
Abstract
Globally, 50 million people live with dementia and mostly receive care at home. Urinary, faecal and functional incontinence is common in this population and increases care demands. This study explores care partners’ experiences managing continence care for people with dementia in Aotearoa New Zealand. The data are drawn from a cross-sectional qualitative study with 18 care partners of people with dementia and incontinence in mid and northern regions of Aotearoa New Zealand. Participants were interviewed face-to-face from June 2022 to April 2023. Data were analysed using Interpretive Phenomenological Analysis. Six Generalised Experiential Themes emerged. Care partners engaged in autobiographical and biographical meaning-making to interpret behaviours and maintain the personhood of people with dementia, focusing on dignity, identity, and social inclusion. However, caregiving often undermined care partners’ personhood due to the physical and emotional demands of continence care. Access to resources was challenging, and healthcare support was often perceived as inadequate. Some care partners’ strategies to find meaning and joy in everyday life contributed to resilience, while others experienced stress, fatigue, and burnout. Care partners used personal knowledge to support personhood, especially in social engagement. Uncertainty in managing incontinence led to self-doubt, exacerbated by the medicalised nature of continence care, which involves intimate attention beyond typical caregiving. Timely, credible advice could reduce uncertainty, but many found seeking resources overwhelming. Balancing their own well-being with caregiving highlights the need for support systems addressing the requirements of both care partners and people with dementia.
Keywords
Globally, an estimated 50 million people live with dementia (Prince et al., 2015). A majority of people with dementia live at home, rather than in a long-term care facilities for example, 70–81% in the USA (Brodaty & Donkin, 2009), 61% in the UK (Wittenberg et al., 2019) and 73% in Aotearoa New Zealand (Ma’u et al., 2021). As dementia progresses personal support is often needed for daily activities, such as bathing, dressing, eating, and using the toilet (Ansah et al., 2017).
Dementia and incontinence (the involuntary loss of urine or faecal matter (Abrams et al., 2017)) often occur together. In Aotearoa New Zealand, a recent study of people with dementia who had been assessed for home care services indicated that 50.1% experienced urinary incontinence (UI) (Burholt, Cheung, et al., 2024), and 26.7% experienced faecal incontinence (FI) (Burholt, Pillai, et al., 2024). UI and FI can be linked to neurological issues associated with dementia (Idiaquez & Roman, 2011; Orimo, 2017; Perneczky et al., 2008; Stubendorff et al., 2012). However, as dementia progresses to moderate or severe stages, individuals may experience functional incontinence (e.g., remembering the location of the bathroom), or difficulties interpreting sensations (e.g., recognising the need to void), and making timely decisions to use the toilet. Incontinence significantly affects quality of life and increases care needs (Nguyen & Li, 2020; Shaw & Wagg, 2021; Suhr & Lahmann, 2017). Furthermore, incontinence and dementia are stigmatised conditions that have the potential to elicit negative responses towards ‘devalued stereotypes’ (Clair, 2018; Goffman, 1963).
Most support and care for people with dementia living in the community is provided by unpaid relatives. In 2015, the annual global number of care hours provided to people with dementia living at home was estimated to be around 82 billion hours (Wimo et al., 2018). In this article, we refer to unpaid caregivers as care partners, acknowledging that non-professional support is usually provided in partnership with the person with dementia who plays a role in their own personal care (Bennett et al., 2017). The notion of partnership is central to ‘personhood ‘for people living with dementia.
Personhood in dementia care refers to the recognition and respect for the dignity, identity, and individuality of a person living with dementia, despite cognitive and functional impairments. Personhood can be supported by acknowledging the history, personality, and life experiences of a person, by supporting the person’s ability to make choices, decisions and remain active in self-care and by valuing social connections, relationships and roles within the family and community. Thus, personhood is evoked in interdependent relationships with others (Smebye & Kirkevold, 2013).
Kitwood (1990) used ‘malignant social psychology’ to describe how personhood could be undermined in social interactions that devalue, dehumanise and diminish the person with dementia, for example, when the person is stigmatised, infantilised, objectified or ignored. While malignant social psychology involves practices and attitudes that harm individuals with dementia, ‘positive person work’ (Kitwood, 1997) focuses on affirming personhood, dignity, and autonomy promoting respectful, empathetic, and person-centred care practices. For example, the loss of control associated with incontinence and dementia can impact on self-esteem and elicit feelings of embarrassment, shame and humiliation, undermining personhood (Aldridge et al., 2017; Hayder & Schnepp, 2008; Ostaszkiewicz, 2017), but positive person work involving compassionate, respectful support, focusing on strengths rather than deficits may help maintain dignity of the person with dementia (Smebye & Kirkevold, 2013).
Kitwood’s (1997) original work on personhood focused on social interaction, as ‘a standing or status bestowed upon one human being by others in the context of a relationship’ (p. 8). However, subsequent research has tended to privilege the experiences of the person with dementia (e.g., Patterson et al., 2018). Research with care partners has tended to focus on instrumental, financial and emotional ‘work’ and ‘dedication’, such as the opportunity costs of forgoing employment (Ma’u et al., 2021; Wittenberg et al., 2019) or the rewards, physical and emotional costs (burden or stress) concomitant with supporting a person living with dementia (Liu et al., 2019, 2021; Murray & McDaid, 2020; Nemcikova et al., 2023).
Care partners of people living with dementia and incontinence experience greater burdens than those who do not manage incontinence (Abrams et al., 2017). Promoting continence and managing incontinence often demands constant vigilance which can lead to sleeplessness and exhaustion, compromising the ability to provide effective support in the community (Gibson et al., 2022; Gibson & Gander, 2021). Despite this, only a small body of research focuses on the experiences of care partners of people living with both dementia and incontinence (Murphy et al., 2021; for a critical review see, Burholt et al., 2020). The gap in knowledge is important because rates of moving into aged residential care are much greater for people with dementia than for older people without dementia, and incontinence is consistently identified as a predictor for institutionalisation in this population (Cole et al., 2022; Luppa et al., 2010). This suggests that we need to know more about care partners’ experiences to develop appropriate resources or services.
The aim of this article is to investigate the experiences of promoting continence and managing incontinence from the perspective of care partners of people with dementia living in the community in Aotearoa New Zealand. We use interpretive phenomenological analysis (IPA) (Smith & Nizza, 2022) to describe and understand how care partners make sense of their situation.
Methods
Data are from a sub-study in a programme of research that identified the prevalence, incidence and risks of urinary incontinence and faecal incontinence for people with dementia living in the community (Burholt, Cheung, et al., 2024; Burholt, Pillai, et al., 2024), examined the current practices of health professionals, people with dementia and their care partners; and co-created resources intended to improve outcomes for people with dementia and their care partners (Burholt et al., 2023).
Sample and setting
A convenience sample of care partners (N = 18) supporting people with dementia. The inclusion criteria for people with dementia (not included in the article) were self-reported dementia, capacity to provide informed consent, aged ≥65 years, experiencing difficulties getting to and using the toilet or incontinence, living in Northland, Waikato, Bay of Plenty and Auckland regions (Supplementary File 1) and able to speak and understand English. The inclusion criteria for care partners, were aged ≥18 years and providing care to a person living with dementia who met the inclusion criteria and was taking part in the study.
Participants were self-selected volunteers who contacted the research team in response to advertisements and through collaborating community group networks across the mid and northernmost regions of North Island, Aotearoa New Zealand. Study information (a participant information form for the person for dementia and one for the care partner) was sent by post or email. The research team followed-up after two weeks and scheduled interviews for those interested.
Design
A cross-sectional qualitative study design was used. People living with dementia were asked whether they wished to be interviewed alone or with their care partner. Two people with dementia and their care partners were interviewed separately (i.e., there was not a joint interview). Sixteen care partners were interviewed with the person with dementia. These care partners were offered a separate individual interview: three chose this option in addition to a joint interview. Care partners took part in face-to-face guided interviews and completed a short demographic survey between June 2022 and April 2023.
All three versions of the interview schedules (individual care partner, joint interviews, additional care partner interview) included sections on toilet use, nocturia (the need to wake one or more times during the night to urinate, with each void preceded and followed by sleep), UI and FI. Each section examined the nature of challenges, the perceived effectiveness of strategies employed (e.g., routines, continence products, dietary and medication interventions, and alternative therapies), experiences with health professionals, and the impact on daily life. Care partners completed a survey that included questions on age, gender, marital status, ethnicity, relationship to care partner, and length of time providing support to the person with dementia. The semi-structured interview schedules and survey are published elsewhere (Burholt et al., 2023).
Interviews were conducted by three experienced research fellows with backgrounds in nursing, social gerontology and occupational therapy. Interviews were recorded and transcribed by a professional transcriber who had signed a confidentiality agreement.
Analysis
The data coding procedure and process followed the seven steps of IPA (Figure 1) (Smith & Nizza, 2022). Steps 1–5: YO thoroughly reviewed the full transcripts until completely immersed in the data. Notes were diligently taken, highlighting relevant units of meaning and emerging themes of significance. Themes were identified based on their relevance to the research question. Subsequently, transcripts were coded to reflect these themes, generating a preliminary list. The transcripts underwent multiple re-readings to ensure the list was exhaustive and relevant extracts were compiled for each theme. All data were coded manually. A second researcher (VB) validated the analysis, interpretation, and definitions of Personal Experiential Themes (PET). The seven-steps of Interpretive Phenomenological Analysis.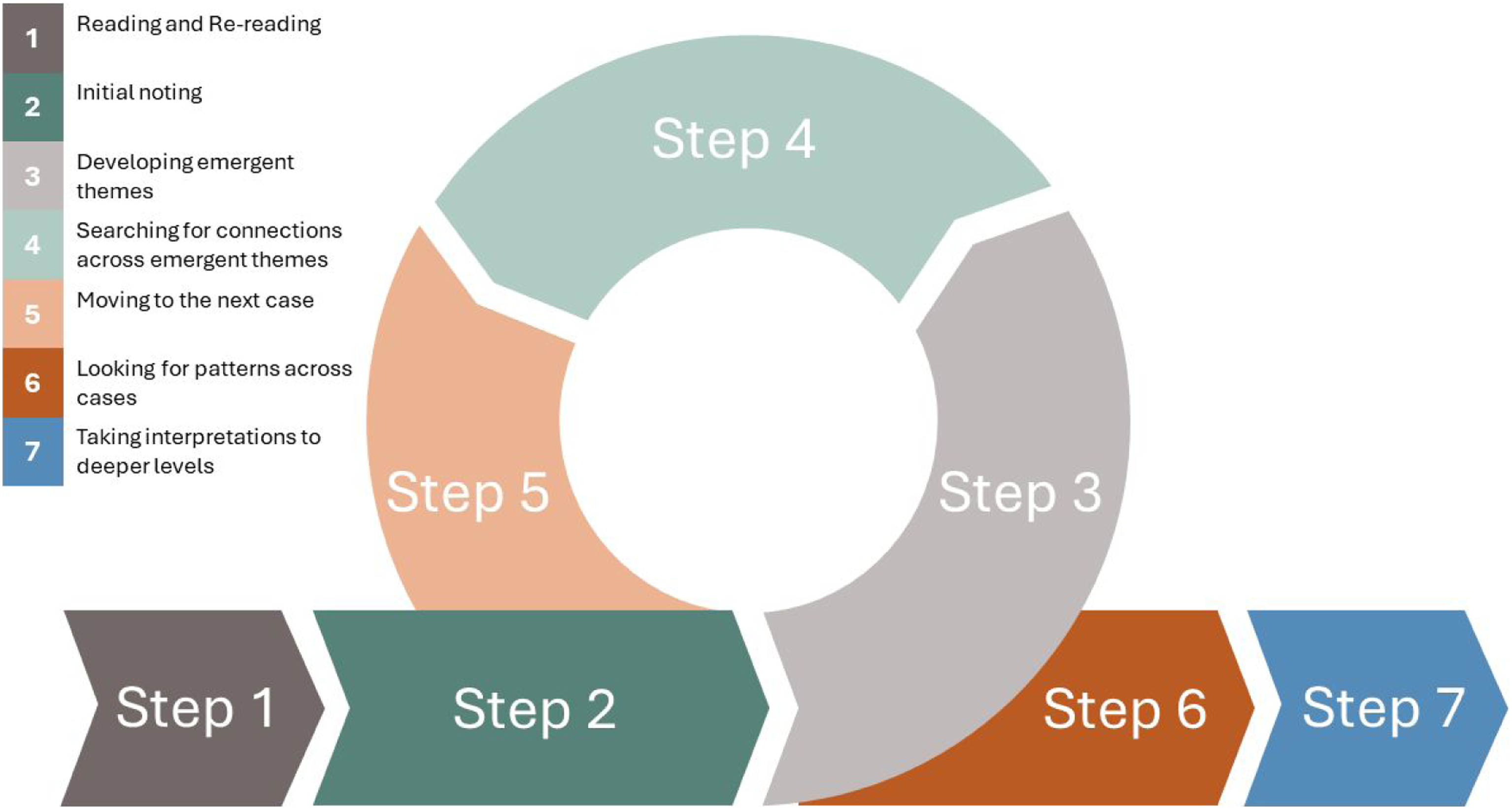
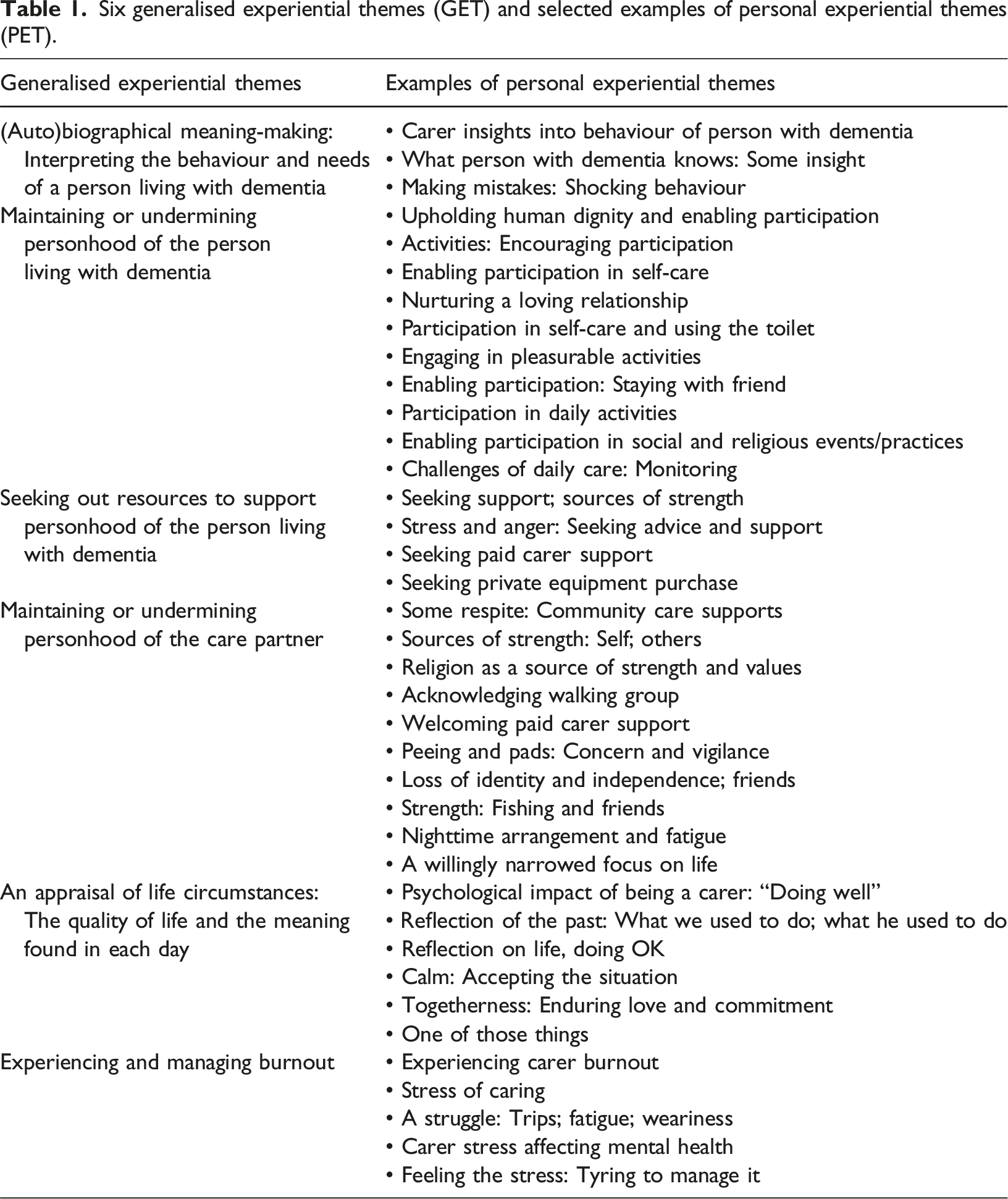
Six generalised experiential themes (GET) and selected examples of personal experiential themes (PET).
Ethical approval
Ethics approval for Phase 3 was obtained from Southern Health and Disability Ethics Committee (reference 11658) on the 28 April 2022.
Indigenous (Māori) engagement
Māori (the indigenous population of Aotearoa New Zealand) have been involved in the conception of the research, design of the methods, data collection and analysis. The research proposal was co-designed with Advisor Māori Research Fellow Tess Moeke-Maxwell (Ngāti Tai (Hauraki); Ngāti Porou). Māori Research Fellow and co-author SA (Ngāti Porou; Ngāti Kahungunu), led the Māori arm of the study in Hawkes Bay region with Māori research assistants Roni Nuku (Ngāti Maniapoto) and Arapera Riki (kuia – female Māori elder). Māori interviews were informed by culturally safe research processes. Recruitment and interviews were informed by a pōwhiri model of engagement. This process upheld rangatiratanga (the right of Māori people to rule themselves; self-determination), whakapapa (genealogical or ancestral lineages; interconnections between Māori), mana (status), tikanga (cultural practices) of Māori based on the principles of whanaungatanga (relationship building) and manaakitanga (nurturing, care and hospitality). A Kāhui Kaumātua (advisory group) guided interpretations of Māori data analysis. The analysis reported in this paper does not include the Māori data collected in the Hawkes Bay region as analysis and interpretation of these data are conducted by the researchers named above, using methodologies and perspectives rooted in Te Ao Māori (Māori worldview).
Informed consent
Written informed consent was obtained for each participant. Participants (both people with dementia and their care partners) provided written informed consent on the day of the interview, prior to the interview commencing. Judgments concerning capacity to provide informed consent were made by trained researchers. The researchers asked participants to describe in their own words what the study was about, and what they were being asked to do.
Findings
Of the 18 care partners, four (22.2%) were male and fourteen (77.8%) were female. The sample comprised 13 (72.2%) spouses, three (16.7%) daughters, one sister (5.6%) and one niece (5.6%) of the person with dementia. The mean age of care partners was 63.83 years (SD 21.51). Six (33.3%) participants had provided support for fewer than 12 months, four (22.2%) for 1–2 years, and eight (44.4%) for more than 2 years.
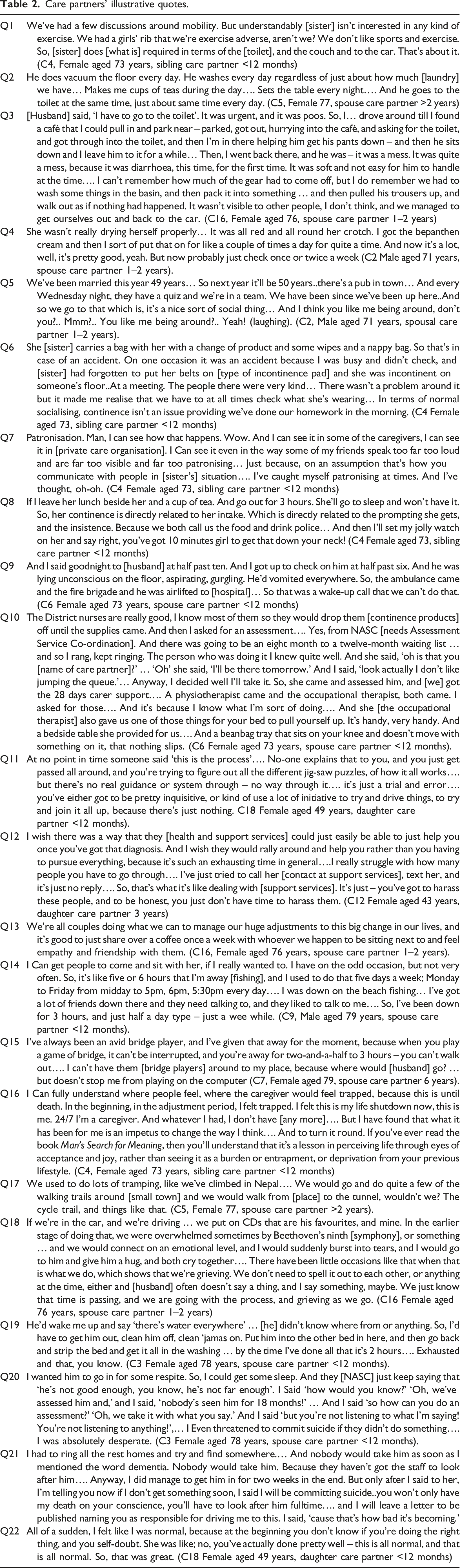
Care partners’ illustrative quotes.
(Auto) biographical meaning making: Interpreting the behaviour and needs of a person living with dementia
Care partners used autobiographical and biographical meaning making to interpret the behaviour and needs of a person living with dementia. Biographical meaning making refers to the care partners’ accumulated understanding of the biography and life course of the person with dementia (i.e. interpretations, assumptions and perceptions about what they are known for, who they know, how they present themselves: their identities, likes and dislikes), For example, one care partner associated her aunt’s cognitive health status with her lifelong religious beliefs and practices and said, “if [aunt] did not have her religious beliefs [Mormon], I believe her cognitive health would have declined faster… because it’s set routines, she reads her scriptures, does certain things.”
Autobiographical meaning making refers to the interpretations of the memories of the overlapping times, places and experiences of the person with dementia and the care partner. It also includes recent knowledge and understanding of behaviours relating to incontinence. For example, one participant discussed her sister’s mobility by providing a history of both siblings’ dislike of exercise (Q1, Table 2). Another participant disclosed some insights into her husband’s love of routine, interpreting his customary habits as contributing to his worry about having an accidental bowel motion while out (Q2 Table 2). Addressing her husband she said, “I think that could be at the back of your mind, do you? Because you think about [an accidental bowel motion] quite a lot like when we’re going out.”
Despite significant autobiographical overlap, some care partners, who knew the person with dementia well, found themselves unable to explain their actions. For example, one spouse revealed that his wife ‘makes mistakes’ that he did not understand, “a few times, she comes around to my side [of the bed] and I say, ‘what’s happening?’ She strips off and does wees. So, I don’t know why that happens” (C13, Male aged 85 years, spouse care partner 3 years). He was confused and worried by his wife’s behaviour and explained it as “something in her mind.” However, he still could not quite fathom it, because he noted “the toilet’s right there.”
Understanding the biography of a person with dementia, or having a shared autobiography contributed to meaning making and interpreting the situation for some care partners, but for others this made understanding more challenging.
Maintaining or undermining personhood for the person living with dementia
Care partners used (auto)biographical meaning making and interpretations to help sustain the personhood of the person with dementia: upholding personal worth, dignity, and identity, fostering social inclusion, empowerment and agency, and keeping them safe and healthy.
One spouse described cleaning up after faecal incontinence in a public place to retain the dignity of her husband (Q3 Table 2). Concerned to keep toilet practices as normal as possible and retain her husband’s personal worth, she added, “he’s still in his ordinary undies… and that pad inside like that. I hope that gives him some dignity.”
Care partners recounted ways in which they fostered social inclusion, empowerment and agency by understanding the preferences of the person with dementia. For example, one spouse drew on her autobiographic knowledge to engage her husband, sharing, “he loves Andre Rieu; we’ve been to quite a few of the concerts. And I’ll just put it there on the iPad and he’ll watch it” (C1, Female Spouse, 77 years, caring 5 years). While confident in selecting appropriate recreational activities for her husband, she experienced uncertainty about providing functional support to maintain independence and agency. She described her husband’s limits to self-care and said, “he can find the toilet, the ensuite… I say, I’d just like you to go and have a try… And just, you know, sit there for a while and he’ll do that but for wees.” However, she was unsure if she should also similarly prompt him to defecate
Other care partners made efforts to retain personhood by keeping the person with dementia safe and healthy. In promoting continence and managing incontinence, this often involved checking on hygiene and skin integrity. One care partner explained that his wife encountered difficulty wiping herself after defecating, so he monitored and assisted her during and after showering (Q4 Table 2).
Care partners also supported personhood, through emotional and affective support. For spousal care partners, this often involved nurturing a loving relationship. For example, one spouse care partner tried to maintain a sense of happiness for his wife by continuing to participate in a weekly pub quiz with her (Q5 Table 2).
Some care partners proactively organised opportunities for socialising despite the challenges that could arise due to incontinence. One spouse organised overnight visits with friends, he said “we’re probably going up tomorrow morning and stay the night, but we’ll take all our bedding – our sheets and that with us, and just use our blankets and that. So, I’m sure that will be alright” (C13, Male aged 85 years, spouse care partner 3 years). Similarly, a sibling had identified local social groups for her sister to attend but commented on the challenges and preparation associated with outings. She recalled an occasion when being too distracted to check on her sister’s preparedness, resulted in urinary leakage while out (Q6 Table 2).
Some care partners expressed ambivalence towards personhood, displaying both supportive and undermining behaviours. While Q6 was presented as evidence of supporting personhood by facilitating opportunities for social engagement, the use of terms such as “nappy bag” infantilised the person with dementia. This care partner acknowledged occasional patronising behaviour and tried to adjust her communication (Q7 Table 2).
Several accounts focused on the instrumentality of care work such as changing pads, dealing with hygiene and skin integrity. This approach may unintentionally objectify the person with dementia and incontinence, as in need of ‘treatment’ and diminish their sense of personhood. Good nutrition and hydration are important for physical health, mental health and wellbeing. However, some people with dementia may not recognise satiety or hunger (Amella, 2004). One participant’s narrative demonstrated the fine line between ensuring sufficient intake and bullying or threatening behaviours to achieve this (Q8 Table 2).
Providing continence care and support to a person with dementia often required constant vigilance; a lapse in attentiveness could undermine personhood of the person with dementia (e.g. loss of dignity, poor skin health), or lead to greater demands on the care partner (e.g. assisting with additional showers, or more laundry). For example, one care partner managed to get a good night’s sleep by sleeping apart once a week, but this compromised her husband’s safety, leading to a fall and hospitalization (Q9 Table 2).
Care partners play a crucial role in either maintaining or undermining the personhood of individuals living with dementia. Through (auto)biographical meaning-making, many care partners strive to uphold personhood, but the demands of caregiving, especially continence care, can lead to moments where personhood is inadvertently diminished.
Seeking out resources to support personhood of the person living with dementia
Some care partners, unable to provide support alone, sought out additional resources and expressed gratitude for support from religion or faith, friends, and formal continence support services. For example, one participant who was a retired nurse used her knowledge and contacts to obtain the support she needed for her husband, emphasising the need to be proactive. She explained how she secured a needs assessment for her husband, regular delivery of continence products, and home equipment that made life easier for both (Q11 Table 2).
Others care partners also proactively sought out resources or information that could help them promote continence or manage incontinence, but without ‘insider’ knowledge of the health system, many struggled to obtain the help that they needed. This was exacerbated in ‘lockdown’ during the COVID19 pandemic when services were often restricted to existing clients (Burholt, Wiles, & Schneller, 2024). For example, an employed care partner living separately from her mother with dementia, struggled to organise support, finding the phone-based care planning process frustrating. (Q11 Table 2). Even after reaching assessment coordinators, she faced further frustration and disappointment as new referrals were not being accepted. She summarised her experience by stating, “the system is broken.”
Some care partners were exasperated by how much effort they had to put in to obtain information or support for promoting continence or managing incontinence of the person with dementia. For example, another daughter care partner who lived separately from her mother with dementia was critical of access to, and the coordination of health and support services. She felt that the GP did not listen to her concerns and that support services neglected her so that she was “left floating around until something goes wrong” (Q12 Table 2). Searching for information put her under considerable stress as she explained, “you have to be quite active in trying to find anything, and then it’s like, you’re pretty tired, and you’re just trying to live life and get through the day…. It’s fucking exhausting.”
Seeking out resources or information to support the personhood of people living with dementia is often a challenging and exhausting process for care partners. While some successfully navigated the system by leveraging their knowledge and connections, many others struggled without such “insider” advantages. The COVID-19 pandemic further complicated access to essential services. However, even outside of lockdown, care partners were still frustrated by the lack of clear guidance and support.
Maintaining or undermining personhood of the care partner
Activities and services were important in maintaining (or undermining) identity, and individuality, valued social connections, relationships and roles within the family and community for care partners. Despite considerable frustrations with access to health and support resources, some services were used to support the personhood of the care partner as well as the person living with dementia.
Strategies were adopted to alleviate some of the negative outcomes of providing support to a person with dementia that could undermine the personhood of the care partner. For example, nocturnal behaviour or activities (such as nocturia) can undermine the sleep health of care partners. One care partner chose to sleep in a separate bed from her husband because he tended to encroach on her side. She interpreted his behaviour as a desire to be close to her, noting, “It’s as if he’s trying to get closer and closer to me, and he ends up with his head on my pillow. When I try to move him, he just gets closer” (C7 Female aged 79 years, spouse care partner 6 years). Sleeping in separate beds has proven to be beneficial for them both.
Respite (a rest) from caring allowed care partners to have some time to themselves to pursue hobbies or friendships, to have a break, rest or sleep. One spouse care partner noted “I’ve got a lady comes in – on a Thursday … about 2–4…. Yeah, so that’s a help; she takes [wife] away to have a coffee” (C13 Male aged 85, spouse care partner 3 years). Others sought support from peers. One participant noted that a weekly walking group hosted by a local dementia organization provided the opportunity to share her experiences and had become a major source of support (Q13 Table 2).
For other care partners, the constant vigilance required of them undermined aspects of their own personhood. For example, one spouse revealed that she no longer went out alone and always took her husband with her. Although she was a manager of a local charity shop she had to mostly work from home and said “I miss going down to work” (C3 Female aged 73 years, spouse care partner <12 months). She was both angry, and sad that friends had stopped visiting and keeping in contact and lamented, “How many friends? You don’t see them, you don’t hear from them..I don’t think they know how to cope with it [dementia].” Similarly, other care partners had given up recreational activities, hobbies or passions. For example, one care partner had significantly reduced fishing (Q14 Table 2). On the other hand, despite being unable to join her friends to play bridge another participant adopted a ‘virtual’ strategy that enabled her to continue to get pleasure from the game (Q15 Table 2).
The efforts care partners make to maintain their own personhood amid the demands of caregiving are both complex and vital. While challenges such as restricted access to resources and the constant vigilance required in caregiving can undermine their identity and social connections, many care partners find ways to support their own well-being. By seeking respite, engaging in supportive communities, and finding personal fulfilment through hobbies and social activities, care partners alleviated some negative impacts of their role.
An appraisal of life circumstances: The quality of life and the meaning found in each day
Care partners assessed their life circumstances, finding meaning and maintaining quality of life despite the challenges of caregiving. As they confronted the emotional and physical demands of supporting a person with dementia, they employed various strategies to stay resilient and to put a positive spin on life.
Some care partners drew on spirituality or religion. For example, one participant who was supporting her sister with dementia and her husband (a stroke survivor) talked about how she altered the feeling of ‘entrapment’ in her role, to one of joy and acceptance through applying philosophical (existential suffering), psychological (logotherapy, where meaning is a central motivating form in human life) and spiritual principles (e.g. human soul’s resilience, and the search for a higher purpose), that were elucidated upon in a book that she read (Q16 Table 2).
Other care partners reflected on the past with the person with dementia and found comfort in recalling joyful experiences that they shared. For example, one participant reflected on the walking trips her and her husband had undertaken. Although there was an air of disappointment that they were now unable to walk together, there was also fondness for the memories (Q17 Table 2).
Similarly, other care partners found comfort in activities that activated a sense of enduring love and commitment. The joy found in everyday activities was a counterpoint to sadness and anticipatory grief. Anticipatory grief is associated with a series of cumulative losses throughout the dementia journey, such as a decline in intimacy and companionship, the erosion of personal freedom, reduced social or occupational opportunities, and shifts in role identity (Cheung et al., 2018). For example, one care partner talked about seeking out fun in everyday activities with her husband, noting “we have as much fun as we can with the day, and laugh when we can.”. Despite her husband’s dementia, she explained that their most powerful connection was emotion. In this respect, music provided an outlet to relieve their sadness and anticipatory grief, but also provided a sense of intimate connection (Q18 Table 2).
Whether through spirituality or cherishing shared memories, some care partners found ways to sustain a positive outlook and good quality of life. These approaches not only helped them cope with the ongoing losses associated with dementia, but also allowed them to sustain a deep emotional connection with their loved ones.
Experiencing and managing burnout
The unrelenting demands of providing continence care for a person with dementia impacted on several care partners’ own sense of identity, ability to maintain friendships or paid work. Some care partners found ways to mitigate challenges thus avoiding burnout, while for others the persisting challenges resulted in anxiety, stress, fatigue, or sleeplessness.
Challenges that contributed to carer anxiety and stress included coping with continence products that did not meet the needs of the person with dementia and navigating the health system to obtain support. This was illustrated by one participant who expressed frustration and annoyance over the inadequacy of the pull-ups her husband used, which often leaked and soiled the bed. She was particularly irritated by her inability to resolve the issue and questioned herself, saying, “What am I doing wrong? Because sometimes I’m fine, and sometimes I’m not” (C1, Female aged 77 years, spouse care partner 5 years). She referred to the continence products as “the bane of my life.” The stress of managing soiled products led to feelings of guilt and anxiety, as she blamed herself when her husband defecated in his pull-ups, saying, “cos I should take him [to the toilet] more often.” However, to mitigate the risk of burnout, she allocated her respite care allowance to facilitate a two-week visit from her family in Australia, providing her with much-needed respite.
Care partner fatigue was associated with disturbed sleep attributed to leaking products that required a change of bed sheet, or nocturia. The former was illustrated by a care partner who experienced interrupted sleep from having to get up at night to change wet bed sheets (Q19 Table 2). The exhaustion resulting from her nocturnal activity, was compounded by an inability to get support. Out of desperation to receive an assessment of her husband and respite care, in her own words she resorted to “threatening suicide” (Q20 Table 2). This prompted an assessment, but her husband was deemed eligible for residential care, not dementia care. Despite her stress and exhaustion, the participant exhibited a strong, courageous, problem-solving approach and lodged a complaint. Although her husband’s eligibility for respite care was revised, this in turn, contributed to increased anxiety and a further “threat” of suicide as she sought an appropriate respite placement for him (Q21 Table 2).
Feelings of abandonment by health and support services heightened stress and contributed to depression for several care partners seeking support. For example, one participant, dissatisfied with the help she received for her mother and struggling with her own declining mental health, was prescribed anti-depressants instead of receiving the needed services. Uncomfortable with taking the medication, she reached out to a local dementia organization (Q22 Table 2). While the charity offered reassurance and hope, it did not resolve the long-term issue of securing adequate health and social support for her mother, preventing her from returning to work.
Providing continence care to a person with dementia can contribute to burnout among care partners. The struggle to balance the role of care partner with personal needs often resulted in severe emotional distress. Challenges accessing health and support services compounded these issues.
Discussion
Care partners used (auto)biographical meaning making and interpretations to help sustain the personhood of the person with dementia (Hennelly et al., 2018). While this was commonly applied in relation to providing opportunities for meaningful recreational activities or social engagement, there were examples of “care partner uncertainty” in continence care (Sodowsky, 2012).
Care partner uncertainty captures the self-doubt and hesitation that caregivers may experience when they are unsure if they are providing the correct care or making the right decisions, such as when assisting a person with dementia in intimate tasks like using the toilet. Incremental change in UI, FI or functional incontinence often requires decision-making by the care partner in how this challenge will be tackled to support personhood. In this study, some care partners’ decision-making was based on the (auto)biographical knowledge of the preferences of the person with dementia, but because continence care carried medicalised connotations, involving a level of intimate attention that goes beyond typical caregiver practices, it also precipitated self-doubt for others.
Care provided at home is linked to personal histories and meaning making, and most care partners’ continence care practices were motivated by a desire to do their ‘best’ to support personhood. There was evidence of care partners attempting to draw on autobiographical experience to make sense of some of the unusual behaviours of the person living with dementia, such as urination or defecation in inappropriate places. This suggests a limited understanding of dementia.
Care partners are often key decision makers and their knowledge of dementia has health implications for the person living with dementia as well as their own psychological wellbeing (Cahill et al., 2015). Elsewhere, it has been noted that care partners require knowledge about the association between dementia and incontinence (Bliss et al., 2013). Practices undermining personhood may arise from inadequate understanding or education concerning dementia and continence care, as well as deficiencies in health professional assistance or respite for care partners.
It is likely that the provision of timely, appropriate advice and information about dementia and incontinence by credible and trustworthy health professionals (Sodowsky, 2012) could contribute to reducing care partner uncertainty and improving health literacy, thus impacting indirectly on supporting personhood for the person with dementia. However, the care partners’ experiences of seeking out resources or information to support the personhood of the person living with dementia were problematic requiring a proactive approach that was exhausting and for some overwhelming. The onerous nature and need for a proactive approach to seeking out information has also been identified as a challenge for care partners of people with dementia in the United Kingdom (Hargreaves et al., 2023).
Personhood for people with dementia is relationally constructed (Kitwood, 1997), and we argue that relationship-centred continence care needs to address the lived experience of care partners alongside that of the person with dementia. While positive person work by care partners focuses on preserving the personhood of the person with dementia, vigilant continence care can impact on their own health and wellbeing. The findings show paradoxically, promoting personhood for people with dementia and continence challenges can simultaneously undermine the personhood of care partners.
Care partners’ ongoing appraisals of negative and positive aspects of life were fundamental to future intentions to continue to provide care. Balancing the negative and positive aspects of their experience contributed to the maintenance of well-being. Care partners employed various strategies to find meaning and joy in their daily lives, such as adapting ways to participate in hobbies and recreational activities, drawing on religion or spirituality, and cherishing shared memories. These methods not only helped them cope with the ongoing challenges but also allowed them to maintain a deep emotional connection with their loved ones, even as they navigated the complex journey of dementia. However, when negative experiences outweighed the positive, care partners faced burnout: physical, emotional and mental exhaustion. The sacrifices and adjustments that care partners made, such as leaving employment, curtailing personal interests or experiencing social isolation, highlight the ongoing need for balanced support systems that address both their needs and those of the individuals they support.
We acknowledge limitations to this study. First, we have drawn on a small sample of care partners comprising mainly white New Zealanders of European descent. Separate arms of this study have collected data from the Indigenous Māori and Pacific Island populations, with analysis and interpretation being conducted by researchers from these communities, using methodologies and perspectives rooted in their respective worldviews. However, this may not fully represent the diversity of experience among all care partners of people living with dement and incontinence in New Zealand, especially those from different ethnic or cultural backgrounds. Second, the study employed interpretive phenomenological analysis (IPA), which, while providing deep insights into personal experiences, is inherently subjective (a double hermeneutic) and may reflect the researchers’ interpretations as much as the participants’ lived experiences. Third, the study was conducted in a specific political, cultural and geographical context, which may influence the findings. The challenges related to incontinence in dementia care might vary significantly in different healthcare systems or cultural settings, limiting the applicability of these findings outside of New Zealand.
Despite these limitations, the study highlights the significant challenges faced by care partners in managing continence care for people living with dementia. This is consistent with evidence from a critical review that suggests continence guidelines often overlook the specific needs of individuals with dementia, particularly in community settings. The review highlights that, internationally, guidance on assessment and care planning for this population is often fragmented and inconsistent (Burholt et al., 2020). Moreover, a systematic review of studies describing the experience of care partners of people with dementia (even when not specifically focused on incontinence) reveals that some themes and challenges identified in our study resonate with care partners globally (Cross et al., 2018). This suggests that the struggles faced by care partners in Aotearoa New Zealand are not unique and may be reflective of broader, international trends. The difficulties in balancing caregiving with personal needs, along with challenges in accessing adequate services and information, often lead to emotional distress and burnout. These findings highlight the urgent need for accessible and coordinated support systems that genuinely address the needs of care partners, helping them to sustain their mental health and resilience while maintaining the dignity and well-being of people living with dementia while providing continence care and support.
Conclusion
While personhood is primarily associated with the rights and dignity of people with dementia, it can also be applied to draw attention to the rights and needs of care partners. Promoting continence and managing incontinence whilst maintaining personhood requires someone to provide support for the person with dementia to enable them “to be who they are, which relates to their past, present, and future achievements, activities, preferences, goals, relationships, and potential for well-being” (Tieu & Matthews, 2023). Although the intimate (auto)biographical knowledge of the person with dementia proved advantageous in devising strategies to attain this goal, care partners who undertook continence care found themselves needing to renegotiate aspects of their own lives. This renegotiation affected their capacity to simultaneously pursue the same objectives as those they are striving to maintain for the person with dementia. This paradoxical life situation suggests that continence care and assessment practices should extend beyond bladder and bowel assessments and strategies for the person with dementia, to explicitly acknowledge care partners as individuals with needs, wishes, and roles, which extend beyond the caring role.
Supplemental Material
Supplemental Material - A ‘personhood paradox’: Care partners’ experiences supporting people with dementia and incontinence
Supplemental Material for A ‘personhood paradox’: Care partners’ experiences supporting people with dementia and incontinence by Vanessa Burholt, Yasmin Orton, Sharon A Awatere, Julie F Daltrey in Dementia
Footnotes
Acknowledgements
We acknowledge the other investigators on the study: Avinesh Pillai, Kathryn Peri, Rosie Gibson, Ngaire Kerse, Gary Cheung, Anna Lawrence, Deborah Balmer.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Health Research Council of New Zealand [Grant number 21/117]. The sponsor had no role in the conceptualization, writing, or publication of this work.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.