
Abstract
Child sexual abuse is associated with a range of negative consequences, including behavior problems and dissociative and posttraumatic stress symptoms. Trauma-Focused Cognitive Behavioral Therapy (TF-CBT) has shown to be successful in the treatment of child victims of sexual abuse, but yet presents some challenges with preschoolers. Child sexual abuse has often been associated with insecure attachment among preschool children. Therefore, combining an attachment-based intervention with the TF-CBT may offer a means to optimize therapeutic outcomes. This pilot study examined in a pre/post-test design whether the combination of the Attachment Video-feedback Intervention (AVI) with the TF-CBT led to changes in the well-being of sexually abused preschoolers and their parents. Participants included 33 sexually abused children aged 4 to 6 years old and their non-offending caregivers. Parents completed questionnaires on their child’s behavior problems and dissociative symptoms, and reported on their own psychological distress and posttraumatic symptoms following their child’s disclosure of trauma. Results showed decreases in child internalizing and dissociative symptoms and maternal psychological distress and posttraumatic symptoms after the intervention. This pilot study suggests this combined protocol is a promising tool to foster the recovery of young victims of sexual abuse and their non-offending caregivers.
Child sexual abuse (SA) is a devastating yet prevalent, world-wide problem. According to a meta-analysis, it is estimated that 1 woman out of 5 and 1 man out of 10 report having experienced child SA before the age of 18 (Stoltenborgh et al., 2011). Research has shown that children victims of SA display higher levels of internalizing and externalizing behavior problems, as well as symptoms of posttraumatic stress disorder and dissociation (Hébert et al., 2016; Lewis et al., 2016).
Although not studied as extensively as in school-aged children, a recent review of the consequences of SA in preschoolers (Tejada & Linder, 2018) indicates that they show higher levels of externalizing and internalizing behavior problems than their non-abused peers. As well, research has shown that preschool victims of SA show greater sleep problems over a 1-year-period than their non-abused peers (Langevin et al., 2017) and that these negative outcomes are associated with dissociative symptoms (Hébert et al., 2017). Furthermore, compared to non-abused children, child victims of SA have more emotion regulation problems and higher levels of emotional lability. These deficits appear more pronounced in boys than in girls, even 1-year following the disclosure of abuse (Langevin et al., 2016; Séguin-Lemire et al., 2017). Sexually abused children also are more likely to display insecure attachment representations (Charest et al., 2018).
Child sexual abuse and attachment representations
Caregivers who are responsive and sensitive to their child’s needs are known to promote the development of a secure internal working model of attachment in their children (Bretherton & Munholland, 2008). Internal working models of attachment are cognitive schemas that include representations of the self, others, and attachment relationships. They guide the way children interpret and behave with others in relationships. Such models are also believed to be good indicators of the caregiving quality children are exposed to (Miljkovitch et al., 2012). Recent studies have shown that children with a maltreatment history are at greater risk of disorganized attachment behaviors in comparison to children of the general population (Cyr et al., 2010). As well, in a sample of preschoolers, attachment representations of SA children were more insecure relative to a comparison group of non-abused peers (Charest et al., 2018). The authors hypothesized that child victims of SA could be exposed to more insensitive caregiving than non-abused children after disclosure and perhaps even before disclosure.
Charest et al. (2019) also found higher scores of attachment disorganization to mediate the relation between SA and internalizing or externalizing problems in preschool-aged victims of SA (Charest et al., 2019). Furthermore, SA children with disorganized attachment were 6 times more likely to show behavior problems reaching clinical levels than victims of SA with a secure attachment (Beaudoin et al., 2013). In addition to showing greater internalizing and externalizing problems, Ensink et al. (2020) reported higher levels of dissociative symptoms in SA children in comparison to children with no history of SA. Ensink and colleagues (2020) also reported that SA children were more likely to show insecure or disorganized attachments than children with no history of SA. These findings led the authors to conclude that interventions intended for SA children should focus on improving posttraumatic symptoms and aim to enhance the quality of the caregiving and attachment relationship. Thus far, Trauma-Focused cognitive-behavioral therapy (TF-CBT) has been the privileged approach in the treatment of child difficulties following SA. However, this strategy does not specifically address the caregiving patterns of the non-offending parent.
Trauma-focused cognitive behavioral therapy (TF-CBT)
The TF-CBT approach (Cohen et al., 2006, 2017) is a widely used therapy in the treatment of psychological problems associated with traumatic events. TF-CBT aims to decrease posttraumatic stress symptoms in victims and enhance their skills to address the trauma. TF-CBT is a structured, short-term intervention varying in length on average from 12 to 16 sessions. The structured frame of the TF-CBT and its’ theoretically driven protocol are key components in alleviating children’s posttraumatic stress symptoms. During TF-CBT, children gradually learn to acquire emotional regulation competencies and effective coping strategies to address the traumatic event. During sessions, the therapist targets cognitive and behavioral aspects of the trauma and uses techniques such as cognitive restructuring, self-protection skills, and relaxation to help generate a more accurate and less threatening narrative about the trauma. Given that this approach is flexible regarding the sequence of the treatment components, its framework can be adjusted according to the child’s progression and cognitive abilities (Cohen et al., 2017).
A unique feature of TF-CBT is that non-offending caregivers are involved in the therapeutic process. With the help of the therapist, children and non-offending parents address various aspects of the trauma, and tools are provided throughout the intervention to reduce the child’s traumatic symptoms. Furthermore, the caregivers learn to adopt adequate support strategies toward children (Hébert & Daignault, 2014), which help maintain therapeutic gains outside therapy. Because parents are a primary source of affection and support in their children’s recovery (Cohen et al., 2006), their presence in the intervention is of great value for children’s overcoming the trauma.
The effectiveness of the TF-CBT is largely supported by many studies (Hébert & Amédée, 2020; Jensen et al., 2014; Konanur et al., 2015; Slade & Warne, 2016 for a meta-analysis). In general, studies revealed that TF-CBT leads to decreases in posttraumatic symptoms and behavior problems for school-aged children. Moreover, results have shown that TF-CBT reduces depressive symptoms and distress in parents of SA children (Cohen et al., 2006). Overall, studies have shown the value of the TF-CBT intervention in the treatment of SA children.
TF-CBT results and challenges with preschoolers
Although TF-CBT has proven beneficial to decrease symptoms associated with SA in school-aged children and their parents, it has raised challenges when used with preschool children. In a previous study we found significant decreases in dissociative, internalizing, and externalizing symptoms for SA preschoolers, and such effects were maintained 6 months after the end of the intervention (Hébert & Daignault, 2014). However, challenges were brought-up by the clinicians with regards to the children’s younger age. One issue is that SA preschoolers are at a different cognitive developmental stage than school-age children and that their levels of awareness and understanding of the trauma vary greatly from one child to another. In our previous study, we suggested that younger children’s level of cognitive maturity is intricately related to what they can learn throughout the sessions, and thus TF-CBT should be calibrated to the children’s cognitive abilities (Hébert & Daignault, 2014). Another issue concerned the parent-child relationship and the extent to which TF-CBT may address the attachment relationship as a fundamental pillar in children’s developing sense of security. Cohen et al. (2006) have mentioned that one of the most salient emotional consequences of SA in children is the fear and the feeling of betrayal they have of the world in general and of their parent, given that they were left unprotected by them. Thus, it is crucial to work with non-offending parents to support the child to parent attachment relationship. Throughout infancy and childhood, sensitive parents, with “good enough” parenting skills, are havens of safety to which children seek proximity in times of distress and security bases from which they learn to explore both their physical environment and emotional world (Cyr et al., 2014). During TF-CBT sessions, parents can be more supportive and learn to improve their communication skills toward the child (Cohen et al., 2006). Nonetheless, despite this relational component, the TF-CBT does not specifically address the parent-child attachment relationship as a means to alleviate children’s trauma symptoms.
To optimize the therapeutic effects of the TF-CBT for SA preschool-age children, it would be much suited to combine it with an attachment-based intervention strategy. In the past years, a few short-term, attachment-based intervention protocols were developed for at-risk, abusive, or neglecting parents and their children (Bernard et al., 2012; Moss et al., 2011). In particular, the Attachment Video-feedback Intervention (AVI), by Moss and colleagues, which was delivered to 0 to 6 years old children, included a small portion of SA children. The AVI was designed to improve parental sensitivity and child attachment security through positive video feedback with the parent. Based on randomized control trials, the AVI showed increases in parental sensitivity in maltreating parents, attachment security, and mental and motor development in their children, and decreases in child attachment disorganization and behavior problems (Cyr et al., 2020; Dubois-Comtois et al., 2017; Moss et al., 2011). To our knowledge, a protocol combining the AVI with the TF-CBT has never been tested with SA preschoolers and their non-offending parents.
The current study
The Child Advocacy Center (CAC) in Montreal, Quebec, Canada, a specialized clinic delivering services to SA children and their families recently implemented a protocol combining the AVI with the TF-CBT. This clinic was concerned about the clinical value of this combined intervention; whether it would lead to similar or better outcomes (i.e. less child behavior problems and less caregiver distress) than a regular TF-CBT protocol without a focus on the parent-child attachment relationship. Hence, in collaboration with this clinic, the current pilot study documented whether the combined TF-CBT/AVI intervention led to positive changes in SA children and their non-offending caregivers. We expected that SA children would show reductions in internalizing, externalizing, and dissociation symptoms following intervention from pre- to post-tests. We also hypothesized that non-offending parents would show diminished psychological distress and posttraumatic symptoms from pre- and post-tests. Results of this combined approach are interpreted in light of the results found in previous studies with SA preschoolers.
Method
Participants
The sample consisted of 33 SA children (10 boys and 23 girls; mean age: 4.79 years old, SD = 0.65), and their non-offending caregivers. Caregivers were the non-offending parental figures and included mothers (69.7%), fathers (15.2%), grandmothers or foster care mothers (15.1%). All families were recruited at the CAC situated in Montreal. To participate in this study, children had to be aged between 4 and 6 years old, had to have disclosed sexual abuse and be eligible to services at the CAC. Participants were referred to the CAC for treatment by Child Protective Services agencies. Information gathered from clinical records indicated that, on average, children began the intervention 11.19 months (SD = 6.34) following the disclosure of the abuse. Regarding additional services, information gathered at post-test indicated that 84.8% of participants did not benefit from other professional services. For the minority of children (15.2%) receiving other services, these services involved sessions with a social worker, psycho-educator or psychologist.
Procedures
The intervention protocol
TF-CBT is a therapeutic intervention that aims to reduce trauma symptoms in youth. The approach involves different components summarized by the PPRACTICE acronym (Cohen et al., 2011). Components thus include
The CAC implemented the TF-CBT in 2006 after the clinicians had been trained by one of the original authors of the approach (E. Deblinger). Recently, to better respond to the needs of preschool children, the CAC added the video-feedback component of the AVI intervention (Moss et al., 2011) to the TF-CBT protocol for children of this group age. The AVI was designed to improve parental sensitivity and child attachment security to the caregiver. In particular, the AVI uses video-feedback. At each AVI session, the clinician films the parent and the child during a semi-structured play (approximately 10 min.). Specific prompts are given to the parent and activities are chosen for the dyad in line with relationship difficulties. After the play, the parent watches the film sequences and the clinician intentionally stops the video during positive moments to reinforce parental sensitive behaviors and parental positive impact on the child. The clinician also enquires about the parent’s feelings and thoughts, and invites the parent to share observations related to the self, the child, and their relationship (Cyr et al., 2012). Moss et al. (2011) have showed that eight, one per week-session protocol increases maternal sensitivity and child attachment security.
For the current study sample, the video-feedback component of the AVI was embedded in the TF-CBT protocol starting session #3. At that session, a 10-minute interaction was filmed during which the mother and child were asked to play as they would normally do. Then, at following sessions, specific prompts in line with the dyad’s relationship difficulties were given to the parent during their filmed interaction. The mother received video feedback from the clinician the following week, which added an approximately 30 min. to the TF-CBT session. TF-CBT components continued to be addressed as planned but content sessions of the TF-CBT were adapted to child’s age. For instance, clinicians spent less time educating young children on their psychosexual development, they made greater use of pictograms and games. Children also spent less time building their trauma narrative given their lower attention span.
A total of 13 clinicians, trained in both the TF-CBT and AVI interventions, administered this combined approach according to the general principles and guidelines described in each manual. Overall, a rounded mean of 12 TF-CBT/AVI sessions (M = 12.06, SD = 4.23) were completed by families. The number of sessions in which AVI was used varied in accordance to the needs of each dyad. All sessions were delivered at the CAC.
Pre-post-tests
During their first visit at the CAC, parents were approached to participate to the research project. The project was explained to caregivers and those who agreed to participation signed a consent form. A pretest visit was scheduled at the clinic by the research team during which parents were invited to complete the questionnaires. Research assistants were available to answer participants’ questions and assist them if needed. Approximately 2 weeks after the intervention, participants were invited to complete the questionnaires for a second time at a post-test visit. This project was approved by the ethical committee of Ste-Justine Hospital and Université du Québec à Montréal.
Measures
Sociodemographic at pretest only
A sociodemographic questionnaire was completed by the caregiver to collect information such as ethnicity, family structure, parents’ occupation, education level and annual family income. This questionnaire also comprised questions on the mothers’ history of SA.
History of victimization form at pretest only
Characteristics of the abuse were collected from the children’s clinical records based on an adaptation of the History of Victimization Form (Wolfe et al., 1987). Information related to the identity of the perpetrator (e.g. member of the immediate or extended family or other known perpetrator), and the severity (clothed touching, unclothed touching, penetration or attempted penetration) and duration (one episode, few episodes or chronic abuse over a 6 months period or more) of SA were coded.
Child behavior checklist (CBCL) at pre- and post-tests
Caregivers were invited to assess the presence of child internalizing (anxiety, depression, somatization) and externalizing (e.g., aggression) behavior problems using the age-appropriate version of the CBCL (Achenbach & Rescorla, 2000, 2001). Items are answered on a 3-point Likert scale assessing the frequency of the behavior (0 = not true, 1 = somewhat or sometimes true, 2 = very true or often true). T-scores, normalizing for child gender and age, greater than 63 indicate scores above the clinical threshold. T-scores were calculated for internalizing behavior problems (36 items in the preschool version and 32 items in the school-age version) and externalizing behavior problems (24 items in the preschool version and 35 items in the school-age version) with higher scores reflecting higher level of behavior problems. The internal consistency scores for this sample were as follow: internalizing scale α = .69 and .65; externalizing scale α = .83 and .49 for the preschool and school-age versions, respectively.
Child dissociative checklist at pre- and post-tests
Caregivers completed the Child Dissociative Checklist (CDC; Bernstein & Putnam, 1986), a 20-item questionnaire. It evaluates the frequency of child dissociative experiences (e.g. derealization or depersonalization) on a 3-point Likert scale (0 = not true, 1 = somewhat or sometimes true, 2 = very true or often true). The scores range between 0 and 40 with higher scores showing a higher level of dissociation. Scores greater than 12 are above the clinical threshold. The internal consistency of this scale for this sample was high (α = .83).
Parental psychological distress at pre- and post-tests
Parental psychological distress was evaluated by the parent with the short form of the Indice de détresse psychologique (Index of Psychological Distress by Préville et al., 1992). It comprises 14 items on a Likert scale (0 = never, 1 = somewhat or sometimes true, 2 = often true, 3 = very true) and assesses the respondent irritability, anxiety, distress and potential cognitive problems. The global psychological distress score varies between 0 and 100. The clinical cut-off scores are established considering age and gender of respondents and correspond to scores above the 80th percentile. Higher scores reflect greater distress. The internal consistency score of this scale for this sample was high (α = .90).
Parental symptoms of posttraumatic stress at pre- and post-tests
Parents’ symptoms of posttraumatic stress following the disclosure of their child’s abuse were assessed using the Modified PTSD Symptom Scale, Self-Report (MPSS-SR) (Falsetti et al., 1993; translated by Guay et al., 2002). This 17-item questionnaire evaluated both the frequency and severity of current PTSD symptoms. It represents symptoms from the DSM-IV Posttraumatic Stress Disorder diagnosis and has been validated in samples experiencing a wide range of traumatic events. Scores range from 0 to 119 with higher scores reflecting greater PTSD symptoms. Scores greater than 49 are above the clinical threshold. The internal consistency score of this scale for this sample was high (α = .97).
Data analytic plan
Analyses were run with SPSS 27. First, descriptive statistics were conducted on the sociodemographic characteristics of the sample as well as for the characteristics of the sexual abuse experiences (severity, identity of perpetrator, duration of abuse). Second, paired t-tests were computed to examine for possible differences in levels of child symptoms (externalizing problems, internalizing problems and dissociation symptoms) and parental symptoms (psychological distress and posttraumatic symptoms) between the pre- and post-tests. McNemar analyses were also conducted to test whether the percentage of participants reaching clinical levels on child and parental symptoms decreased following the intervention. Effect sizes were computed and interpreted according to Cohen’s d criteria, where d = 0.2 is a small effect, 0.5 a moderate effect, and 0.8 a large effect size (Cohen, 1992).
Results
Descriptive statistics
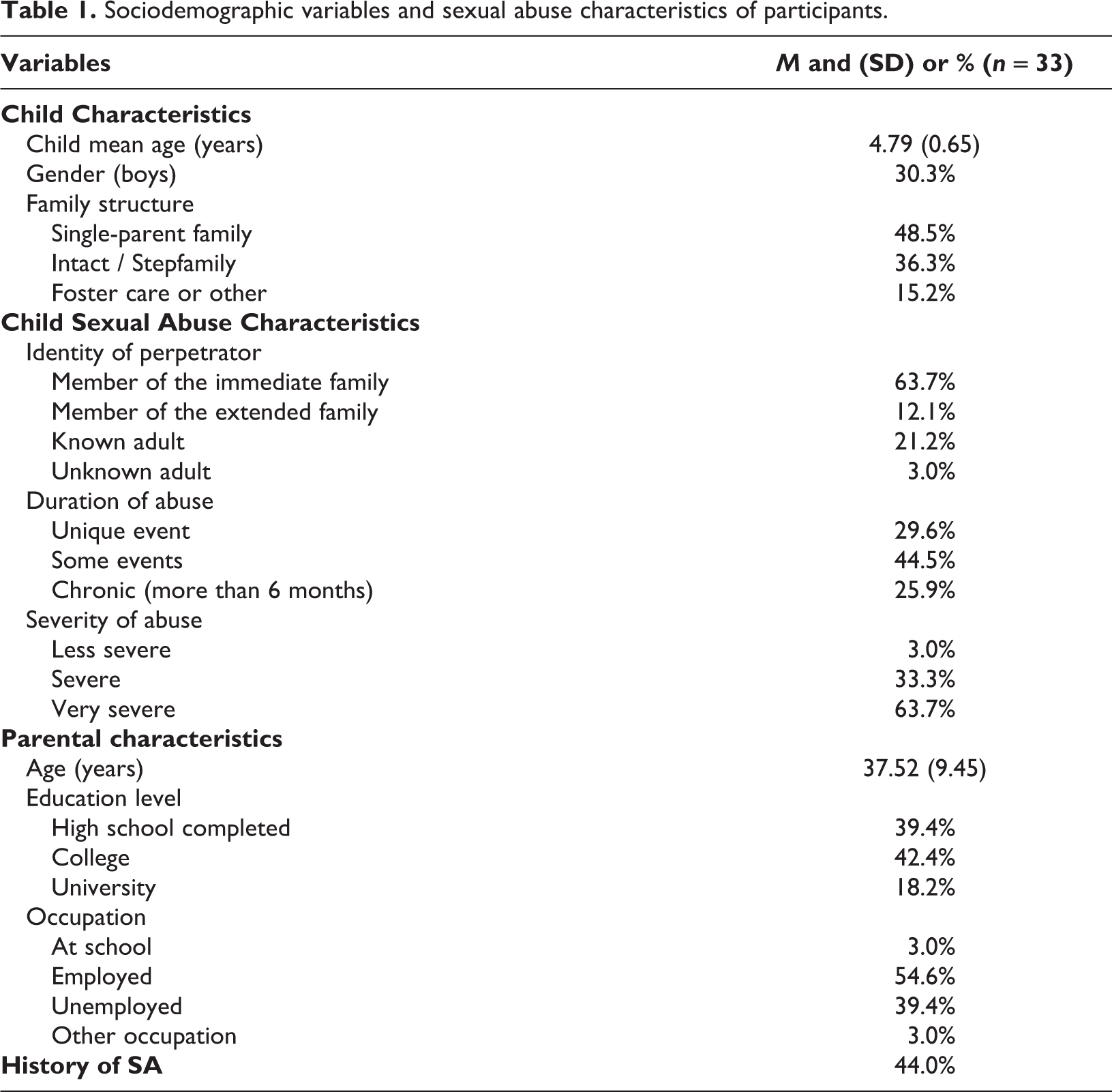
Table 1 presents the sociodemographic characteristics and the abuse-related variables for the whole sample. More than half of the children (63.7%) were sexually abused by a member of their immediate family. More than two thirds of the children (70.4%) suffered more than one event of sexual abuse and the vast majority (97%) went through severe or very severe forms of abuse such as attempts of penetration, penetration, or oral contacts. Most participating caregivers (81.8%) had completed a high school or college degree, and a little more than half (54.6%) of them were employed. Findings also revealed that 44.0% of the caregivers reported experiencing sexual abuse in their childhood.
Sociodemographic variables and sexual abuse characteristics of participants.
Analyses of the parental and child changes between the pre- and post-tests
Child symptoms
Means and standard deviations of child symptoms are presented in Table 2. Results of a paired t-test revealed a significant reduction of internalizing behavior problems following the intervention (t(30) = 2.90, p < .01, d = 0.52). A paired t-test also showed that mean scores for children’s dissociative symptoms significantly decreased from pretest to post-test (t(32) = 2.60, p < .05, d = 0.45). Effect sizes for these outcomes can be qualified respectively as moderate and small. There was no significant reduction for child externalizing problems (t(30) = 1.36, p = 0.19, d = 0.24).
Paired T-tests on children and parental figures outcomes from pre- to post-test.
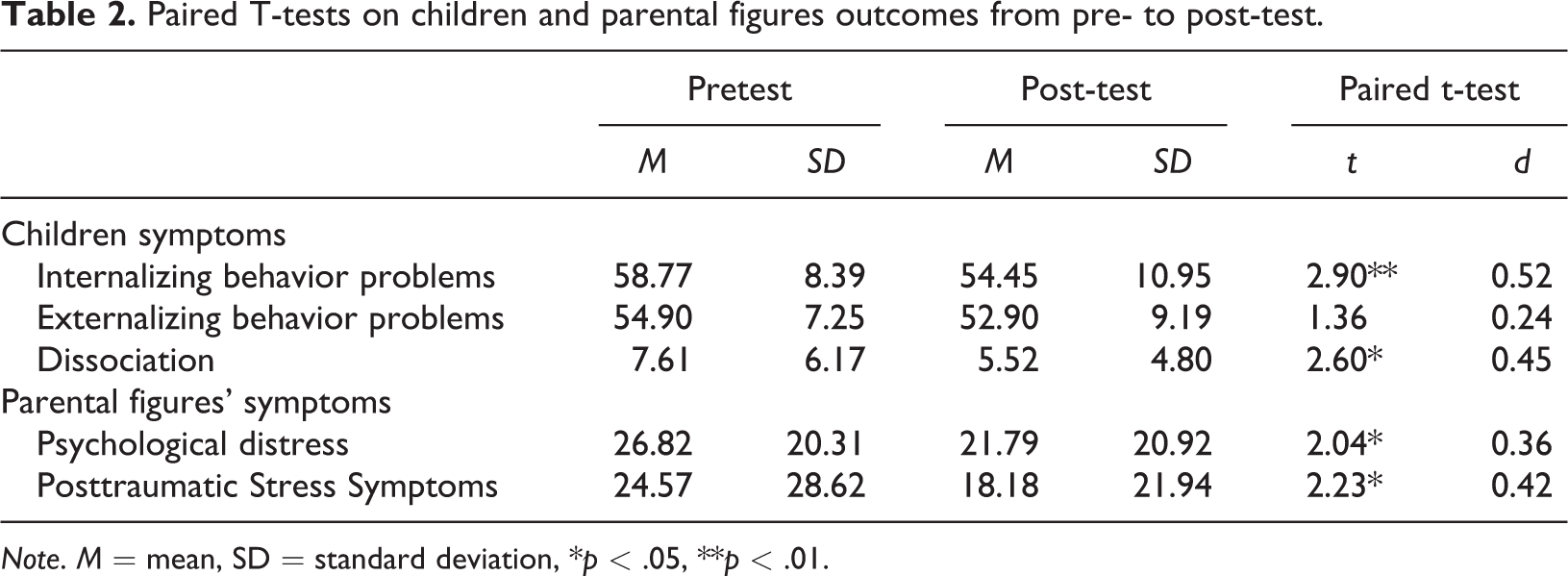
Note. M = mean, SD = standard deviation, *p < .05, **p < .01.
Caregiver symptoms
Results of a paired t-test indicated that maternal psychological distress decreased from pretest to post-test (t(32) = 2.04, p = .05, d = 0.36). Similar findings were obtained with caregivers’ symptoms of posttraumatic stress which diminished from pretest to post-test (t(27) = 2.23, p = .04, d = 0.42). Both results show small effect sizes.
Changes in clinical status
Results of a McNemar analysis showed a significant decrease in the percentages of children with clinical levels of internalizing problems between the pretest 32.3% and post-test 12.9% (p = .03). No significant changes in percentages of children with clinical levels of externalizing problems (pretest = 12.9%, post-test = 12.9%, p = 1.00) or dissociative symptoms (pretest = 18.2%, post-test = 9.1%, p = .38) were observed. As well, McNemar analyses on parental outcomes revealed no significant differences in the percentages of parents with clinical levels of PSTD symptoms (pretest and post-test = 10.7%) or psychological distress (pretest = 39.4%, post-test = 33.3%, p = .63).
Discussion
This pilot study explored the value of the TF-CBT combined with the AVI for SA preschool-age children and their non-offending caregivers receiving services at a Child Advocacy Center. The primary goal of this study was to evaluate whether this newly combined protocol, oriented on both the child’s trauma and the child attachment to parent relationship, 1) led to significant changes in child and parental symptoms after the intervention, and 2) if effect sizes of these outcomes were similar or stronger, according to Cohen’s criteria, than those obtained in a previous study with SA preschoolers only exposed to the TF-CBT protocol. Overall, results of this study showed positive changes for caregivers and their children. This pilot study could then be seen as a first step in the evaluation of an innovative combined protocol for the recovery of SA preschool children. Given that SA children are also likely to show insecure and disorganized attachments (Charest et al., 2019; Ensink et al., 2020), this approach is promising to foster positive adaptation despite severe adverse experiences at an early age.
Our study focused on a population of young children and, notwithstanding their young age, the majority of them were victims of severe sexual abuse involving penetration or attempted penetration. Furthermore, over 25% of the children were victims of multiple and chronic episodes of SA, spanning over a period of 6 months or more. Moreover, the majority of the children were abused by a member of their immediate or extended family. An important proportion of the children showed clinical symptoms, especially internalizing problems (32.3%). Fewer children showed clinical levels of externalizing (12.9%) or dissociative symptoms (18.2%). As well, a fair proportion of the mothers showed clinical levels of psychological distress (39.4%), although fewer mothers presented clinical levels of PTSD (10.7%). These data support the need of further studying post-trauma adaptation for this population using state-of-the-art designs, such as randomized control trials, to properly test the efficacy of treatment protocols facilitating the recovery of young victims. Given the lack of intervention studies with this population, our pilot study is a step in that direction.
Changes in child outcomes
As expected, results revealed significant changes in children’s internalizing and dissociative symptoms over the course of the intervention. These findings echo previous studies supporting the TF-CBT as a successful approach to decrease such symptoms (de Arellano et al., 2014; Deblinger et al., 2006; Hébert & Daignault, 2014). Throughout the intervention process, the child is brought to talk about the traumatic elements associated with the SA in a secure environment with trained clinicians. During sessions, children develop emotion regulation competencies (to address, name and regulate emotions) as a means to promote healthy ways of addressing the traumatic event. Perhaps because of the therapist’s attachment lens, the parent’s role in rebuilding a trust relationship with the child was emphasized during the therapeutic process. The parent’s increased availability toward the child’s emotional and attachment needs during the sessions may have contributed to the reduction of symptoms. By addressing both the child’s trauma and attachment relationship to the parent, the child may restore or develop trust in the care of their parent, helping reducing child symptoms. This is consistent with Bolen and Lamb’s (2007) study who showed that improvements in parenting practices are associated with decreases in posttraumatic symptoms in SA children. It is also in line with Moss et al.’s (2011) intervention study who showed decreases in child internalizing problems for maltreated children following the AVI.
However, results on child externalizing problems revealed that there were no significant changes in the levels of these symptoms after the intervention. These results are contrary to those of Moss et al.’s AVI who reported less child externalizing behavior problems at post-test. However, in the Moss et al. study, reduced levels of behaviors problems were only found for the oldest preschoolers of their sample. Also, very few SA children were included in the Moss et al. study, the majority being physically abused or neglected. Our lack of results on child externalizing problems could also be due to the trauma narrative that was completed by children in our sample. Deblinger et al. (2011) reported less behavior problems in children who were exposed to varying lengths of the TF-CBT protocol that did not include a trauma narrative component in comparison to children exposed to varying lengths of the TF-CBT protocol including such a narrative component. Authors argued that parents in the no-trauma narrative conditions (a condition similar to the AVI intervention) devoted more time to the parent training component which may have resulted in less child behavior problems. This may suggest that the trauma narrative may not be as useful for very young children as for school-age children and that the parent training component is crucial for younger children.
Changes in caregivers’ outcomes
The present study indicates that non-offending parents showed lower levels of psychological distress and posttraumatic stress symptoms following the intervention. These results are consistent with previous TF-CBT studies on post-trauma outcomes in non-offending parents of preschool SA children (Hébert & Daignault, 2014). In particular, the clinician, relying on principles of the AVI, provided positive feedback to the parents about their caregiving practices toward the child, which may have helped decrease parental levels of distress. SA children face a plethora of difficulties following the traumatic event (e.g., posttraumatic stress, behavior problems, dissociation, sleep problems) and such symptoms, in addition to the abuse event itself, are overwhelming for the parent who may find it very difficult to deal with this whole situation. Non-offending parents often describe the unveiling of the abuse as a shock (Elliott & Carnes, 2001), which comes with many long-lasting significant challenges. Feelings of anger, helplessness, and despair are often observed in parents, who may become doubtful about their capacities to help their child through these difficult times. As portrayed in several studies, the psychological impact on parents is considerable, as clinical depression and posttraumatic stress disorders have been observed in parents of SA children, and these problems can last as long as 1 year after the disclosure (Cyr et al., 2018).
Overwhelming feelings and clinical symptoms may even be more intense when the parent has been sexually abused in their own childhood (Daignault et al., 2017). In the current study, the prevalence of the caregivers with a history of sexual abuse reached 44%. Parent survivors of SA often have not disclosed their own abuse or did not have access to therapeutic services. This may increase their level of psychological distress. In our study, 39.4% of the caregivers reported clinical levels of psychological distress. Disclosure of the abuse by their child may also trigger past memories of their own abuse, which might reactivate symptoms including flashbacks and the re-experiencing of symptoms, which is characteristic of individuals with PTSD. Although caregivers showed PTSD symptoms and distress at the beginning of intervention, they reported significantly less of these symptoms following the intervention. To help with the development of a secure attachment relationship, the AVI highlights to the parent their sensitive behaviors, further helping them to use these behaviors a means to repair their relationship with the child. As previously reported by caregivers exposed to the AVI, this intervention has helped them regain confidence in their parental sense of competency toward the child, which could explain the decreases in psychological distress (Moss et al., 2014). Furthermore, as mentioned by Cohen et al. (2006), even if TF-CBT is a child-focused therapy, the non-offending parent also participates in the sessions. This involvement may help them acquire strategies and skills to deal with distress.
Prior research evaluating the impact of TF-CBT in preschool and school-aged child victims of trauma (e.g. natural disasters, abuse and neglect, terrorism, etc.), reported using symptoms measures in child and caregivers such as posttraumatic stress symptoms, dissociation, behavior problems, psychological distress, global functioning and more (Mcguire et al., 2021). Given that the goal of this pilot study was to evaluate the potential benefits from a combined therapeutic approach in preschool-aged child victims of sexual abuse, we considered appropriate to rely on similar measures previously used in TF-CBT studies. The effect sizes found in one of our previous study with a different sample (Hébert & Daignault, 2014) showed the benefits of the TF-CBT in SA preschoolers. For symptoms such as child behavior problems and dissociation, effects sizes reached d = 0.89 for internalizing problems, d = 0.83 for externalizing problems and d = 1.07 for dissociation symptoms. For the parents’ psychological distress and posttraumatic stress, effects sizes reached d = 0.52 and d = 1.18, respectively. In the current study, effects sizes for internalizing and externalizing behavior problems and dissociation were d = 0.52, d = 0.24 and d = 0.45, respectively. Concerning the caregiver outcomes, effects sizes for psychological distress reached d = 0.36 and d = 0.42 for posttraumatic stress symptoms. Overall, effects sizes from the current study were all in the small to medium range, whereas those of our previous study not including the AVI were all large effect sizes. These differences in effect sizes may however be due to the higher levels of problems of children and parents in the Hébert and Daignault (2014) study. The combined approach intervention (TF-CBT + AVI) proposed in the current study is the first of its kind to be studied, and while its’ effects may not be as stronger than those reported in the Hébert and Daignault (2014) study, significant child and parental improvements were observed. At the moment, as reported in a systematic review of the TF-CBT for traumatized preschoolers, the TF-CBT is considered “probably efficacious” (McGuire et al., 2021). The changes observed in our study suggest that a combined approach is a promising strategy.
S trengths and limitations of the present study
This study is the first to investigate the value of the combined TF-CBT/AVI intervention in a population of preschool-aged victims of SA. Despite its contribution, some limitations must be mentioned. First, the design of the study did not include a control group, precluding from any firm conclusions about the effects of the intervention. Many other confounding variables, such as the simple passage of time, may explain our study results. Nevertheless, our study, as mentioned earlier, is a first step toward the identification of a successful intervention strategy for SA preschoolers. Another limitation is that the study outcome data were solely based on parents reports, who may have been subjected to the caregiver’s social desirability. As well, the present sample has a very small sample size, which limited further analyses, such as moderator analyses.
Future studies should consider a randomized control trial design to clearly attribute the obtained effects to the intervention. As well, future studies should conduct assessment of implementation issues, such as the fidelity with which principles of the intervention were followed by clinicians (whether the format of delivery, number of sessions, setting of delivery was as planned). Also, adding multiple assessment times would be important to ascertain the sustainability of therapeutic gains over time. As well, future research should include more participants to ensure statistical power when performing analysis on possible moderators (e.g., child gender, maternal presence and severity of past trauma) of treatment effects. Finally, outcomes, such as caregiver sensitivity, and attachment security, which are key outcomes in studies testing attachment-based interventions, were not assessed in the current project, and should be explored in future studies.
Conclusion
Despite limitations of this study, results indicate changes in parents’ and children’s levels of well-being. Such results are noteworthy from a clinical point of view. First, results suggest that the TF-CBT combined with the AVI may be successful in reducing internalizing and dissociation symptoms in preschool children victims of SA, as well as psychological distress and posttraumatic symptoms in caregivers. These findings indicate that an intervention oriented on both the child’s trauma and the parent-child attachment relationship may be well-suited in the treatment of child victims of SA. It also underscores the value of the non-offending caregiver in therapeutic process as a means to ameliorate, and perhaps even sustain, children’s recovery following sexual abuse. This pilot study tested the effects of a combined TF-CBT and AVI protocol for a population of SA preschool children. Further studies are now needed to replicate these findings with a randomized control trial design.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Chaire interuniversitaire Marie-Vincent sur les agressions sexuelles envers les enfants awarded to Martine Hébert. Financial support was also provided to Martine Hébert and Chantal Cyr by the Canada Research Chairs Program.