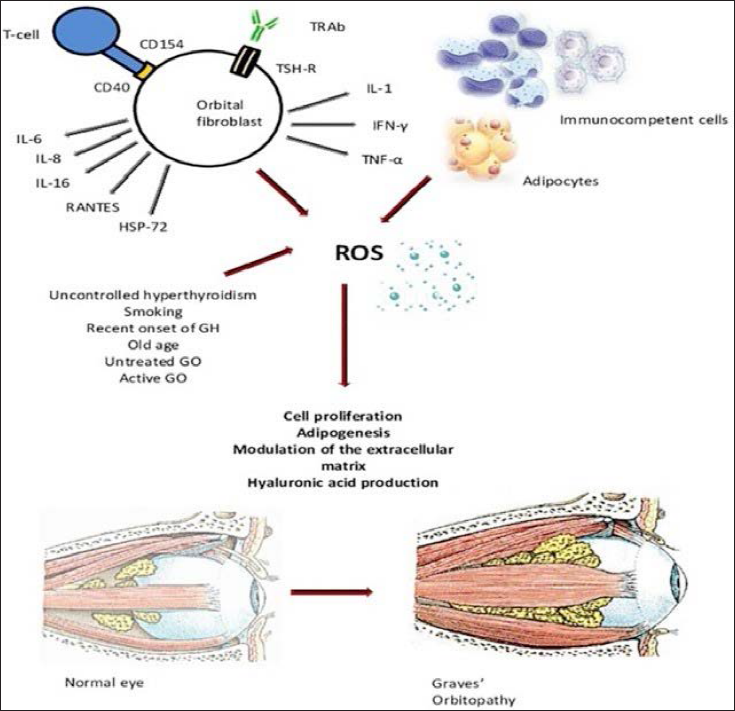
Our study evaluated the efficacy of addition of RT in terms of reduction in symptoms such as diplopia, muscle bulk, and proptosis. Graves’ ophthalmopathy is an autoimmune disease (Figure 1) with the following 3 main phases in pathology: active phase, plateau or static phase, and inactivation phase. The active phase is characterized by periorbital and orbital inflammation, leading to volume increase of extra-orbital muscles and orbital adipose tissue. This pathophysiology accounts for the clinical presentation of proptosis, diplopia, extraocular movement restriction, and compressive optic neuropathy with a risk of decreased visual acuity. It is during this active phase that medical treatment, corticosteroids, and RT are thought to be most effective, highlighting the importance of early intervention, possibly within the first year of onset of symptoms. Remission during the inactivation phase can occur spontaneously but the patient can often be left with residual cosmetic or functional changes. Therefore, patients in the inactivation phase will often require surgery to have improvements in their orbital and visual symptoms and quality of life. 9 RT with corticosteroids has been shown to be effective and admissible, improving patient’s visual acuity, color vision, and upper lid edema. Patients benefited from active monitoring that led to quick intervention during its active phase. This increases the importance of early consideration of RT in patients with GO who are not responding to corticosteroids and consideration of outcome measures other than improvements in orbital and visual symptoms to evaluate the response of RT.
Planning CT Scan.
Target Volumes.
Distribution of Dose in Color Wash.
Beam Arrangement.
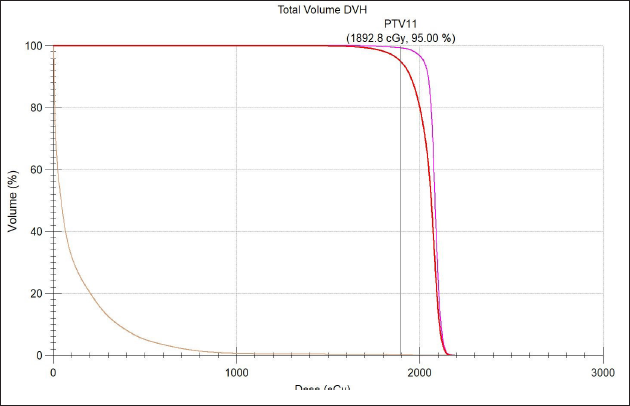
Dose Volume Histogram.
Results
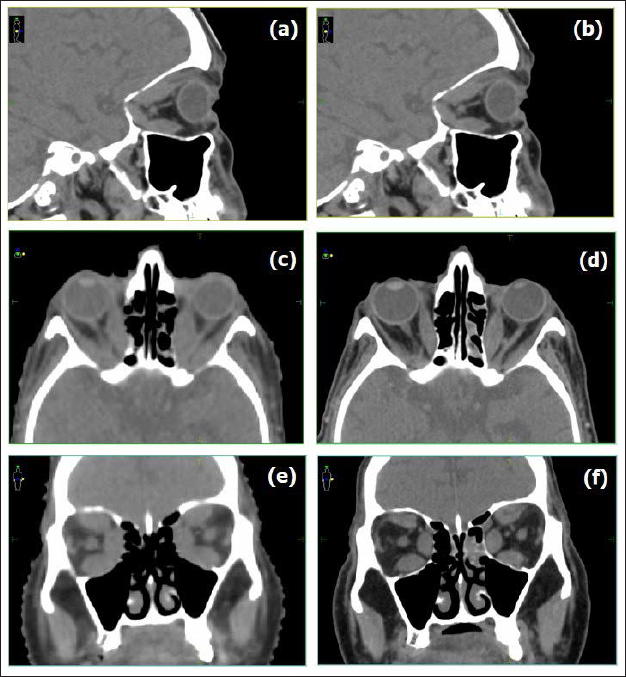
Addition of RT improved diplopia, visual acuity, proptosis, and color vision significantly. RT also decreased upper lid edema, optic nerve compression, and intraocular muscle bulk (Figure 3). EOM diameter reduced significantly. Patients experienced significant reduction in diplopia clinically. Good average reduction (0.38 mm) in optic nerve compression was documented. In EOM, significant reduction of 1.88 mm and 1.5 mm was observed for right and left medial rectus, respectively. For right and left inferior rectus, the average reduction was 1.5 mm and 0.64 mm. Average reduction in right and left superior group of muscles was observed to be 0.88 mm and 1.14 mm. Right and left lateral rectus reduction was observed to be 0.88 mm and 0.58 mm, respectively. Average reduction of 4 mm in proptosis was also observed. Patients reported significant reduction in diplopia clinically.
Pre and Post OP Scans of Patient Compared at Various Levels.
Conclusion
External beam radiation is a safe and effective intervention in thyroid ophthalmopathy. Appropriate selection of patients is essential. Orbital inflammatory signs and symptoms are eliminated within weeks by adding RT as a treatment option. Our study demonstrated that radiation is effective in decreasing inflammatory signs and symptoms due to inflammation. This treatment modality is well tolerated and long-term complications are almost non existing.
Pearls
TED is rarely seen in the RT setting. We see the unique aspects of this disease and the multidisciplinary approach needed in this study.
This case series provides an overview of how this treatment was planned and delivered, and highlights new techniques that could be implemented.
TED requires timely intervention owing to the unpredictable nature of disease progression.
Further studies on the use of RT in a controlled environment are needed to understand the true efficacy and mechanisms of the said intervention.
Footnotes
Acknowledgments
We would like to thank our Physics team, RTT team, and the ethics committee for helping us to do this study. We would like to thank all the patients who are part of this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval and Informed Consent
All the patient data were obtained as a part of the prospective data registration program and there was no intervention. Therefore, this study was exempted from the ethical approval requirement by the hospital ethics committee. Nowhere in this study patient personal details has been revealed.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.