
Abstract
Introduction
Caring for young stroke survivors presents challenges for carers. Little is known about the burden experienced by them.
Aim
In this study, we estimated the caregiving burden among carers of young stroke survivors and explored its patterns and determinants.
Methods
One hundred and fifty young stroke survivors (aged <45 years at index stroke) and their caregivers were recruited in this hospital-based cross-sectional study, three or more months from the stroke. We estimated the burden of caregiving using Burden Assessment Schedule-20 (BAS). Cognitive status, physical disability, and neuropsychiatric symptoms were evaluated using standard instruments. We used descriptive statistics and performed multivariate analysis for factors associated with high burden. We used STATA ver. 14.2, Stata Corp, TX, USA.
Results
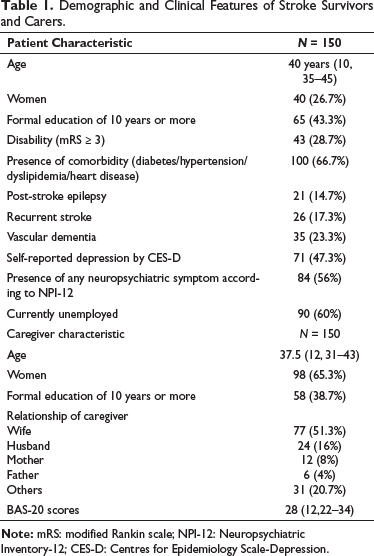
The median age of caregivers was 37.5 years (IQR 12) and 98 (65.3%) were women. The carers were most often spouses (101; 67.3%). The median total BAS score was 28 (IQR 12). Most carers (127; 84.7%) experienced some burden while 15 (10%; 95%CI: 5.2%–14.8%) reported high burden. The most common domain of burden was relationships with others (105; 70%) and marital relationships (66; 65%). Dementia (OR: 2.55; 95%CI: 1.07–6.07) and the presence of neuropsychiatric symptoms (OR: 7.62 95%CI: 2.94–19.81) were associated with an increased burden of caregiving.
Conclusion
Most caregivers of young stroke survivors experience some burden, with interpersonal relationships being the most common domain. Dementia and neuropsychiatric symptoms are associated with increased burden.
Abbreviations
BAS: Burden Assessment Schedule-20
CDR: clinical dementia rating
NPI-12: Neuropsychiatric Inventory-12
Introduction
In India, as in other countries, stroke survivors primarily rely on home-based care with family members acting as primary caregivers. 1 The key role played by caregivers in the rehabilitation of stroke survivors and providing continued stroke care has resulted in rehabilitation approaches moving toward a more patient and caregiver-centric model.2, 3 However, such informal caregiving over long periods of time can be associated with significant consequences for the caregiver. 4 The carer often has to constrain social participation and/or withdraw from the workforce. Further, the constant demands of caregiving can have detrimental effects on the mental health of the carer. 5
In a systematic review of studies reporting caregiver burden following stroke, 6 it was noted that the prevalence of high caregiver burden was 24%–54%. The authors concluded that more research was needed to understand this burden and use this knowledge to develop interventions to offset it.
Young adults between 18 and 50 years of age often are breadwinners, parents of young children, and carers of elderly family members. Thus, young stroke survivors and their families, have to contend not only with the stroke-associated disability and increasing healthcare expenditure but also loss of productivity. 7 Further, unlike in other age groups, there is evidence to suggest that globally there is an increase in the incidence of stroke in young adults. 8 There is little known about the caregiving burden experienced by carers of young stroke survivors. In this study, we aimed to estimate the proportion of principal caregivers of young stroke survivors experiencing a high burden of caregiving and to identify its determinants.
Methods
Study Design and Setting
Between Jan 2018 and July 2019, we recruited 150 consecutive young stroke survivors (between 18 and 45 years of age at index stroke) and their principal caregivers from the outpatient stroke clinic of a tertiary care referral hospital in south India for this cross-sectional study. After obtaining institutional ethics committee approval (JIP/IEC/2017/0450) approval we approached the participants at least three months after the last stroke. The principal caregiver was defined as the person who is involved in routine care of the patient and spends 10 hours/day or more with them. We excluded stroke survivors with severe aphasia, only silent infarctions, major pre-existing psychiatric illnesses, and other acute conditions producing neurologic dysfunctions. Stroke survivors whose caregivers were not available or were unwilling to participate were also excluded. Both stroke survivors and their caregivers participated after providing written informed consent.
Instruments Used
We collected demographic data of survivors and caregivers along with clinical details of patients on a structured proforma using information from hospital records and through direct interviews. Self-reported employment status both current and prior to the stroke, of the stroke survivor was recorded. Jobs requiring technical skills such as electricians, plumbers, etc. were grouped into skilled labor, and those jobs not requiring special skills as unskilled.
We used a modified Rankin scale to assess motor disability. We evaluated cognition using the Addenbrookes Cognitive Examination III Tamil version and clinical dementia rating scale (CDR) sum of boxes scores. We classified cognitive status as dementia, normal cognition, and cognitive impairment, not dementia according to the American Heart Association—American Stroke Association 2013 criteria. 9 Neuropsychiatric symptoms were assessed using the Neuropsychiatric Inventory-12 (NPI-12) and Centres for Epidemiology Scale-Depression. The details of their neuropsychiatric symptomatology have been previously reported. 10
Although many instruments are available to measure caregiver burden in stroke, 11 we assessed using the Burden Assessment Schedule (BAS-20). 12 This scale was developed and validated in the Indian population to assess the caregiving burden in chronic mental health disorders. It has been previously used to estimate the burden among carers of stroke.13–15 It is a semi-quantitative-interview-based scale of 20 items grouped into five factors—impact on well-being; marital relationships; appreciation for caring; impact on relations with others; and perceived severity of the disease. Each question is graded on a 3-point Likert scale with scores ranging from 20 to 60 and higher scores indicating more burden.
All instruments except for NPI-12 are in the public domain and we obtained permission for the use of NPI-12.
Statistical Methods
Descriptive statistics were used to describe the frequency and patterns of the subjective burden of caregiving. A median BAS score with an interquartile range was reported. The correlation was explored between BAS scores and the age of the patient, CDR sum of boxes scores, time from stroke, years of education, and NPI scores. Missing data was reported as such. Based on a literature review, we identified certain patient factors (disability, gender, co-morbidities, employment status, cognitive dysfunction, depression) and carer factors (gender, younger age, and relation to the patient) that were reported to be associated with a higher burden of caregiving.16, 17 We explored these associations, by comparing the group with the highest tertile BAS scores to the lower two tertiles. We performed a univariate analysis for each of these factors. We constructed a multivariate logistic regression model for the factors that were found significant in univariate analysis. We obtained adjusted odds ratios and examined for interactions. The value of p < .05 was considered significant. All analysis was carried out with STATA ver. 14.2, StataCorp, TX, USA.
Results
The median time from stroke to the assessment of the young stroke survivor and caregivers dyads was 24 months (IQR 24). Table 1 details the basic demographic and clinical characteristics of the 150 patients and carers. Of 132 stroke survivors who had details of employment prior to stroke 5 (3.8%) were unemployed and 74 (56.1%) were in employed in skilled labor. Following a stroke, most 90 (68.2%) survivors were unemployed. Carers were younger, less educated, and more likely to be women compared to stroke survivors.
Demographic and Clinical Features of Stroke Survivors and Carers.
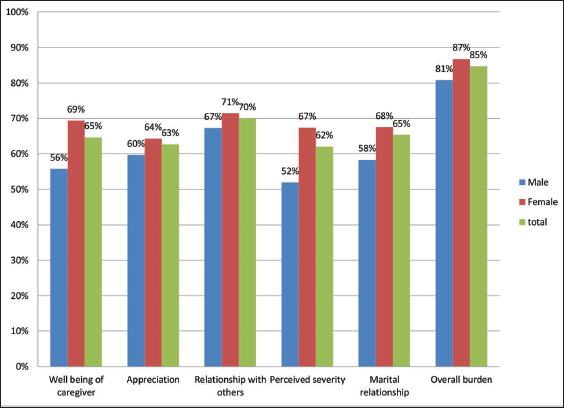
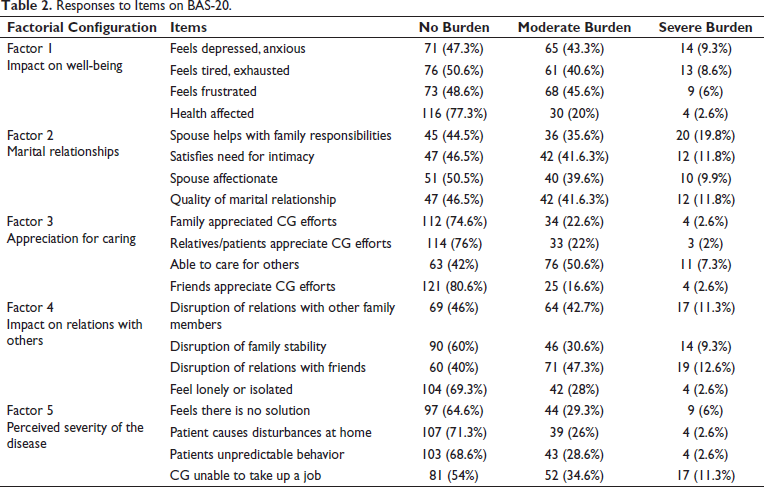
Some burden of caregiving was experienced by 127 (84.7%) of the carers. Of the five domains evaluated in BAS-20, “Impact on relation with others” and “Marital relationship” were most affected (Figure 1). The caregiver responses to individual questions are in Table 2. Correlation analysis revealed that BAS scores increased with increase in the score on NPI-12 (p = .34; p < .001), CDR sum of boxes score (p = .45, p < .001) and with increasing age of stroke survivor (p = .16; p = .04); and decreased with increase education of stroke survivor (p = −.19; p = .02); but BAS score was not correlated with time since stroke.
Proportion Reporting Some Burden on Burden Assessment Schedule-20 by Gender of Caregiver.
Responses to Items on BAS-20.
Fifteen (10%; 95%CI: 5.2%–14.8%) carers reported a very high burden of caregiving (BAS scores ≥40). Twelve of these carers were wives of the stroke survivors. Fourteen of these survivors had neuropsychiatric symptoms, 10 were unemployed and 6 each had dementia and significant disability.
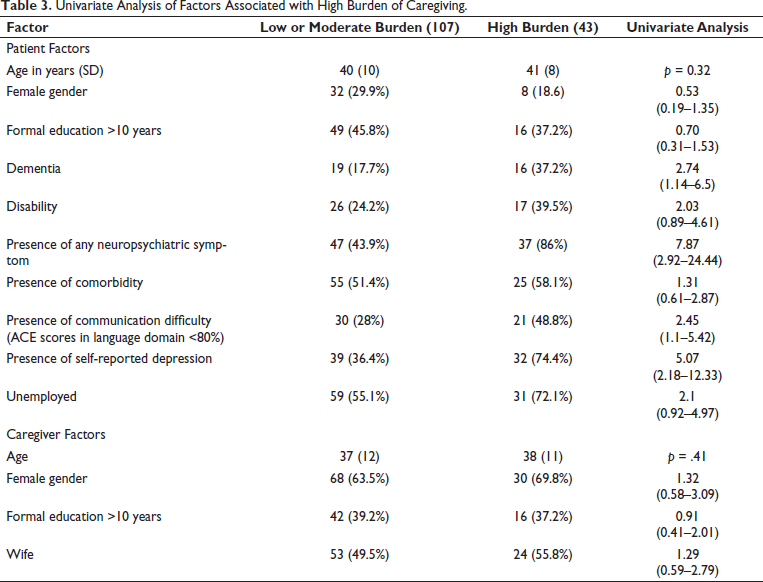
We compared the highest tertile of BAS scores to the lower two tertiles for both patient and carer factors associated with a higher burden of caregiving and the results are in Table 3. On logistic regression analysis, dementia (adjusted OR:2.55; 95%CI: 1.07–6.07) and the presence of any neuropsychiatric symptom (adjusted OR:7.62 95%CI: 2.94–19.81) were the only significant factors that were associated with a higher burden of caregiving, and no interaction was noted.
Univariate Analysis of Factors Associated with High Burden of Caregiving.
Discussion
In this study, we found that around 1 in 10 (95%CI: 5.2%–14.8%) of our caregivers experienced a severe burden of caregiving. The most common domains were burden was perceived were relationships with others and marital relationships. Dementia (OR: 2.55; 95%CI: 1.07–6.07) and the occurrence of any neuropsychiatric symptom (OR:7.62 95%CI: 2.94–19.81) were significantly associated with higher levels of burden.
Telang et al. reviewed studies reporting on the caregiving burden among carers of stroke survivors from India. 18 They identified seven relevant studies and reported that caregiver burden was high in all of them with the highest being reported from Ludhiana with 85% reporting stress on the caregiver strain index. 19 We also found 84.7% of our carers experiencing some burden, however high burden (BAS scores ≥40) was reported in 15 (10%). Bhattacharjee et al. reported a prevalence of major stress using the caregiver stress index, in 34.2% (38 of 111) of stroke carers from India, 16 and similar figures were reported by Khanapur et al. 20 and more recently by Kumar et al. 21 We found a smaller proportion experiencing high burden. This is likely due to multiple reasons including the younger age of the stroke survivors and caregivers, instruments used, cut-offs used, and other patient characteristics like status post decompression. Rigby et al. in their systematic review of 24 studies using nine different assessment scales for post-stroke caregiver burden. 6 They reported that the prevalence of high burden was variable (25%–54%). They too attributed this variation in prevalence of burden to the differences in demographic characteristics and instrument features.
Two studies from India have estimated caregiver burden using BAS or a modified form of it. Das et al. studied caregivers of 199 stroke survivors. They reported that 88% felt that they did not have time to look after themselves and 76% reported feeling depressed or anxious. 13 In our study, 22.6% felt their health was affected and 52.6% felt depression or anxiety. These differences are probably because our stroke survivors were two decades, and our caregivers five years younger than those reported by Das et al. Further, most caregiving in our study was done by spouses while in Das et al. only 30% of caregivers were spouses (wives). Sreedharan et al. studied 150 stroke survivors and their caregivers. 14 Although the caregivers in their study were older, most were spouses like in our study. They found that 40% of caregivers felt their health was affected and 22.6% reported feeling anxiety or depression. They also reported a decline in social function participation of the caregivers using 6 parameters such as visits to marriage, religious places, etc. Though we did not asses similarly, our caregivers reported maximum burden in maintaining relationships with friends (60%) and other family members (54%).
As most of our caregivers (101, 67.3%) were spouses, we were able to assess the effect of caregiving and stroke on their marital relationship using the BAS-20. Sixty-six (65.3%) felt some burden in this domain. More than half felt that their spouses were no longer able to satisfy their intimacy needs and reported deterioration in the quality of their relationship, while less than half felt that their spouses were helping with family responsibilities. Marital relationships of young stroke survivors face considerable strain. Ramazanu et al. identified 17 studies in their scoping review on the experiences of stroke survivors and their spousal carers in the community. They found five key themes including changing the quality of marital relationship. 22 Teasell et al. reported on social issues in young stroke rehabilitation. Of the 55 couples, 8 (14.5%) of young stroke survivors and their spouses separated within three months of the stroke. 23 Thus, marital relationships of young stroke survivors and their spousal caregivers are particular areas of need that need to be addressed as couples are often not adequately prepared to manage stroke at home. 20
Zhu et al. performed a meta-analysis to identify the predictors of caregiving burden among carers of patients with stroke. 24 They identified 22 articles with 3,025 patients and 2,887 carers. They concluded that of the predictor variables considered, disability levels and anxiety among stroke survivors, and depression, anxiety, and sense of coherence in their carers were associated with the highest effect sizes. A similar association between disability and degree of burden has been reported from India. 21 In our study we did not find motor disability to be a significant predictor of the high level of burden, probably because most of our patients (71.3%) had a low disability, and similar results have been reported previously by Sreedharan et al. 14 Neuropsychiatric symptoms and self-reported depression among patients were significant predictors of high burden in our patient population too. Only two studies in the review by Zhu et al. evaluated cognitive status as a predictor of high burden with moderate to large effect size. 24 We found the presence of dementia to be significantly associated with high burden and CDR sum of boxes to be significantly correlated with BAS scores. Freytes et al. also found that cognitive/emotional deficits were better predictors of caregiver’s burden than motor/functional deficits. 25 Other studies too have found that dementia is associated with a greater caregiver burden. 26 We did not find any caregiver factor significantly associated with a high burden.
Strengths and Limitations
Reintegration into society and engagement in productive employment to provide for themselves and their families continue to remain significant challenges for young stroke survivors and their carers. 27 However, there are very few studies that have specifically looked at the burden of caregiving in this group as our study has. We used standardized batteries were used for cognitive assessment, neuropsychiatric assessment, and burden assessment. As this is a hospital-based study, there may be an increased prevalence of stroke survivor morbidity compared to a community setting. Also, the BAS-20 does not evaluate financial burden. As young stroke survivors belong to the working age group but few have returned to work in our study population, similar to other stroke cohorts 28 ; there is likely to be a considerable financial burden on stroke survivors and their families. We did not specifically look for it as we felt this burden was likely to be universal and will be difficult to quantitate in our cultural setting. We did not evaluate many caregiver factors like anxiety or depression or coping skills which have been shown to have an effect on the burden of caregiving.
Conclusion
Our study suggests that even though most young stroke survivors have a low physical disability, most carers (84.7%) still report a subjective burden of caregiving. Traditional measures of stroke disability may be insufficient to predict the burden of caregiving for this group. Marital relations and relationships with others were two major areas of burden. Dementia and neuropsychiatric symptoms were associated with a greater burden of caregiving. More studies are required to understand the burdens, determinants, and needs of carers of young stroke survivors.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Institute ethics committee approved (JIP/IEC/2017/0450).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Informed written consent was obtained from the stroke survivors and their caregivers.