
Abstract
Introduction
Ischaemic stroke at young age carries an increased risk for mortality in comparison to the general population, but factors associated with mortality have been poorly studied. We studied the role of electrocardiogram in mortality risk stratification in young stroke patients.
Patients and methods
The Helsinki Young Stroke Registry encompasses 1008 patients aged <50 years with ischaemic stroke. We included 690 patients for this electrocardiogram substudy. Our endpoints were all-cause and cardiovascular mortality. Cox regression models – adjusted for clinical and demographic characteristics – were used to identify the electrocardiogram parameters associated with these endpoints.
Results
At a mean follow-up of 8.8 years, cumulative all-cause and cardiovascular mortality were 16.1 and 9.1%, respectively. Factors associated with both endpoints included diabetes (type 1 for all-cause, type 2 for cardiovascular mortality), heavy drinking, malignancy, as well as stroke severity and aetiology. Of the electrocardiogram parameters, higher heart rate (hazard ratio 1.35 per 10/min, 95% confidence interval 1.21–1.49), a shorter P-wave (hazard ratio 0.78 per 10 ms decrement, 0.64–0.92) and longer QTc interval (1.09 per 10 ms, 1.03–1.16) were associated with increased all-cause mortality. Only a higher heart rate (1.42 per 10/min, 1.24–1.60) was associated with death from cardiovascular causes.
Conclusions
A higher heart rate during the subacute phase after stroke is associated with an elevated risk of all-cause and cardiovascular mortality in young adults. A longer QTc interval is associated only with higher all-cause mortality. P-wave characteristics and their possible association with mortality need further studies.
Introduction
Ischaemic stroke (IS) is known to decrease survival in young adults.1,2 In this patient population, vascular diseases are the most common cause of excess mortality, while known factors increasing the risk for death include more severe stroke, increasing age, higher CRP levels, malignancy, heart failure, myocardial infarction, heavy drinking, type 1 diabetes (T1D), different stroke aetiologies, recurrent stroke, leukoaraiosis and accumulation of multiple risk factors.1,3–8
Since many electrocardiogram (ECG) findings are related to increased mortality in the general population, we hypothesised that ECG could be useful in assessing the risk of mortality in young patients with IS. Such findings in the general population have included intraventricular conduction delay (IVCD), left ventricular hypertrophy (LVH), T-wave inversions, P-terminal force (PTF), atrial fibrillation (AF), a wide QRS-T angle and bundle branch blocks (BBBs).9–16 In older stroke populations, pathological Q-waves, AF and a higher heart rate have been found as markers of higher mortality.17–20 In contrast, a large study on young stroke patients observed no association with AF and increased mortality. 21
To our knowledge, risk factors for cardiovascular death after stroke in young adults have not been systematically studied and the value of ECG findings associated with increased mortality has neither been studied. In this study, we assessed the risk factors for cardiovascular death in particular, and whether ECG abnormalities are associated with long-term risk of death after stroke in young adults.
Patients and methods
Study population
The relevant authorities approved the study, and it was carried out at the Departments of Neurology and Cardiology, Helsinki University Hospital. This retrospective study investigated data from the Helsinki Young Stroke Registry, with 1008 consecutive patients with first-ever IS aged 15–49 years and admitted to our hospital between 1994 and 2007. 22
Patients were examined according to a standard protocol, involving a 12-lead ECG on admission and, in most cases, also during the stay at the hospital. 22 To exclude changes related to the acute phase of stroke and obtaining an ECG close to baseline, we analysed ECGs taken 1–14 days after the onset of stroke symptoms and at least one day after admission. 23
Risk factors
We included in our analyses the following demographic factors: age and sex, and the following comorbidities: obesity, hypertension, smoking, dyslipidaemia, known AF, cardiovascular disease, T1D, type 2 diabetes (T2D) mellitus, malignancy and heavy drinking. Definitions of the comorbidities are described in detail in the online-only supplement (Table e1). Stroke characteristics analysed were NIH Stroke Scale (NIHSS) score on admission, stroke aetiology according to Trial of Org 10172 in Acute Stroke Treatment classification (with modifications to better adapt the classification for young patients; Supplementary Table e3), lesion size (ordinal scale ranging from 1 to 4) and lesion multiplicity (one or more lesions). 24 A lesion was defined as small when it was measured as <1.5 cm. A medium size lesion was defined as a lesion of a cortical superficial branch of the anterior, middle or posterior cerebral artery. A large anterior lesion involved the complete territory of the anterior or middle cerebral artery and a large posterior lesion involved the complete territory of the posterior cerebral artery with border zone territories.
Follow-up data
We obtained data on deaths and causes of death from Statistics Finland. The reliability of this register is described elsewhere. 25 Follow-up data were obtained until 31 December 2011.
Definition of endpoints
The primary endpoint was death from any cause. Our secondary endpoint was death from cardiovascular disease, defined as any of the three primary reasons (underlying cause of death, intermediate cause of death or immediate cause of death) being a diagnosis from 390 to 459 in ICD-9 or from category I in ICD-10. Death due to index stroke was counted as both primary and secondary endpoint regardless of time from stroke onset.
ECG analysis
JPi, blinded to clinical data at time of analysis, analysed the ECGs. In uncertain cases he consulted two senior cardiologists (ML and AA) for consensus.
We considered the continuous ECG parameters heart rate, P-wave duration, P-wave axis, PR interval, QRS complex duration, QRS frontal axis, T-wave frontal axis, corrected QT interval and QRS-T angle. The dichotomised ECG parameters we considered were IVCD, first-degree AV block, P-wave duration <80 ms, PTF, LVH, pathological Q-waves, J-waves (early repolarisation pattern), T-wave inversions, BBBs, prolonged QTc, rhythm, QRS duration >110 ms and frontal QRS-T angle >110°. Detailed definitions of ECG characteristics used in this registry are previously published. 23
Statistical analysis
We used the Cox proportional hazards model to investigate the factors associated with the endpoints. First, we performed a univariate analysis and determined which of the demographic factors, predefined risk factors and index stroke characteristics fell below significance level of P < 0.10. For both endpoints, a unique set of covariates was thus created for the multivariate analysis. Second, we tested all of the significant parameters in multivariate models, one model for each endpoint. The ECG parameters were then added – one at a time, in order to avoid overcorrection – into these models, creating an adjusted model for each ECG parameter. To correct for the performed multiple partly correlated ECG parameters, we applied a principal component analysis of all ECG parameters to define the amount of underlying uncorrelated components. The resulted number of components needed to explain 95% of the overall variability in ECG parameters was 8, which we used as a correction factor in Bonferroni correction. P < 0.05 was considered statistically significant. Kaplan–Meier survival plots were finally created to graphically demonstrate the major findings. We performed all analyses on SPSS 22.0 for Windows (SPSS Inc., IBM, Armonk, USA).
Results
A total of 690 patients fulfilled our inclusion criteria and were included in the present study. Of the original 1008 patients, four patients were excluded due to false primary diagnosis (stroke mimic), 48 due to unknown exact stroke date, 25 were treated only as outpatients and 241 had no ECG of good quality obtained during the required time window. Thirty-three patients (4.6%) received thrombolysis. Brain imaging was performed by either CT or MRI on all patients: CT was performed on 662 patients (95.9%) and MRI on 452 patients (65.5%). On 424 patients (61.4%), both imaging modalities were used. Compared with the excluded patients, the included patients had higher NIHSS score, longer corrected QT interval, wider QRS-T angle, more cardiovascular disease and a different distribution of stroke aetiology (Supplementary Table e3). Mean follow-up of the study cohort was 8.8 years (interquartile range 6.3–12.1). Supplementary Table e2 shows baseline comorbidities and medication data.
Mortality
Causes of 111 deaths during the follow-up.
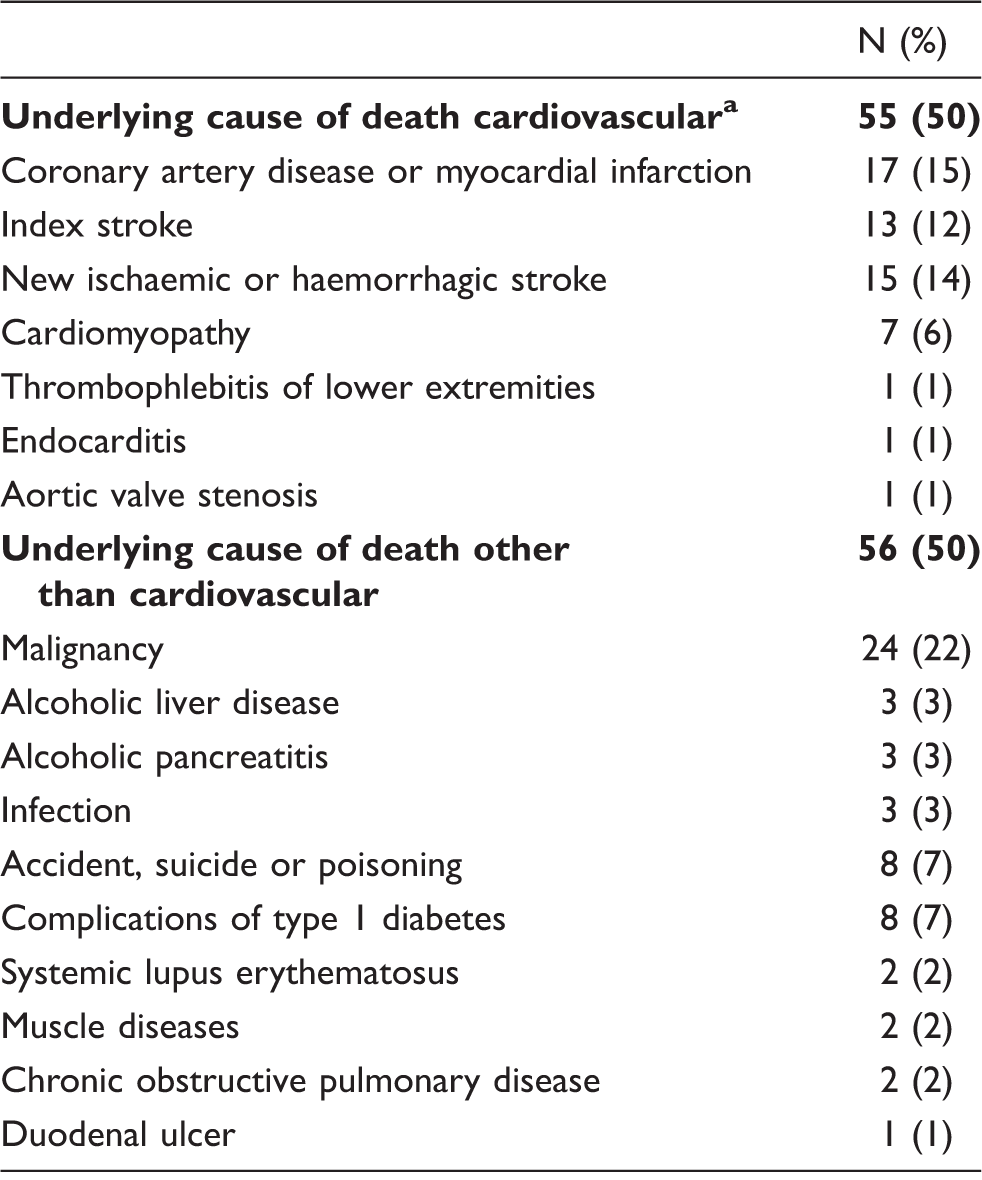
In addition to these, eight other patients had a cardiovascular intermediate or immediate of death, hence 63 patients in the cardiovascular cause of death group.
Association between demographic and clinical factors and long-term mortality
Risk factors for death from any cause. Multivariate analysis with Cox regression of different parameters and their hazard ratio: demographics, comorbidities and index stroke characteristics, only those significant in univariable analysis included.
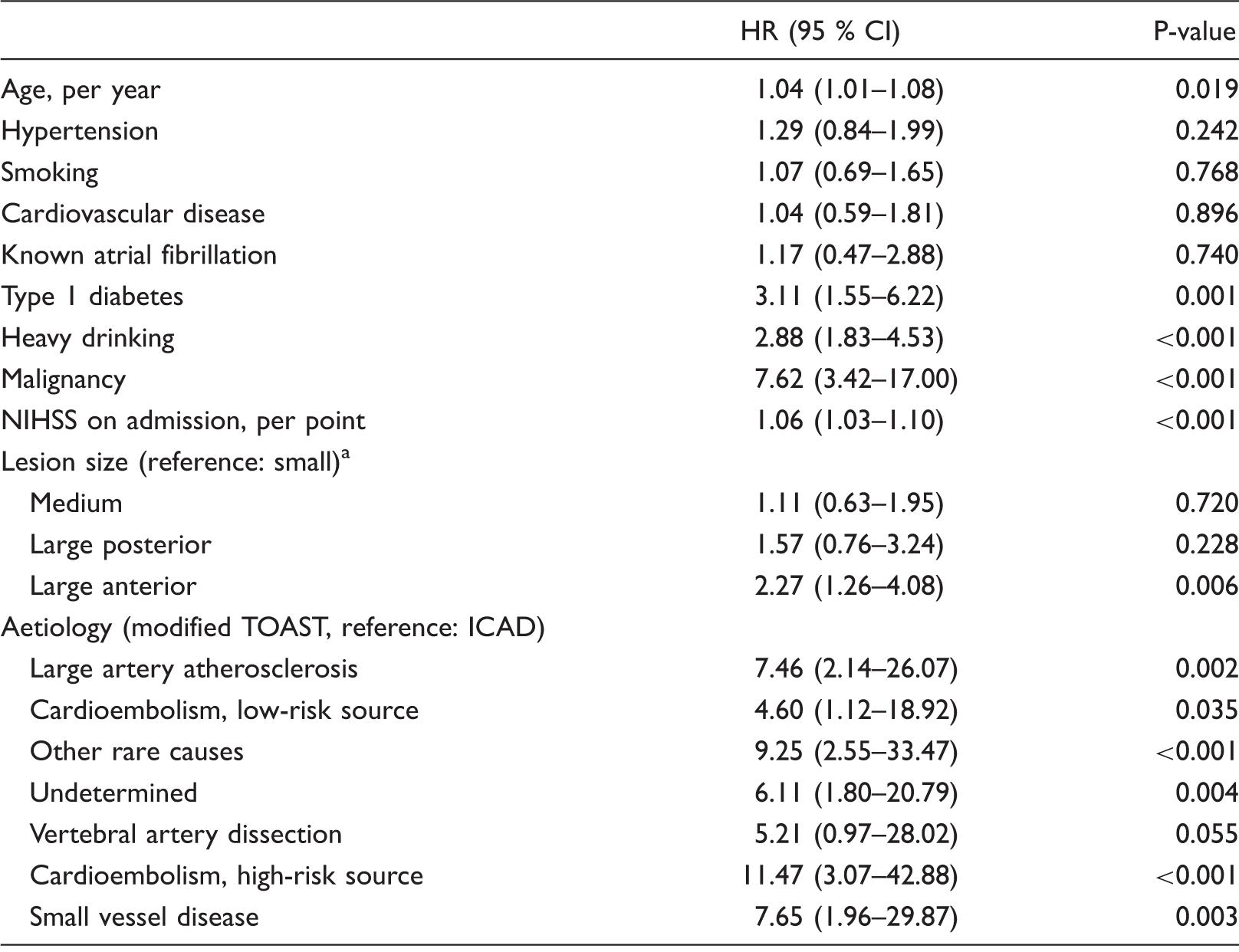
ICAD: Internal carotid artery dissection; NIHSS: National Institutes of Health Stroke Scale; TOAST: Trial of Org 10172 in Acute Stroke Treatment.
See methods for definitions.
Risk factors for death from cardiovascular cause. Multivariate analysis with Cox regression of different parameters and their hazard ratio: demographics, comorbidities and index stroke characteristics, only those significant in univariate analysis included.

ICAD: Internal carotid artery dissection; NIHSS: National Institutes of Health Stroke Scale; TOAST: Trial of Org 10172 in Acute Stroke Treatment.
See methods for definitions.
ECG findings associated with long-term mortality
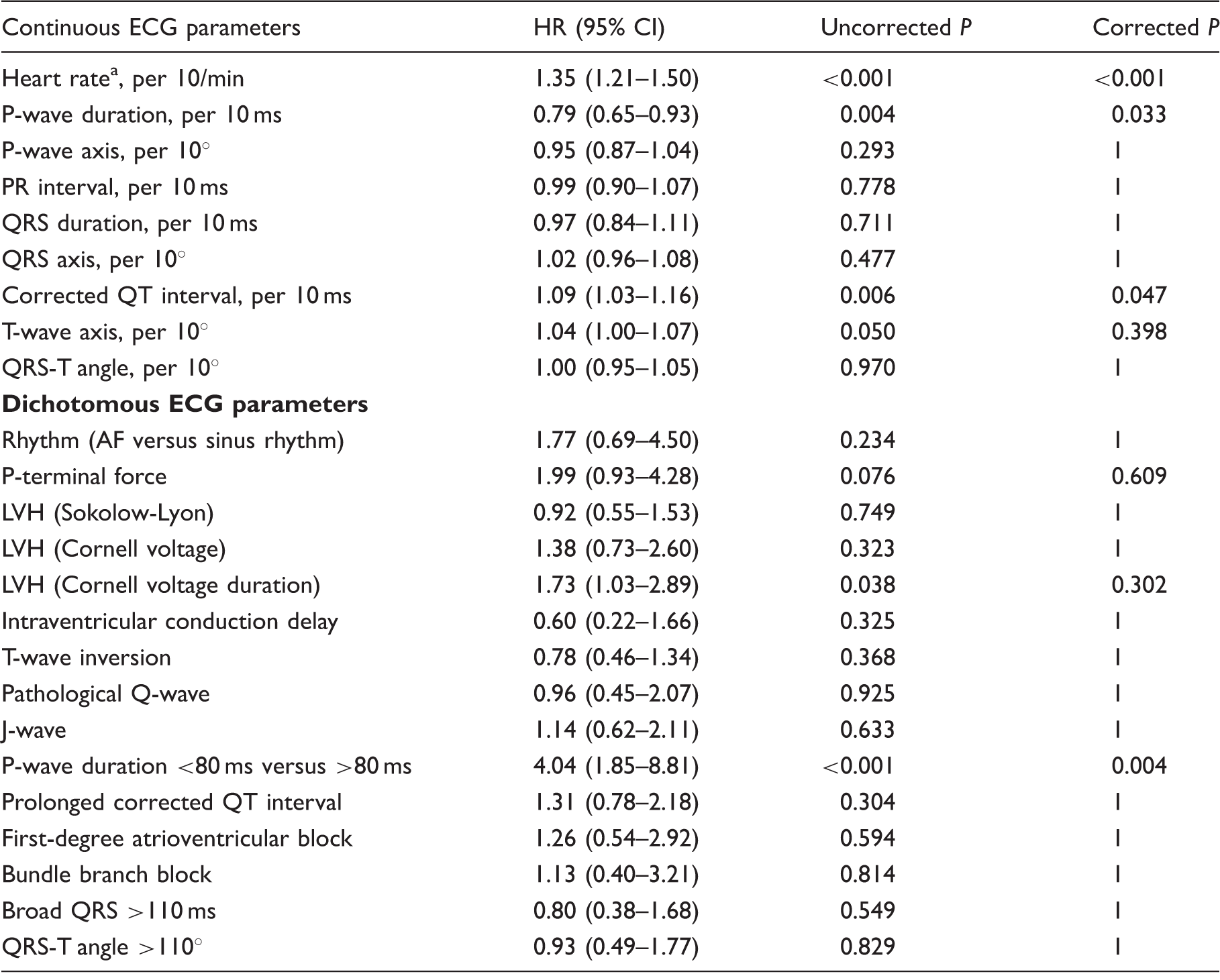
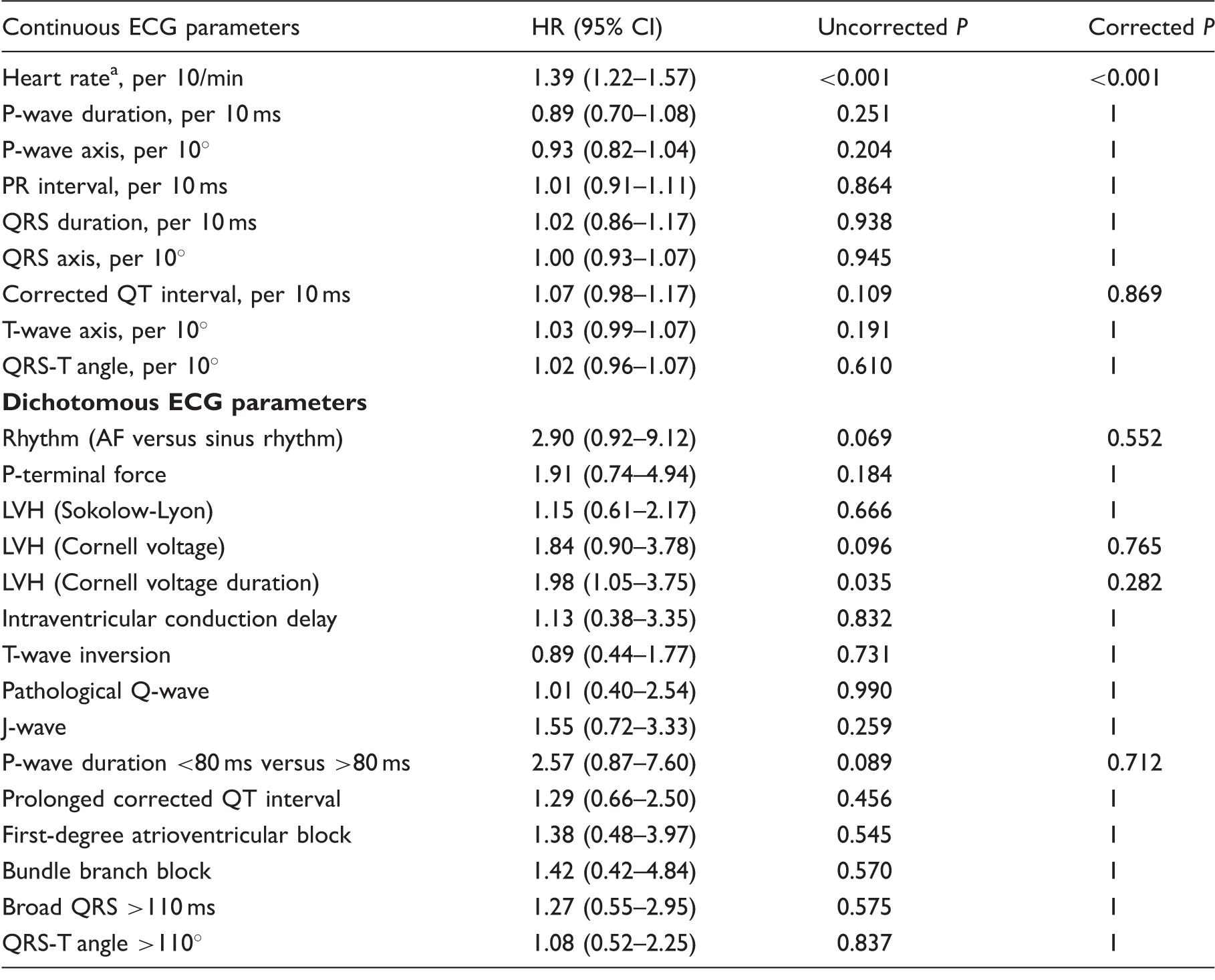
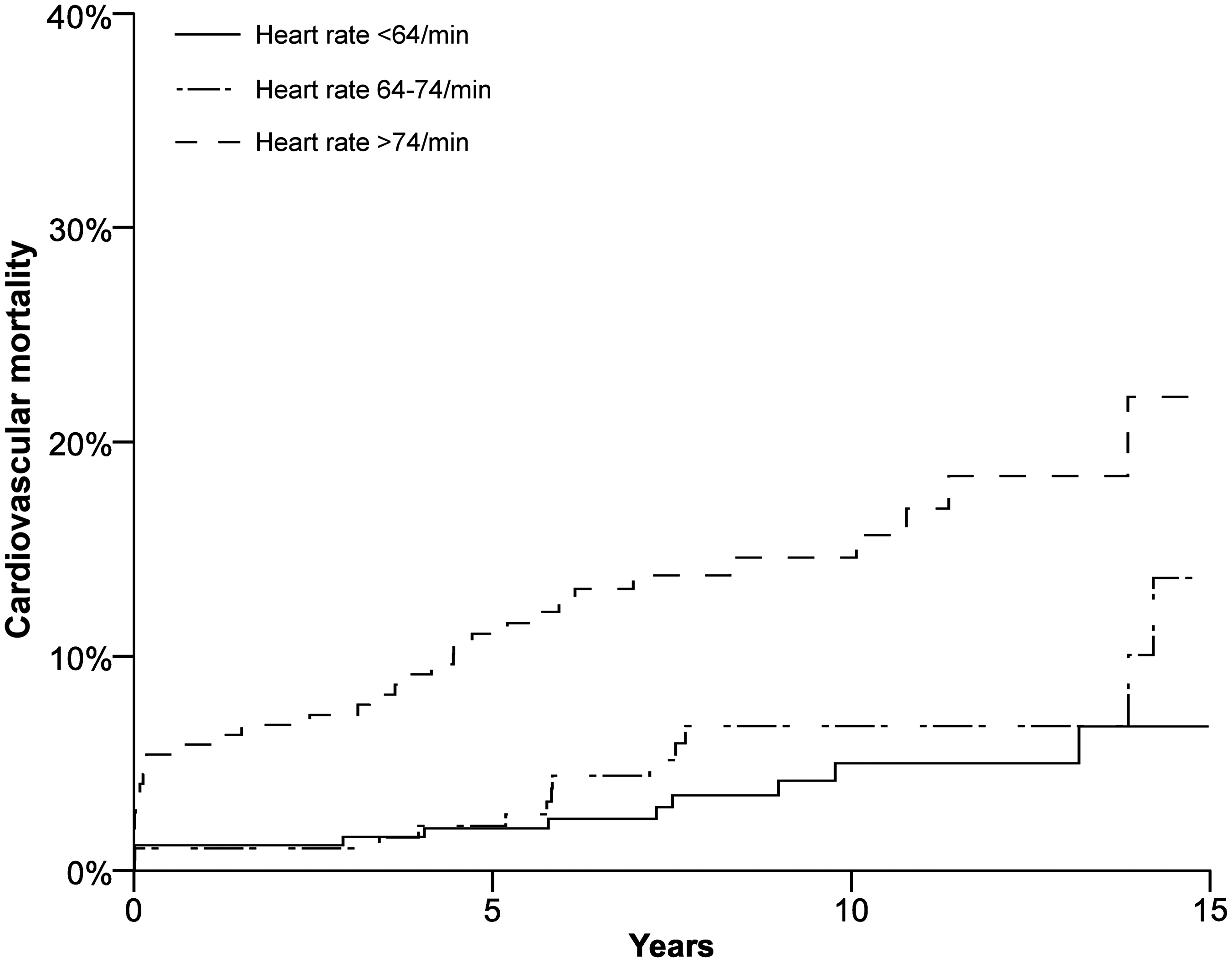
In the Bonferroni-corrected multivariate analysis, heart rate, QTc interval and P-wave duration were associated with death from any cause (Table 4). Only heart rate was statistically significantly related to cardiovascular death (Table 5). Kaplan–Meier survival plots of heart rate tertiles are presented for all-cause mortality and cardiovascular mortality (Figures 1 and 4).
Kaplan–Meier plot of heart rate tertiles and all-cause mortality. Log rank P < 0.001. ECG parameters’ relation to death from any cause. Multivariate analysis with Cox regression, adjusted for age, hypertension, smoking, type 1 diabetes, cardiovascular disease, known AF (except for rhythm), malignancy, heavy drinking, stroke aetiology, NIHSS and lesion size. AF: atrial fibrillation; ECG: electrocardiogram; LVH: left ventricular hypertrophy; NIHSS: National Institutes of Health Stroke Scale. Only considered for patients in sinus rhythm. ECG parameters’ relation to death from cardiovascular disease. Multivariate analysis with Cox regression, adjusted for age, hypertension, type 2 diabetes, cardiovascular disease, known AF (except for rhythm), malignancy, heavy drinking, stroke aetiology, NIHSS and lesion size. AF: atrial fibrillation; ECG: electrocardiogram; LVH: left ventricular hypertrophy; NIHSS: National Institutes of Health Stroke Scale. Only considered for patients in sinus rhythm.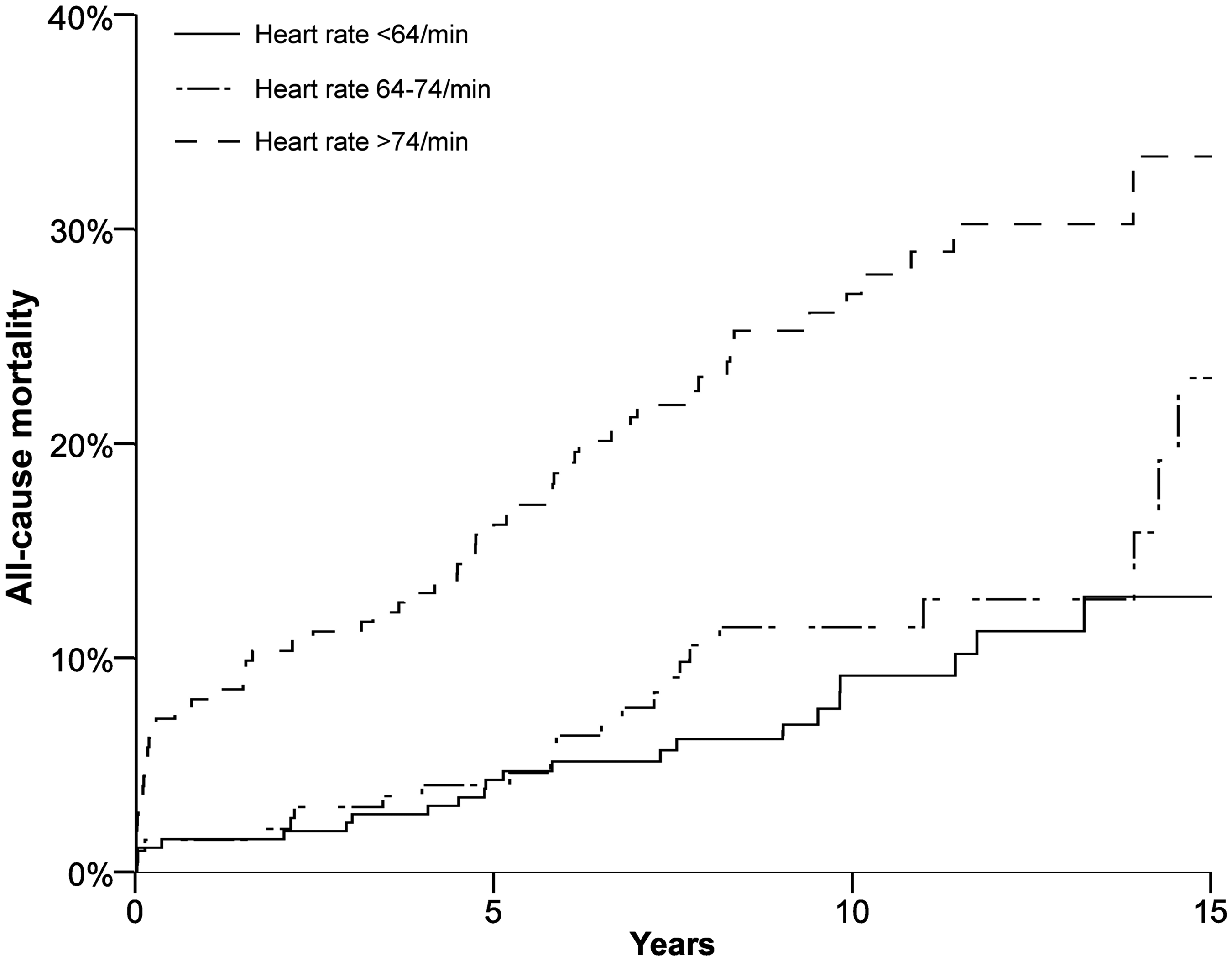
P-wave duration and all-cause mortality
We further investigated the role of P-wave duration and all-cause mortality. We tested dichotomising P-wave duration at a threshold of 80 ms. There were 16 patients with P-waves shorter than 80 ms, eight of whom died during follow-up. These patients had very variable causes of death, and only four of them died due to cardiovascular causes.
Discussion
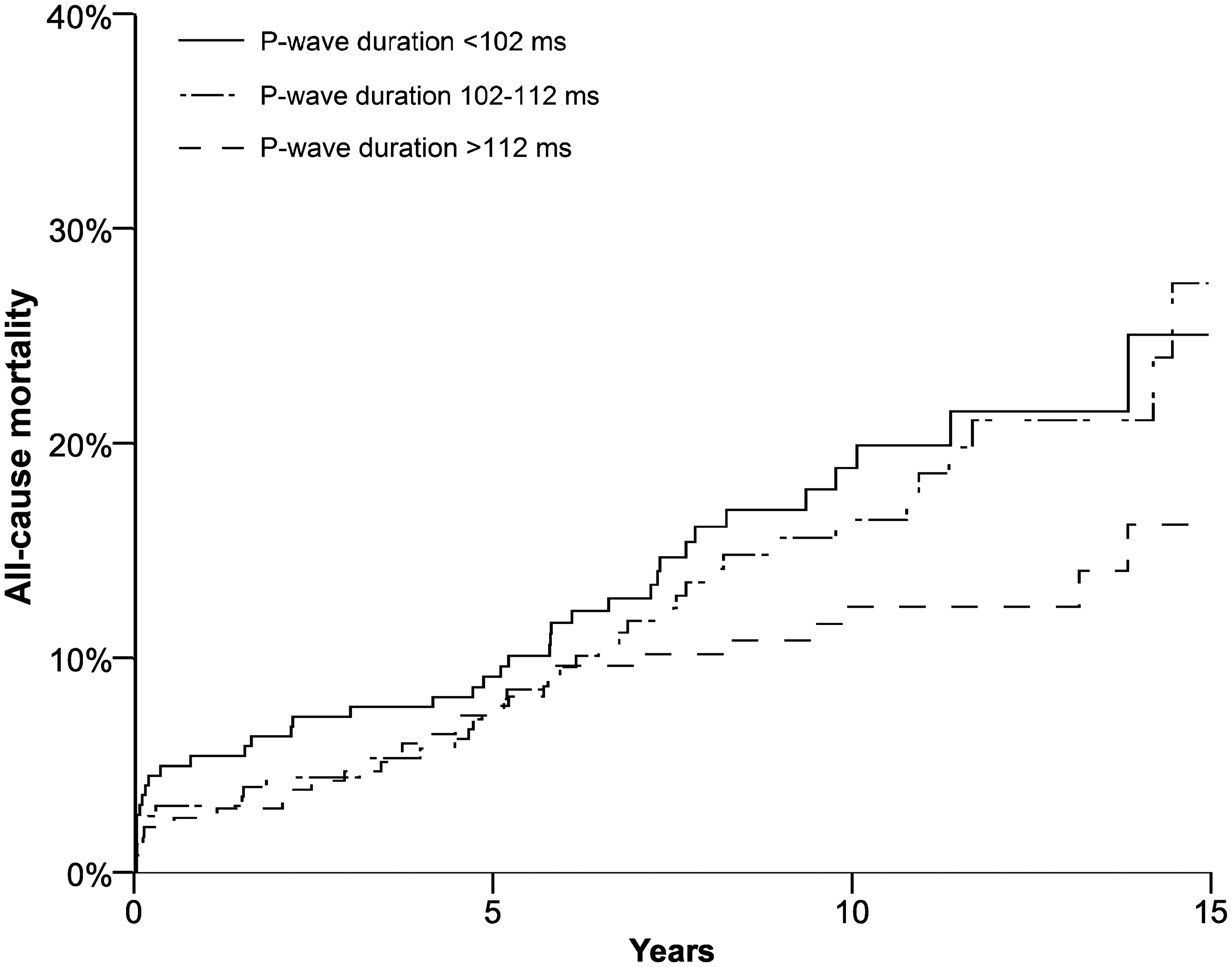
To our knowledge, this study is the first to identify ECG findings associated with all-cause and cardiovascular mortality in young adults with IS. It is the first study to reveal factors associated with cardiovascular mortality in young adults with an IS. A higher heart rate was related to increased all-cause and cardiovascular mortalities in our patients. We also found an association between a longer corrected QTc interval and all-cause mortality (Figure 2). We found a strong association between a short P-wave and all-cause mortality, however; due to the relatively small number of deaths and heterogeneous causes in this group, this most likely represents a chance finding. The non-significant association between P-wave duration tertiles and all-cause mortality emphasises the finding of only the very short, <80 ms, P-waves being significant in our study (Figure 3).
Kaplan–Meier plot of QTc interval tertiles and all-cause mortality. Log rank P < 0.001. Kaplan–Meier plot of P-wave duration tertiles and all-cause mortality. Log rank P = 0.129. Kaplan–Meier plot of heart rate tertiles and cardiovascular mortality. Log rank P < 0.001.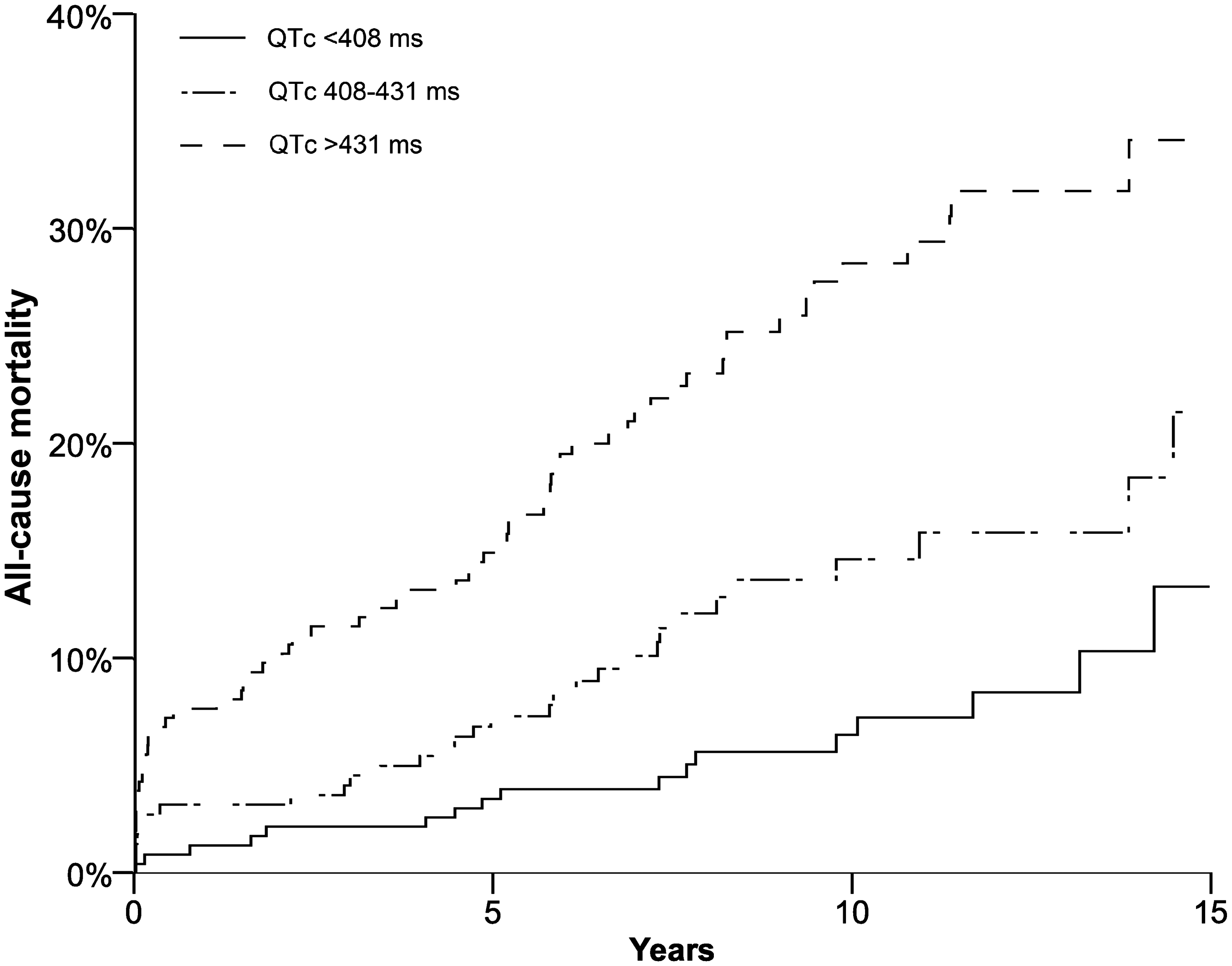
Higher heart rate was recently found to be associated with increase in in-hospital mortality in a large population of older stroke patients. 20 Although our study analysed the ECG in the subacute phase and not the acute phase, as in the study of Eldur et al., the results of both studies strongly suggest that heart rate is associated with mortality both in the elderly and also in the younger IS patients.
There are many hypotheses on why a higher heart rate is associated with higher mortality, observed in many patient groups. Higher heart rate has been linked to increased psychological stress, increased sympathetic tone, decreased vagal tone, lack of physical exercise, increased shear stress on arterial walls, inflammation in arterial walls, arterial stiffness, endothelial dysfunction, faster development of atherosclerotic lesions, reduced angiogenesis and myocardial ischemia due to a shorter diastolic time. 26
A longer QTc interval is also associated with higher mortality and cardiovascular mortality in the general population and even in older stroke patients,27–29 but quite surprisingly we did not find an association between longer QTc interval and cardiovascular mortality, yet one would specifically think the causes of death would be cardiovascular with this ECG abnormality.
It is rather surprising that we did not find an association of any other ECG parameters with mortality, since many of the parameters we analysed have earlier been associated with increased mortality (both all-cause and cardiovascular) in the general population, and AF and pathological Q-waves have been associated with higher mortality also in older stroke populations.9–19 As our patients’ causes of death were heterogeneous and the endpoint of cardiovascular death rather nonspecific, so it might be that other factors than cardiac electrophysiological abnormalities explain the risk of these endpoints.
The clinical factors associated with cardiovascular mortality were as could be expected known cardiovascular disease, heavy drinking, malignancy, markers of a more severe stroke (higher NIHSS score, larger lesion) and stroke aetiologies associated with existing cardiovascular disease (LAA, high-risk CE, other rare causes and small vessel disease). The fact that T1D was associated with all-cause mortality in this patient group was expected based on earlier findings.1,5 T2D being associated with cardiovascular, but not all-cause, mortality was a rather surprising observation, because both T1D and T2D increased both the all-cause and cardiovascular mortalities in the general population.30–32 T2D in the young adults with IS may be a more aggressive, early-onset form of T2D, and might have a poorer cardiovascular prognosis compared with a later-onset T2D. 33 This finding needs, however, further investigations in young adults and in other populations.
Knowing that a higher heart rate means higher mortality helps directing follow-up resources in stroke patients. A high heart rate, among other clinical findings could be a reason for taking a stroke patient to a ward with more intense control and moreover, considered as a signal of having increased risk of death. However, since the study was not an interventional study, it does not reveal the possible beneficial effect of lowering heart rate, e.g. with beta blockers.
Our study has its strengths and limitations. The strengths include a relatively large population of young IS patients with many variables considered for multivariate analysis, systematic analysis of a large scale of ECG parameters and a reliable database of deaths and their causes. Limitations include the retrospective nature of this study and relatively unspecific endpoints, representing various disease mechanisms.
Conclusion
A higher heart rate during the subacute phase of stroke is independently associated with a higher risk for death from any cause and from cardiovascular disease in the young with IS. Also, a longer QTc interval was associated with higher all-cause mortality. The importance of P-wave characteristics deserves to be further investigated.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The project was funded by the Heart Research Foundation (Sydäntutkimussäätiö). Jani Pirinen also received a grant from the Greta and Alfred Runeberg Foundation and Finska Läkaresällskapet.
Ethical approval
Ethical approval for this study was obtained from the ethical committee of the hospital district of Helsinki and Uusimaa (approval number 73/13/03/00/11).
Informed consent
Written informed consent was obtained from all subjects before the study.
Guarantor
JPi.
Contributorship
JPi: analysis of ECG strips, statistical analysis, obtaining follow-up data and drafting the manuscript. JuP: building up the patient registry and revising the manuscript. KA: obtaining follow-up data and revising the manuscript. ALA: analysis of ECG strips and revising the manuscript. SM: obtaining follow-up data and revising the manuscript. JS: obtaining follow-up data and revising the manuscript. MK: building up the patient registry and revising the manuscript. EH: building up the patient registry and revising the manuscript. TT: building up the patient registry and revising the manuscript. ML: analysis of ECG strips and revising the manuscript.
Acknowledgements
None.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.