
Abstract
This fast-moving global COVID-19 pandemic caught many nations unprepared and has exposed numerous flaws in global health, public health, and economic and social welfare infrastructures. It may seem premature to write about responses, but there are lessons to be learned from the response of Aotearoa New Zealand. Although its geopolitical situation as an island nation meant that it had late exposure to COVID-19, NZ has been commended because it closed its borders (to non-nationals); lockdown; traced; tested contacts; told people to pick a ‘bubble’ (immediate and usual family or household) and stay within that bubble; and promoted clear public messages. Government assistance was available for employers to retain staff, and additional support was provided for businesses and individuals. A strong and empathetic prime minister communicated regularly with the public and developed a sense of common national purpose. However, COVID-19 still exposed the impact of social inequalities. Implications for the next steps of recovery are considered in the paper.
Introduction
Writing about the COVID-19 pandemic while still in the midst of the global outbreak is a risky undertaking. Anything we say now may well be out of date, short-sighted or simply proven wrong in a few days, weeks or months. This fast-moving global pandemic has caught many nations unprepared and has exposed numerous flaws in the global health, public health, and economic and social welfare infrastructures, even though this scenario was predicted by health experts decades ago (Garrett, 1994, 2001). The dismantling of these infrastructures, either by design or neglect, has made the current crisis inevitable. We have frequently heard the COVID-19 pandemic called ‘unprecedented’, although to call it so is to ignore numerous similar devastating events in human history (Jarus, 2020), and even in the last few decades. It is usually commentators in the developed world who use the word unprecedented about the pandemic, and the notion rings hollow to those of us who were part of the global response to HIV. Assessing national responses to COVID-19 now, however, may establish a kind of framework for lessons learned so far to support the recovery from the current crisis and prepare for the next, inevitable one. It may also help us to identify particularly vulnerabilised populations where social inequities have been laid bare by this virus, just as they were identified during the height of the HIV epidemic. It is in this spirit that we may consider the Aotearoa New Zealand (NZ) experience as a kind of case study.
Country Profile
Aotearoa New Zealand (NZ) is a small island nation of nearly five million people situated in the southwestern Pacific Ocean. Its geographic isolation has been a key in both the timing of the appearance of the virus and the nature of the government response. NZ is a bicultural nation with a formal treaty relationship (the Treaty of Waitangi, signed in 1840) between indigenous Māori iwi (tribes) and the British Crown, now represented by a Westminster-style Parliament with a Prime Minister as head of Government and Governor General (who represents the Queen) as head of State. Although the Treaty of Waitangi is considered part of the constitutional arrangements of the country, NZ is also a very multicultural country: In the 2018 Census, 70.2 per cent of the population were identified as European (in other countries called ‘Caucasian’ or ‘white’), 16.5 per cent were Māori, 15.5 per cent were Asian, 8.1 per cent were Pacific Island, 1.5 per cent were Middle Eastern, Latin American or African (MELAA) and 1.2 per cent were all others (these are self-reported and non-exclusive categories, so the total exceed 100%). The three official languages are English, Māori and New Zealand Sign Language; after English and Māori, the most widely spoken languages are Samoan, Northern Chinese (Mandarin) and Hindi; other widely spoken languages include Yue (Cantonese) and other Sinitic languages, Tongan, Tagalog and Afrikaans (all data from StatsNZ/Tatauranga Aotearoa, n.d.). Kiwis (as New Zealanders are often called, after the endogenous flightless, nocturnal bird, not the fruit) travel widely, and it has been anecdotally estimated that at any given time as much as 15–20 per cent of the population may be overseas (StatsNZ/Tatauranga Aotearoa, 2012). This means that Kiwis collectively have a lot of international travel experience, which we would expect from an island nation, but it also has implications for managing a global viral pandemic.
NZ is a gateway to the Pacific Island nations and territories, which puts a significant responsibility on NZ, not only for transport and international development aid but also for public health. The memory of the 1918 influenza epidemic (Kahukura-Iosefa, 2018), brought to Samoa by the NZ ship Talune, is very much alive. The Talune was allowed to dock rather than remain in quarantine, although it had passengers on board infected with influenza; over 8,000 Samoans, 22 per cent of the population, were killed by the resulting epidemic. More recently, between September and December 2019, there was a measles outbreak in Samoa which resulted in over 5,700 cases of measles and 83 deaths; measles was also widely reported in Tonga and Fiji. While the spread of measles has been attributed to low population vaccination rates in Samoa, it is thought that an infected passenger on a flight from NZ to Upolu in August 2019 sparked the outbreak (Deer, 2019). As a consequence, travellers from NZ (which was undergoing its own measles outbreak) were barred from entering many Pacific Island nations and territories during the outbreak. The Samoan influenza and measles experiences create a regional backdrop for NZ’s responsiveness to COVID-19.
COVID-19 in Aotearoa New Zealand
The first case of COVID-19 was reported in NZ on 28 February 2020 in a NZ resident returning from Iran. The NZ Government had been closely monitoring the outbreak in the People’s Republic of China (PRC) and other countries (including Korea, Italy and Iran), so this case was not unexpected. In fact, on 3 February 2020, the government had announced that foreign travellers leaving PRC would be denied entry to NZ, and that only NZ citizens and permanent residents would be permitted to enter NZ. Despite strong representations from the NZ tertiary education sector, the exclusion was also applied to Chinese and other international students enrolled in NZ courses of study. This was a particularly unwelcome decision as international students are considered essential for the economic well-being of the NZ education sector (which is almost entirely public, and chronically underfunded). Returning nationals from Iran and Italy, and passengers from cruise ships (and their contacts) were the earliest reported cases of COVID-19 in NZ. By 21 March 2020, there were 52 cases in NZ, of which only two did not have links to overseas travel. 1 At this writing (early May 2020), 72 per cent of cases had direct links to overseas travel (Ministry of Health/Manatū Hauora, 2020b), and most of the others had links to those cases.
On 21 March 2020, the Prime Minister, Jacinda Ardern, announced the establishment of a four-stage ‘alert’ level system: 2 Level 1 (Prepare), Level 2 (Reduce), Level 3 (Restrict); Level 4 (Eliminate) is the highest risk, requiring a compulsory ‘lockdown’ of individuals and businesses. On 23 March 2020, an Epidemic Notice was issued, and Level 3 was announced with its significant restrictions on personal movement, social contact and travel. Two days later, a national state of emergency was declared, roughly 12 hours before an announced move to Level 4. At Level 4, the entire population was instructed to remain in their homes and associate only with those in their ‘bubbles’ (i.e., their immediate and usual family or household). All public gatherings of any size, including funerals and tangihanga (Māori cultural funeral rituals), were banned; all non-essential businesses, educational institutions, bars and restaurants (including takeaways), liquor stores, gyms and pools, and personal care (e.g., hairdressers) services were required to close. Essential workers (who included health, pharmacy, residential care workers, first responders, public safety, grocery store and food distribution workers, veterinary services, and the media, among a limited group) were permitted to work under strict protocols governing personal interactions. Physician appointments, for example, were managed online or by telephone in the first instance. Some essential social services remained available, including people who worked or volunteered at crisis hotlines, food banks, homeless shelters and services, child protection, and family violence agencies. Ground travel was severely curtailed during the four weeks of Level 4 and on two long holiday weekends during the period, when people would ordinarily travel to vacation spots or holiday homes, police checkpoints were established, and violators turned back. The border was closed (and remains closed at this writing), and all international and domestic air travel were suspended except for a few government-arranged relief flights to repatriate Kiwis who had been stranded overseas by various travel bans, and airline and marine crews. (The Ministry of Foreign Affairs and Trade rejected advice for a complete border closure as politically untenable: It could not see barring citizens and residents from returning.) All arrivals were (and are) required to undertake a 14-day government supervised quarantine on their return to NZ (Ministry of Health/Manatū Hauora, 2020a).
NZ is a significant tourist destination, and the extent of the Level 4 restrictions and the speed of their implementation took many people by surprise: Some tourists could not find flights out of the country (or to international airports) in time, and some had to remain in hotels, hostels or campgrounds at tourist spots (Neal & Brunton, 2020). There were a few violations of Level 4 restrictions, and police had the authority to enforce and prosecute where necessary. Communities with high numbers of Māori residents saw impromptu checkpoints and blockades staffed by Māori volunteers on their roads preventing non-residents from entering those communities (Williams & Biddle, 2020). These blockades became a point of tension because although they were not strictly legal, police were reluctant to confront or dismantle them since sovereignty over land is guaranteed to Māori by the Treaty of Waitangi.
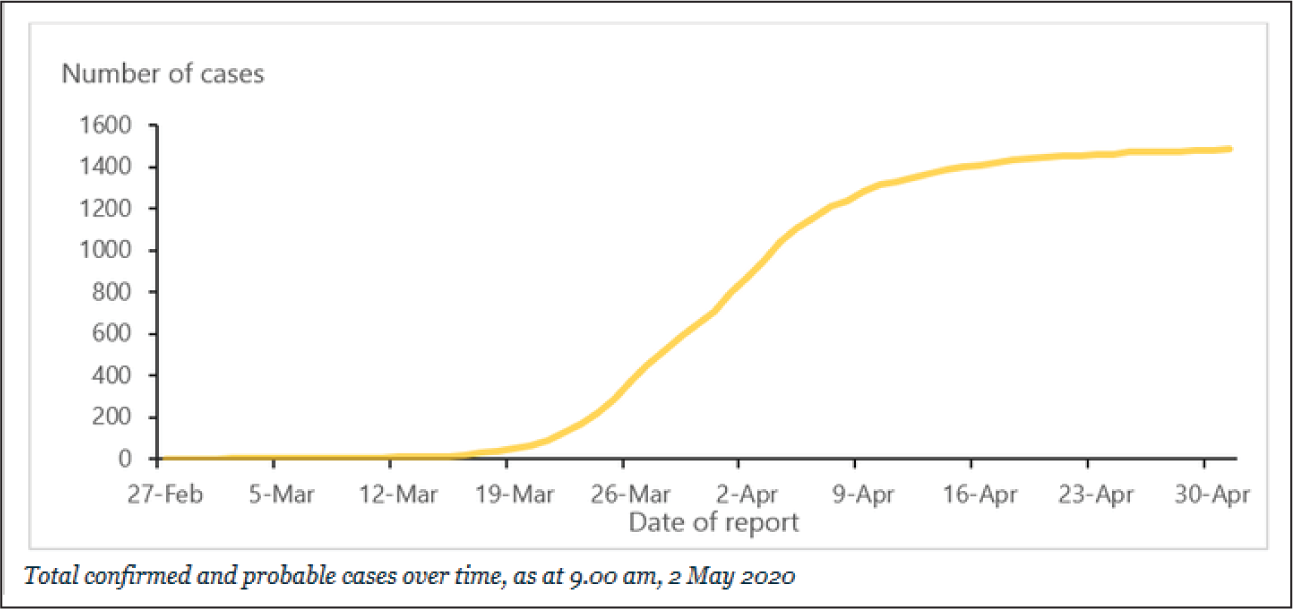
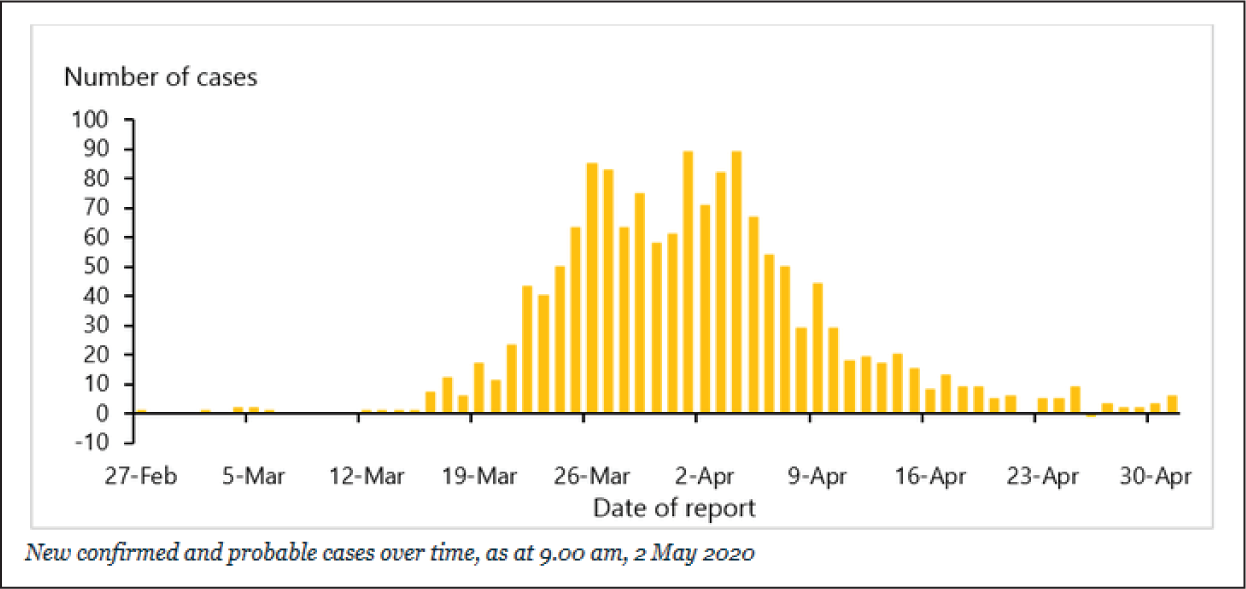
On 19 April 2020, daily reports of new cases dropped below 10, and on 28 April 2020 the country moved back to Level 3 (Figures 1 and 2). On 30 April 2020, the government announced that some businesses (such as construction and forestry), takeaway restaurants and businesses using ‘click-and-collect’ (online ordering and delivery or contactless in-person collection) shopping for essential items were permitted to open under strict regulations governing personal contact. Limited recreational activities (such as surfing and beach swimming) were permitted. Some children (particularly children of essential workers) were permitted to return to their classrooms, although teaching at all levels—including research supervision and meetings—remained—and will remain—online, possibly for the remainder of the calendar year.
Testing kits gradually became available, and testing for COVID-19 ramped up to 8,000 tests per day, with 145,000 community tests done by 1 May 2020. On 18 April 2020, the testing rate for Asians was 10.8 per 1,000; for Europeans/Other and MELAA was 15.9; for Māori was 15.8; and for Pacific peoples was 19.4, for an overall rate of 15.4 per 1,000. (Ministry of Health/Manatū Hauora, 2020b). Contacts for all cases were traced and notified (although the systems to do this were initially criticised as inadequate), to the point where the Ministry of Health/Manatū Haurora asserted that 80 per cent of close contacts were notified within 48 hours of the case diagnosis (BBC News, 2020b). By 1 May 2020, the total number of cases had reached 1,485 (1,134 confirmed and 351 probable), the total recoveries were 1,263 or 85 per cent. There were 20 deaths attributed to COVID-19, mostly in residential aged care facility residents (Ministry of Health/Manatū Hauora, 2020b). Ministry of Health data show that as on 1 May 2020, 73 per cent of COVID-19 cases have been among European or Other New Zealanders, 9 per cent among Māori, 12 per cent among Asian, 5 per cent among Pacific peoples and 1 per cent are unknown (these are exclusive categories), roughly paralleling the population ethnicity distribution in NZ.
On the day that the country moved to Level 3, Prime Minister Ardern became the focus of global media coverage when she announced that NZ had ‘eliminated’ transmission of COVID-19, and she said ‘We can say with confidence that we do not have community transmission in New Zealand’ (Radio New Zealand, 2020b), although some public health experts noted that ‘eliminate’ had not been clearly defined. Ardern and her staff also warned that residual pockets of virus would need to be managed as the country emerged out of its complete lockdown.
What Government has Done Well
NZ’s Prime Minister, along with her senior ministers and health administrators, has been widely respected during this crisis. Prime Minister Ardern is the leader of a centre-left coalition government and is a formidable communicator who is respected by allies and political opponents alike. She has enjoyed an 80 per cent public approval rating during this period, and she and various ministers and senior health staff held press conferences at 1 pm each day which became must-see TV. These daily briefings, public service messages in multiple languages, an up-to-date dedicated government website 3 and special sections on the usual Ministry of Health/Manatū Hauora, Statistics New Zealand/Tatauranga Aotearoa 4 and Ministry of Social Development/Te Manatū Whakahiato Ora 5 websites rely on science and hard data rather than partisan politics, and have provided clear messages, and transparency to the public, almost in real time. This is the same Prime Minister, it should be noted, who also managed the Christchurch mosque shootings in March 2019 which resulted in 51 deaths, and the Whakaari/White Island volcanic eruption in December 2019 which resulted in 21 deaths, with empathy, resolve and grace. She also became the second world leader in modern history to give birth, to a daughter, in June 2018, and at the age of 39 is the youngest prime minister in NZ since 1856. During the COVID-19 crisis, she has empathised with the difficulties of lockdowns and encouraged a mutuality of response across all sectors of the country. She has appeared at formal press briefings, and also casually dressed on Facebook Live chats; she has reassured children that the Tooth Fairy and Easter Bunny are essential workers during COVID-19 Level 4. She and her ministers have popularised the term ‘physical’ rather than ‘social’ isolation, recognising that socialising safely was an essential way of gaining the trust and collaboration of the nation for the restrictions placed on them.
Aotearoa New Zealand clearly has enjoyed some advantages in its approach to managing the COVID-19 crisis: It is a fairly remote island nation with clearly defined and monitored borders. COVID-19 was a relatively late arrival in NZ, and so officials had the advantage of watching the Chinese, Korean, Iranian and Italian experiences, as well as the spread of the pandemic in Europe. NZ is a small country, with a relatively low population density (except in the major cities), although there are strong cultural, social and relational networks. Much of the country trusts a strong central government in times of crisis, and adheres to public health and safety messages that have been clearly explained and make sense. There was a certain amount of panic buying when Level 4 was announced, but that passed reasonably quickly when people realised the country was not going to run out of toilet paper.
An analysis by overseas media (BBC News, 2020b) found that NZ has done a number of things right in its national response to COVID-19:
It closed its borders (to non-nationals);
It had a quick and clear lockdown;
It traced and tested contacts;
It told people to pick a ‘bubble’ and stay within that bubble;
There were clear public messages.
Since NZ is a small country, there is a strong central government and limited local government (although local councils applied bans to public gatherings, theatres, libraries, recreational and other facilities at the same time the central government called for such measures), and so coordination of the response was national and centralised. The national response was led by epidemiological data and health scientists, who were widely sought for commentary in the media. There were reasoned debates among public health experts about the extent of the Level 4 lockdown and its temporary suspension of some civil liberties, to which government responded, and minimal public protest (after an initial and widely condemned outburst in Parliament by the Leader of the Opposition, a centre-right party; it was considered unseemly and untimely by all parties and the general public to threaten a unified national response in a time of crisis). Moving out of Level 3, the length of time that the social and other public restrictions will be imposed will no doubt occasion much more public debate among the commentariat.
In addition to these measures, early in its response, the government announced a package of support worth NZ$5.3 billion in wage subsidies that would support businesses to pay workers up to 80 per cent of their normal wages or salary rather than making staff redundant (Carroll, 2020b). Additional business support was made available through banks on guaranteed loan schemes, deferred tax and tax compliance relief, and special support for Māori businesses and iwi responses. Banks, insurance companies and utilities (e.g., power companies, telcos) also made support available through mortgage holidays, lifting data caps and other measures (Carroll, 2020b). As a show of solidarity with people who had been made suddenly redundant or furloughed, the Prime Minister and her senior ministers all took a voluntary six-month 20 per cent reduction in their own pay. Additional recovery support is currently working its way through normal Parliamentary procedures as government turns from crisis management to a more usual and sustainable way of operating.
Future Shock
However, we are in only the first wave of the pandemic, and the public health crisis is only the leading edge of what will inevitably be major social and fiscal shocks both globally and in NZ. Financial commentators are predicting three major waves of redundancies: the first when government subsidies run out and employees are made redundant; the second when businesses begin to fail; and the third when the full fiscal impact of the global pandemic begins to take hold in a year or more. The Finance Minister Grant Robertson said, ‘This is the rainy day we have been planning for. We hope to save some jobs, but we won’t be able to save all jobs’ (Farmers Weekly, 2020). Unemployment or underemployment and failing businesses will inevitably mean falling tax revenue at the very moment the country has pledged what are vast sums for a relatively small country. NZ relies heavily on tourism (21% of NZ’s export goods and services, nearly 10% of GDP) and trade in agriculture (5% of GDP) and forestry (1.6% of GDP), and it is particularly vulnerable to international economic forces at the best of times; the full global economic impact of COVID-19 is not at all clear at this writing. NZ’s major trade partner is the PRC (20% of goods), and it may be some time before that trade relationship is normalised. Some commentators are predicting a major global depression similar to that of 90 years ago. The fast-food giant Burger King has already filed for receivership (bankruptcy) as a result of the pandemic (Carroll, 2020a), and other businesses, small and large, are threatening to follow.
Air New Zealand, the national carrier, reduced its domestic and international flights by 95 per cent as a result of the border closure and domestic lockdown. It has estimated that its revenue could result in the loss of NZ$5 billion (on a reported operating revenue of NZ$5.8 billion in 2019), and it has already announced plans to make at least 12,500 employees redundant (Cropp, 2020), including 300 pilots (Radio New Zealand, 2020a). In 2018, Air New Zealand employed 8.4 per cent of NZ’s total workforce (Air New Zealand, 2018), so the economic and personal impact will be substantial. Since nearly 80 per cent of freight to and from NZ is usually carried on passenger airline services, the national implications for trade and the availability of goods is also significant. The airline will inevitably require additional support or concessions by government, which owns 52 per cent of Air New Zealand. Since Auckland is a major airline hub to access destinations throughout the Pacific, the implications of these reductions reach far beyond the national borders.
Continuing Challenges for Rich and Poor
Government’s approach of ‘go early-go hard’ was not without controversy, as businesses—particularly in the tourism and hospitality sectors (which generated NZ$11.2 billion in 2018) on which the national economy is so dependent—experienced a complete loss of income, and associated sectors (e.g., rental accommodation for workers) were also affected. While some workers could work from home, many others—particularly in the retail and services sectors—could not, and they experienced a significant or complete drop in income if their employers could not continue to employ them full- or part-time.
As always, the most fragile sectors of the population are enduring the economic effects of the pandemic effect. A social impact report by the Salvation Army (Social Policy & Parliamentary Unit, 2020) noted that social and policy issues such as food insecurity, financial hardship, addictions, housing and income support, and employment that predated the COVID-19 crisis were being exacerbated by the pandemic and the government’s response. In particular, NZ was already experiencing a significant housing crisis, with 15,235 people on a waiting list for social housing and a total of only 70,738 homes available. Jobseeker benefit claims grew by 26 per cent in the first three weeks of the Level 4 lockdown, and there is an expectation that by the end of 2020, unemployment will double from 4 per cent which was at the end of 2019; this translates to an expected 270,000 unemployed persons. The report also notes that Māori and Pasifika workers and communities have been the most vulnerable to COVID-19-associated unemployment because they already had unemployment rates more than twice that of the rest of the workforce. Even in Level 3, there are some inequalities because shopping must be done online in most cases, and cash is not accepted; therefore, anyone who does not have access to a computer or Wi-Fi or a bank account or a credit card is disadvantaged. The expression ‘COVID-19 underclass’ (Scoop, 2020) entered the policy discourse during the Level 4 period to reflect how especially vulnerable Māori and Pasifika peoples are, not only to public health crises but also to economic downturns more generally. Fortunately, no cases have been reported from prisons in NZ; since NZ has one of the highest incarceration rates in the Organisation for Economic Co-operation and Development (OECD) and a large proportion of the prison population have chronic health conditions, an outbreak of COVID-19 in the prisons would be catastrophic. The Department of Corrections and the unions are working collaborative to put robust prevention measures in place, but there are no expectations of unplanned inmate releases as we have seen in other countries. In Auckland, the largest city, particular outreach efforts were made to shelter homeless persons in motels for the period of the lockdown, with extra volunteers recruited to support them; nevertheless this writer saw several people sleeping rough during the lockdown period. The COVID-19 crisis again has highlighted inequalities and weaknesses in the health, public health, economic and social policy infrastructures in which vulnerabilised populations are embedded.
One of the unanticipated impacts of COVID-19 and the border closures will be on street drugs. While most street drugs used in NZ are manufactured in NZ, precursor materials for methamphetamine (the most widely used drug after alcohol and cannabis) must be sourced from overseas, particularly from Myanmar and Mexico. Since there are virtually no incoming international flights, and container traffic has been disrupted (Vance & Ensor, 2020), methamphetamine prices doubled in the South Island during the lockdown (Ensor, 2020). This is likely to drive up demand for other drugs, put pharmacies at increased risk of burglaries and push gangs who manufacture the drug to become more creative in sourcing precursor supply.
Where to from here?
Just as it is risky to write about the impact of COVID-19 in the midst of the developing response to the pandemic, it is also risky to write about what may happen in the future. The expression ‘return to normal’ is fading in the public discourse, and is being replaced by ‘the new normal’. As the Age of Terrorism affected politics, business and travel around the world over the last 40 years, there is increasing awareness that Aotearoa New Zealand, and probably most of the world, has entered a new era, the Age of Viral Anxiety. If governments and economies attempt to preserve (or return to) life as it was, then it is likely that economic inequalities will be further exacerbated: The wealthy will continue to become wealthier, and the poor will be poorer, hungrier, unhealthier and angrier than they were before the crisis. It is not impossible that in some developing countries there will be widespread social upheaval. Street riots are unlikely in NZ; however, protests and hikoi (Māori protest marches) are quite imaginable as economically fragile communities recognise the extent to which they have been marginalised and vulnerabilised by capitalist and neoliberal policies. NZ adopted the Thatcher–Reagan neoliberal attitudes and policies in a form dubbed ‘Rogernomics’ in 1984 (after Roger Douglas, the Finance Minister of the Fourth Labour Government). As a consequence, NZ, where the saying ‘Jack’s as good as his master’ expressed the egalitarian spirit of early colonialism, has become increasingly unequal (Newshub, 2018); the 2018 GINI index was 32.5 per cent, in the top three of the most unequal countries in the OECD. The wealthiest 10 per cent of the population own nearly a fifth of the wealth, while the poorest 50 per cent own less than 5 per cent (Rashbrooke, n.d.). Housing costs have skyrocketed to the point where Auckland, home to one-third of the population, is counted among the most expensive cities to live in the world (Cox & Pavletich, 2019).
The NZ government, like developed economies around the world, has an opportunity to reconsider its political and economic philosophies and policies as a result of the COVID-19 pandemic. It will be paying for its economic support of workers and businesses and for strengthening health and public health infrastructures for many years, possibly generations. Even with a viable and affordable vaccine—unlikely in the next several years—and an equitable distribution network, it is unlikely that COVID-19 will ever be completely eliminated from every nation or region. In the Pacific, we would need to see vaccine administered not only in NZ but also in Australia, other Pacific Island nations and territories, and much of East and South Asia before travel restrictions are lifted. We will probably see localised outbreaks for decades to come. In a generation which has seen regional and global outbreaks of diseases such as SARS, MERS, Zika and Ebola before COVID-19, where we insist on the destruction of rainforest habitat (Zimmer, 2019) and ignore the public health impacts of climate change at our peril, we have clearly not seen the last of novel pathogens. Lurching from lockdown to lockdown is unsustainable, economically, socially or politically. Rising social and economic inequalities, the end of one-career (or employer)-for-life, the emergence of the so-called gig economy, the role of cash, and the increasing flexibility of the virtual world invite, or demand, a reconceptualisation of work and of capitalism in its various forms. The notion of a universal basic income has resurfaced in public discourse as an alternative to existing models of social welfare (Manch & Cooke, 2020; St John, 2020). This means that the goals (and methods) of education and skills training in secondary schools, polytechnics and universities will need to be reconsidered and reconfigured. The Age of Viral Anxiety may also mean that the health and social sciences may be more attractive to students and government funders.
Despite, or perhaps because of, its unique geopolitical context, we in Aotearoa New Zealand have learned some lessons from COVID-19. Most importantly, we have learned how important it is to have trustworthy governments and empathetic political leadership that are led by science and not merely by politics, polls or personal ambition. We have learned that governments must respond to a pandemic crisis as it is, and not how they would wish it to be. We have learned that it is important to have political leadership who is willing to take advice from people knowledgeable in their fields and to be ready to respond to the changing on-the-ground realities. We have learned how important it is for a government to respond quickly, clearly and consistently to a public health crisis like COVID-19, and to communicate regularly and transparently. We know that politicians are better at responding to crises than preventing them, but by the time a public health crisis has appeared it is, of course, too late to prevent it. A pandemic highlights existing flaws and stress points in fragile health and public health systems, so that putting prevention in place—and funding it adequately—is even more important than responding to a crisis. The contrast of NZ with the delayed, confused or authoritarian responses of the United States, Hungary or Serbia, or the denial of Brazil, could not be starker. We have learned that a light touch with people who do not adhere to isolation and temporary restrictions on movement is more likely to garner public support than a heavy-handed one that violates human rights and social norms.
Border controls were a key tool in NZ’s response to COVID-19. A Māori whakataukī (proverb) says, He whare maihi tū ki roto ki te pā tūwatawata, he tohu nō te rangatira: whare maihi tū ki te wā ki te paenga, he kai nā te ahi. (A carved house standing in a fortified settlement is the mark of a chief; a carved house standing in the open, among the cultivations, is food for the fire.) Just as walls or borders keep danger out, they can also serve to bring people together within those borders. Prime Minister Ardern has repeatedly referred to ‘our team of five million’ (BBC News, 2020a) as a way of bringing the country together to support temporary restriction of movement and other hardships of Levels 3 and 4. Whether that sense of national cohesion and purpose will survive the next steps of recovery and the painful economic realities it will bring remains, of course, to be seen.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author received no financial support for the research, authorship and/or publication of this article.